Meningococcal Purpura Fulminans: A Rare Presentation in an Adult Case of Serogroup W135 Infection
Usamah Al-Anbagi, Muayad K Ahmad, Mohamed G Mohamedali, Abdulrahman Saad, Marwa I Elaziz, Abdulqadir J Nashwan, Hatem M Abusriwil

TL;DR
This paper describes a rare case of meningococcal purpura fulminans in an adult with a W135 infection, emphasizing the importance of early diagnosis and treatment.
Contribution
The novelty lies in presenting an unusual adult case with non-typical early symptoms leading to severe complications.
Findings
The patient initially showed non-specific symptoms like sore throat before developing severe septic shock.
The case underscores the variability in clinical presentation of meningococcal purpura fulminans.
Aggressive treatment including antibiotics and intensive care was crucial for managing the condition.
Abstract
Meningococcal purpura fulminans is a rare but serious complication of invasive Neisseria meningitidis infection, marked by widespread clotting problems and skin tissue death. Diagnosis can be tricky, especially when patients show unusual early symptoms that do not fit the classic pattern. We present an adult case infected with serogroup W135 who initially had non-specific symptoms such as sore throat, which progressed quickly to severe septic shock and purpura fulminans. The patient required intensive care and tailored treatments, including antibiotics and supportive care. This case highlights how varied the presentation can be and stresses the need for early recognition and aggressive management to improve outcomes and prevent lasting damage.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
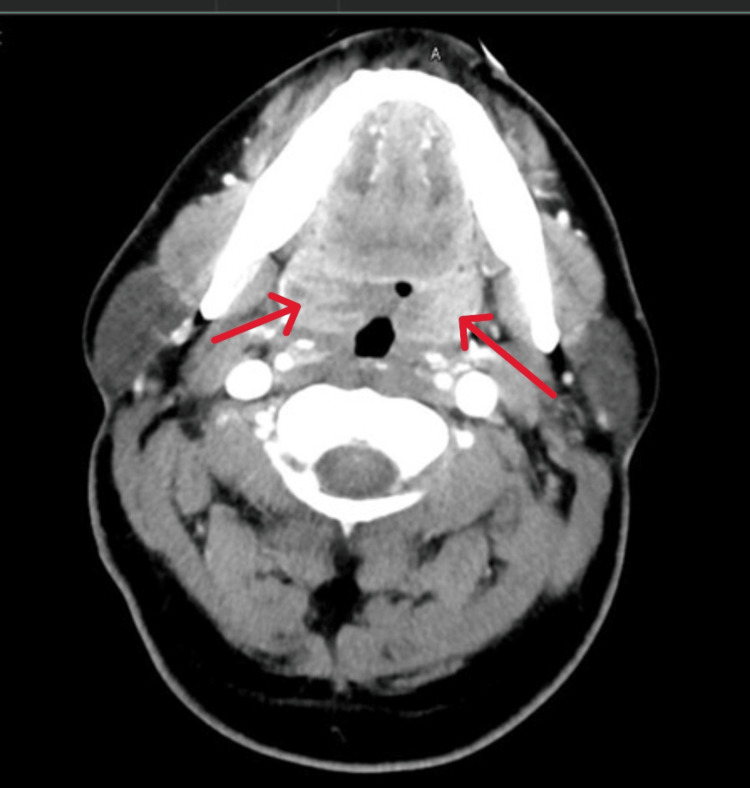 Figure 1
Figure 1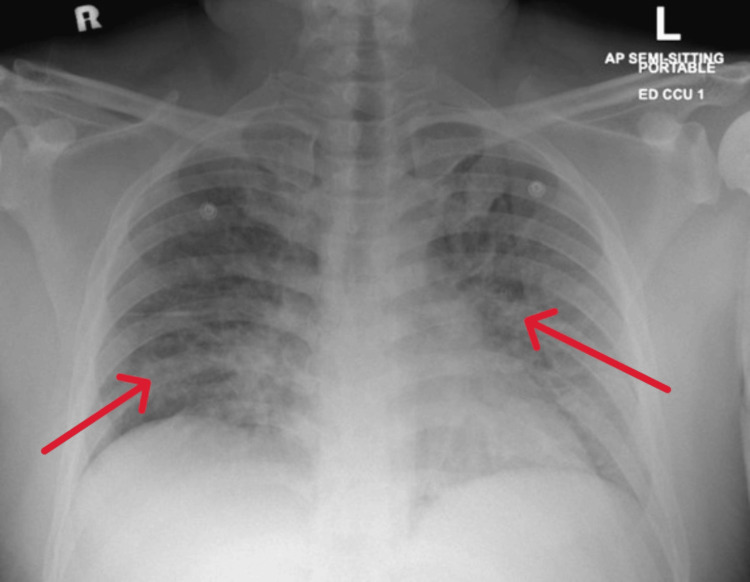 Figure 2
Figure 2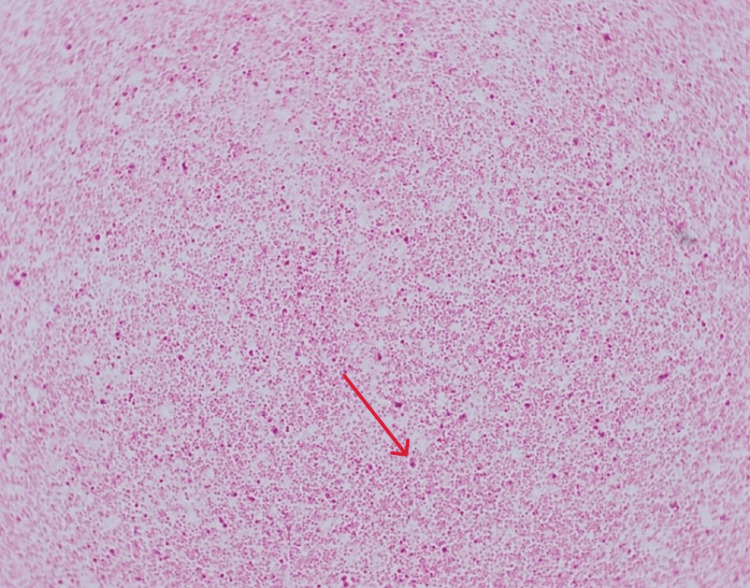 Figure 3
Figure 3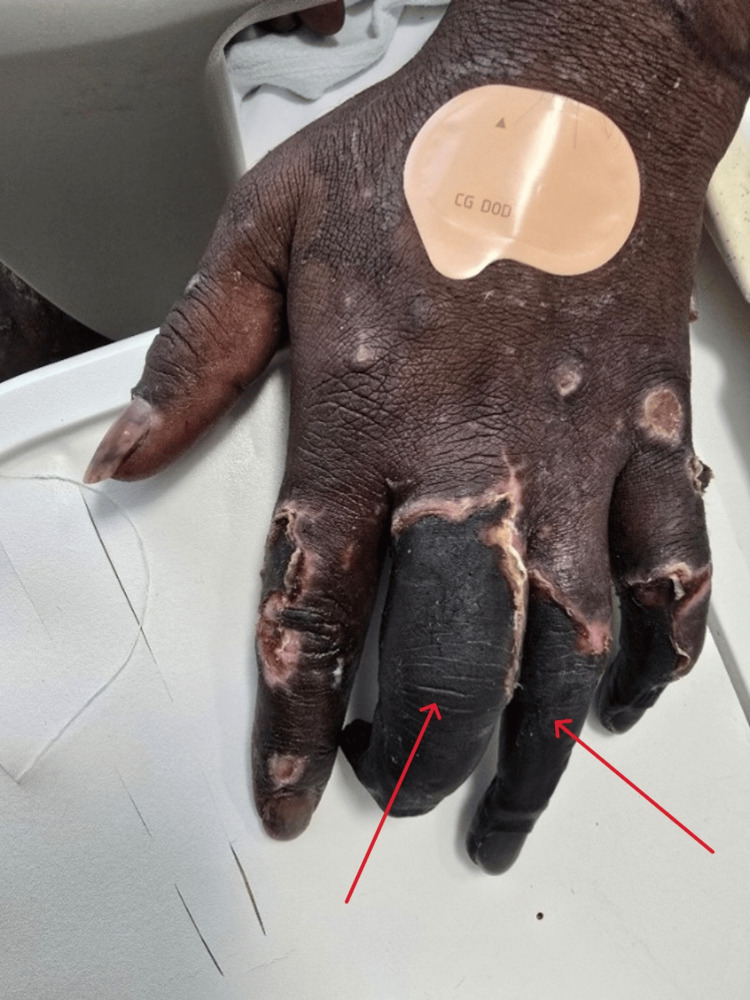 Figure 4
Figure 4 Figure 5
Figure 5| Parameter | On Admission | On Discharge | Normal Values |
| WBC | 18.3 | 7.5 | 6.2 × 10³/μL |
| Hb | 16.1 | 12.1 | 13-17 g/dL |
| Plt | 33 | 294 | 150-410 × 10³/μL |
| CRP | 179 | 14.4 | 0-5 mg/L |
| PCT | >100 | 0.7 | < 0.05 ng/mL |
| Urea | 5.8 | 3.5 | 2.5-7.8 mmol/L |
| Creatinine | 255 | 55 | 62-106 μmol/L |
| K⁺ | 2.8 | 4.0 | 3.5-5.3 mmol/L |
| Na⁺ | 131 | 129 | 133-146 mmol/L |
| Total Protein | 60 | 87 | 60-80 g/L |
| Albumin | 31 | 30 | 35-50 g/L |
| ALT | 67 | 58 | 0-41 IU/L |
| AST | 58 | 44 | 0-41 IU/L |
| ALP | 168 | 199 | 40-129 U/L |
| Bilirubin | 38 | 17 | 0-21 μmol/L |
| PT | 22.9 | 15.0 | 9.4-12.5 s |
| INR | 2.0 | 1.4 | < 1.0 |
| APTT | 64.4 | 109.0 | 25.1-36.5 s |
| DD | 125.9 | Not tested | 0-0.5 mg/L FEU* |
| Troponin | 20 | Not tested | 3-15 ng/L |
| CK | 3025 | 47 | 39-308 U/L |
| Myoglobin | 3405 | Not tested | 28-72 ng/mL |
| Lactatic acid | 13.4 | Not tested | 0.5-2.2 mmol/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBacterial Infections and Vaccines · Virology and Viral Diseases · Influenza Virus Research Studies
Introduction
Meningococcal disease is a major public health concern worldwide, associated with high morbidity and mortality, particularly in children and young adults. Neisseria meningitidis, a Gram-negative diplococcus, is responsible for invasive infections that may present as meningitis or fulminant septicemia, often leading to devastating complications, including shock, disseminated intravascular coagulation (DIC), and purpura fulminans [1-3]. Outbreaks and sporadic cases continue to occur globally, with epidemiological variations across regions and serogroups [4,5].
Purpura fulminans is a rare but life-threatening complication of severe sepsis, characterized by rapidly progressive purpuric skin lesions, vascular thrombosis, and DIC [6,7]. It results from dysregulation of the coagulation system, often related to deficiencies in natural anticoagulant pathways, such as protein C, protein S, or antithrombin III [8-11]. Clinically, it manifests with hemorrhagic infarction of the skin and may progress to extensive necrosis requiring surgical intervention or even limb amputation [12,13].
