Clinical Pharmaceutical Reasoning in Hospital Pharmacy Practice using the DRIP framework: a New Approach for a Perfectionist Profession
Heleen van der Sijs, Midas B. Mulder, Devi Prasad Mohapatra, Heleen van der Sijs, Sarah Alghanem, Heleen van der Sijs

TL;DR
This paper introduces the DRIP framework to improve clinical pharmaceutical reasoning in hospital pharmacy practice, helping perfectionist pharmacists manage uncertainty and enhance decision-making.
Contribution
The DRIP framework is a novel structured approach to teach and support clinical pharmaceutical reasoning in hospital settings.
Findings
Pharmacists using DRIP felt more confident in addressing complex pharmaceutical problems.
The framework helped pharmacists anticipate underlying issues in simple pharmaceutical questions.
The DRIP approach enables simultaneous training of several CANMEDS roles.
Abstract
Clinical pharmacists are responsible for safe medication use in hospitals. Most clinical pharmacists are perfectionists. However, in their decision-making process, they have to embrace uncertainty, while interpreting available data, and integrating knowledge and clinical experience. In clinical practice, how to teach and master clinical pharmaceutical reasoning is unclear. We developed the DRIP framework including different aspects on drug, indication and patient and a stepwise approach to support clinical pharmaceutical reasoning by students, residents in hospital pharmacy and clinical pharmacists. The DRIP framework was first introduced during the daily report with residents and faculty of the clinical pharmacy. The framework was implemented in daily clinical practice to handle drug safety alerts, and to optimise drug therapy during ward rounds, multidisciplinary consultations, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
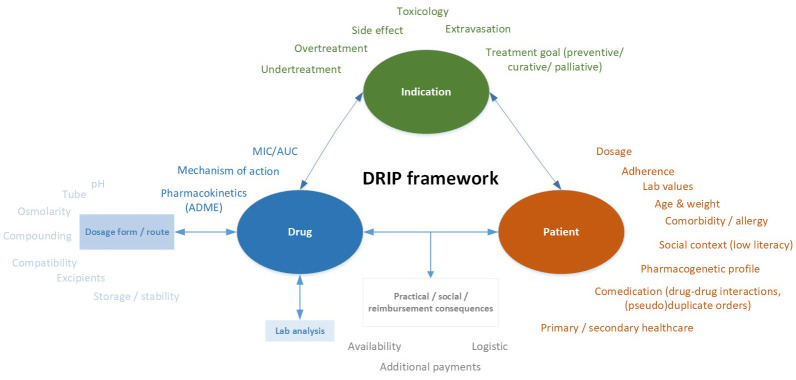 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPharmaceutical Practices and Patient Outcomes · Patient Safety and Medication Errors · Clinical Reasoning and Diagnostic Skills
Practice points
Clinical pharmacists are perfectionists that have to embrace uncertaintyHow to teach clinical pharmaceutical reasoning is unclearThe DRIP framework shows aspects of drug, indication and patient to considerThe accessory stepwise approach supports the clinical pharmaceutical reasoning process
Educational challenge
Clinical pharmacists are responsible for the safe use of medications in hospitals. Therefore, they are trained to be perfectionists to avoid risks associated with medication. Healthcare has become more complex over the years because of multimorbidity, polypharmacy, and shorter hospital stays of severely ill patients. Thus, clinical pharmacists must deal with guidelines that conflict with or are not applicable to patients at hand. Moreover, they have to accept and embrace complexity and uncertainty and weigh the risks and benefits using relevant context parameters in their decision-making process. Clinical pharmaceutical reasoning is defined as a context-dependent cognitive process whereby pharmacists apply and integrate knowledge and clinical experience to interpret the available clinical data ( Mertens et al., 2022).
Clinical pharmaceutical reasoning is often necessary when questions seem simple and straightforward, such as questions about the right dose, route of administration, or potential interaction between two or more drugs. In general, context parameters must be considered to formulate an adequate answer. For example, the rather simple question ‘Can this drug be administered through a feeding tube?’ generally requires more information on the patient, the reason for prescribing (indication or diagnosis), and the drug (regimen). How old is the patient, are there swallowing problems, and which administration form and dosing schedule are prescribed? The answer ‘no’ does not help the nurse or physician and will result in a follow-up question.
Thus, clinical pharmaceutical reasoning is of vital importance in clinical pharmacists’ daily practice, and this complex skill should be developed and taught. It is also a trust criterion for Dutch residents in clinical pharmacy to grant them entrustable professional activities (EPAs) ( Ten Cate & Hoff, 2017). Residents should not only demonstrate that an adequate answer has been given in a certain case but also how context-dependent risks and benefits are weighed with different context parameters in a so-called entrustment-based discussion. Thus, supervisors should be able to understand and express their own decision-making processes beyond their gut feelings. However, pharmacists lack training in clinical reasoning, as opposed to physicians, who are intensively trained in clinical diagnostic reasoning at medical schools ( Woodruff, 2019).
We recognized that pharmacy students and clinical pharmacy residents relied too much on published case reports, did not consider all relevant context parameters in their recommendations, and could not explain their reasoning. Moreover, supervisors do have difficulties in explaining their clinical decision-making process to students and residents.
What was the solution?