Although purpura fulminans has been described in association with several infectious agents, meningococcal septicemia remains one of the most important causes, and timely recognition is critical to reduce mortality [10]. We present a case of meningococcal septicemia complicated by purpura fulminans in an adult patient.
Case presentation
History
A previously healthy 36-year-old Indian man presented with a four-day history of gradual onset of fever, headache, generalized body aches, sore throat, and a noticeable change in voice. Over the preceding two days prior to admission, he developed difficulty swallowing along with bilateral upper neck pain. He denied cough, shortness of breath, chest pain, abdominal pain, vomiting, diarrhea, dysuria, skin rash, or recent travel. Family history was unremarkable. The patient denied any recent use of herbal, illicit, or over-the-counter medications. He is a non-smoker. There was no history of contact with individuals who were sick or had a prior history of similar illnesses.
Examination
On examination, he was conscious, alert, and oriented, with a Glasgow Coma Scale 14 of 15 (eye opening: 4/4, verbal response: 4/5, motor response: 6/6) [14], but appeared dehydrated, irritable, and hypotensive with a blood pressure of 101/39 mmHg, tachycardia at 133 bpm, respiratory rate of 22, temperature of 38.7 °C, and oxygen saturation of 97% on room air. His pharynx was markedly congested with enlarged tonsils nearly obstructing the airway. Chest examination revealed good bilateral air entry with normal breath sounds, and cardiovascular examination showed normal heart sounds with no murmurs or added sounds. The abdomen was soft, non-distended, and non-tender, with no organomegaly or guarding. There was no costovertebral angle tenderness, peripheral edema, or meningeal signs. Skin examination revealed no rash, petechiae, or purpura at presentation. Cranial nerves and motor-sensory examinations were intact, and there was no focal neurological deficit.
Investigation and treatment
Laboratory workup revealed leukocytosis, thrombocytopenia, elevated creatinine, low potassium levels, metabolic acidosis, markedly elevated inflammatory markers, deranged liver enzymes, and very high CK, myoglobin, and DIC parameters (Table 1).
CT of the neck showed diffuse adenoidal and tonsillar enlargement without abscess formation (Figure 1), and chest X-ray revealed bilateral infiltrates (Figure 2).
CT neck, axial view, revealed diffuse tonsillar enhancement and enlargement (red arrows)CT: Computerized tomography
Chest X-ray, PA view, revealed bilateral infiltration (red arrows)PA: posteroanterior
He was admitted as a case of tonsillitis with sepsis, but soon deteriorated, requiring vasopressors with noradrenaline. He became drowsy with declining consciousness and was subsequently intubated. Blood cultures returned positive for *N. meningitidis *serogroup W135 (Figure 3), leading to a revised diagnosis of meningococcemia with meningitis, septic shock, rhabdomyolysis, and acute kidney injury.
Gram-negative diplococci observed on direct Gram stain of a positive blood culture (red arrow)
Ceftriaxone was escalated to 2 g twice daily for 10 days, as per infectious disease advice. Despite improving labs and clearance of bacteremia, he remained critically ill on mechanical ventilation and vasopressors, prompting escalation to meropenem. He was extubated after five days, but by day four developed small necrotic lesions on his hand and foot (Figure 4), rapidly progressing to gangrene involving fingers, toes, arms, legs, buttocks, and perioral regions (Figure 5).
Areas of necrosis, ulceration, and black discoloration affecting primarily the middle and ring fingers, consistent with purpura fulminans (red arrows)
Multiple well-demarcated necrotic ulcers with dark eschar centers and erythematous-violaceous borders, consistent with purpura fulminans (red arrows)
Antibiotics were later (after stabilization) de-escalated to ceftriaxone, and wound care with topical glyceryl trinitrate was initiated under the guidance of vascular and dermatology specialists. He was completely hemodynamically stable, with vital signs and blood pressure maintained within normal limits. The patient remained afebrile, with oxygen saturation maintained on room air. He was mobile, fully conscious, and oriented. Despite progressive gangrene, his overall condition stabilized. After a 30-day hospitalization, he opted to discharge himself against medical advice to return to his home country for continued rehabilitation.