In 2021, we developed a framework for clinical pharmaceutical reasoning. This DRIP framework includes many relevant aspects of ** dr **ug, ** i **ndication, and ** p **atient that may influence the responses of clinical pharmacists to medication-related questions and tasks (See Figure 1). The framework is not comprehensive in that it can be used as a checklist/roadmap. It is merely a toolbox that should be used with adaptive capacity and professional values (e.g., accountability, moral integrity, trustfulness) ( Woodruff, 2019). With increasing complexity, people are inclined to use a reductionist standardized approach that is not applicable to complex systems. The framework may provide insight into unknown aspects that should be taken into consideration. Acknowledging and embracing this uncertainty may result in better clinical reasoning ( Stolper et al., 2021). The DRIP framework focuses on content, but this is not sufficient to support the clinical reasoning process that requires the integration of relevant data ( Mertens et al., 2022).
DRIP framework for clinical pharmaceutical reasoning.
To provide guidance in the clinical reasoning process, we developed a stepwise approach next to the DRIP framework, including the following steps: (a) summarize the medication problem/question, (b) map all relevant patient and drug characteristics and consult trustworthy information sources; (c) interpret lab values and patient parameters taking into account context, history, and comedication; (d) weigh the benefits and risks of possible solutions, including implications of stopping drugs on drug-drug interactions and therapeutic drug monitoring, (e) test for feasibility on practical, financial, social, and sustainability levels; (f) discuss the options with the healthcare professional, conclude and record in the patient file, and (g) follow-up and learning.
How was the solution implemented?
Our DRIP framework for clinical pharmaceutical reasoning has been introduced and used in our daily clinical pharmacy report. In case-based discussions during the daily report, questions were asked using the framework, for example, ‘What if the patient was pregnant or obese?’, or ‘What would you recommend if the intoxicated patient was seen within one hour of ingestion, or ingested sustained release tablets?’. Residents were invited to answer first and explain their clinical pharmaceutical reasoning process, but the questions also stimulated this process among faculty and pharmacy students. The framework was evaluated and did not require any adjustment. The printed DRIP framework was visible in the room for daily reporting and digitally linked to daily report meetings.
In addition to their use in daily reports, residents and consultant clinical pharmacists were encouraged to use this framework during their clinical activities and on-call shifts to serve clinics with well-considered recommendations. The framework was applied during the daily rounds on the wards, in multidisciplinary consultations, in one-to-one supervision of residents in handling drug safety alerts, in entrustment-based discussions with residents, and in the supervision of pharmacy students.
What lessons were learned that are relevant to a wider global audience?
By introducing the DRIP framework, our students, residents, and consultant clinical pharmacists were taught to provide a more holistic overview of the complexity of clinical pharmaceutical problems. We recognize that the DRIP framework may unveil unknown aspects and, consequently, whether the case is simple or complex ( Stolper et al., 2021). Consultant clinical pharmacists and senior residents said that they used the DRIP framework only for complex cases, and novices perceived it more often as helpful. The stepwise approach was mainly used by students and less experienced pharmacists. Although all the steps must be completed, the decision-making process is often not straightforward. Particularly in complex cases, the steps occur crisscrossing and iteratively arrive at the final recommendation ( Woodruff, 2019). However, using the stepwise approach ensures that all relevant steps are completed, including practical consequences to anticipate further questions and learning by performing follow-ups.
The most important lessons learned from the implementation of the DRIP framework for clinical pharmaceutical reasoning are as follows.
Pharmacists felt more confident that the relevant aspects of a difficult and complex pharmaceutical problem were considered.Pharmacists could better explain their reasoning process;Pharmacists learned to anticipate the issues behind the apparently simple pharmaceutical questions of healthcare workers or patients.
Furthermore, the DRIP framework appeared to be helpful in entrustment-based discussions by varying one or several aspects, and in the simultaneous training of the CanMEDS roles of communicator, collaborator, professional, and scholar.
What are the next steps?
The first step in developing a tool for clinical pharmaceutical reasoning in clinical pharmacy resulted in a well-received DRIP framework and an additional stepwise approach. Currently, we are developing a course for the national education program for residents of clinical pharmacies and their (deputy) trainers using the DRIP framework. As awareness of the lack of training of Dutch pharmacists in clinical pharmaceutical reasoning is growing, we have tried to build collaborations with other universities, teaching hospitals, and pharmacy schools in the Netherlands.
As prescribers may also benefit from the DRIP framework, and both physicians and pharmacists may learn from each other, we would like to expand to an interprofessional clinical pharmaceutical reasoning course for fellows of the Dutch Society for Clinical Pharmacology and Biopharmacy.
Ethics and consent
Ethical approval and consent were not required.
Disclaimer
The views expressed in this article are those of the authors. Publication in MedEdPublish does not imply endorsement by MedEdPublish.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mertens JF Koster ES Deneer VHM : Clinical reasoning by pharmacists: a scoping review. Curr Pharm Teach Learn. 2022;14(10):1326–1336. 10.1016/j.cptl.2022.09.011 36123233 · doi ↗ · pubmed ↗
- 2Stolper E Van Royen P Jack E : Embracing complexity with systems thinking in general practitioners’ clinical reasoning helps handling uncertainty. J Eval Clin Pract. 2021;27(5):1175–1181. 10.1111/jep.13549 33592677 PMC 8518614 · doi ↗ · pubmed ↗
- 3Ten Cate O Hoff RG : From case-based to entrustment-based discussions. Clin Teach. 2017;14(6):385–389. 10.1111/tct.12710 28971576 · doi ↗ · pubmed ↗
- 4Woodruff JN : Accounting for complexity in medical education: a model of adaptive behaviour in medicine. Med Educ. 2019;53(9):861–873. 10.1111/medu.13905 31106901 · doi ↗ · pubmed ↗