Discussion
N. meningitidis remains a leading cause of bacterial meningitis and septicemia worldwide, disproportionately affecting children and young adults. In the United States, the annual incidence ranges from 0.5 to 1.5 per 100,000, with serogroups B, C, and Y predominating, while serogroup W135 has caused notable outbreaks associated with travel to the Middle East [1]. Mortality still hovers around 10-15% even in well-resourced settings, largely due to the organism’s propensity for rapid progression to septic shock and multiorgan failure [2]. This case illustrates the often deceptive clinical spectrum of invasive meningococcal disease, particularly when it presents with upper respiratory symptoms instead of the classic triad of fever, rash, and meningismus. The patient began with pharyngitis, odynophagia, and voice change, misleading clinicians toward a local ENT infection, when in fact it heralded meningococcemia. These atypical features can contribute to diagnostic delays that prove fatal without early empiric therapy [3-5].
Purpura fulminans is a rare but catastrophic complication characterized by DIC with extensive microvascular thrombosis and hemorrhagic skin necrosis. It typically presents as rapidly evolving retiform purpura with irregular, branched, or angular lesions (6), as was evident in this case. This syndrome is generally classified into hereditary and acquired forms. The hereditary type most often results from homozygous protein C deficiency, typically manifesting in neonates with severe purpura and thrombosis, while heterozygous individuals usually develop venous thromboembolism without DIC [6]. The acquired form is frequently linked to overwhelming infections such as meningococcemia, where a strong inflammatory response drives excessive tissue factor expression and the release of procoagulant microparticles, leading to widespread coagulation activation [6].
Clinically, purpura fulminans is recognized by its abrupt onset of thrombotic DIC with characteristic skin findings, and while biopsy is seldom required, it can sometimes be performed to confirm the diagnosis [6]. Regardless of cause, purpura fulminans follows a shared pathway involving reduced protein C levels or activity, which promotes unchecked clot formation [7]. In severe sepsis, the widespread inflammatory response activates coagulation and complement systems and damages the endothelium. Cytokines such as interleukin-1 and TNF-alpha suppress the production of protein C, protein S, and antithrombin while boosting prothrombotic factors such as factor VIII and fibrinogen [8]. Normally, activated protein C helps regulate clotting and inflammation by stabilizing the endothelium and downregulating pro-inflammatory signals, but its depletion in sepsis exacerbates microvascular thrombosis. This leads to consumption of platelets and clotting factors, paradoxically increasing bleeding risk [8]. Early skin lesions show small vessel blockage and capillary congestion; later stages demonstrate irreversible endothelial damage, dermal hemorrhage, and necrosis [9]. Ultimately, the loss of natural anticoagulants fosters more clotting, impairs fibrinolysis, and sustains inflammation [10].
Early recognition of sepsis-associated purpura fulminans is crucial, as prompt intervention can sometimes halt progression [4,11]. Management centers on rapidly controlling infection with antibiotics, supporting circulation and oxygenation, and correcting coagulation imbalances. Fresh frozen plasma or protein C concentrate is used to restore depleted clotting regulators [12]. Due to protein C’s short half-life, repeated doses are often needed. When bleeding is significant, platelet or cryoprecipitate transfusions may also be required [11]. Unfortunately, once tissue necrosis is established, surgical interventions such as debridement, fasciotomy, or amputation frequently become necessary [13].
Purpura fulminans lesions often advance within 24-48 hours to deep skin or soft-tissue necrosis, requiring weeks to heal and commonly leaving extensive scarring [13]. Without timely treatment, these areas can become gangrenous, sometimes necessitating limb amputation. The condition often involves microvascular thrombosis in organs such as the lungs, kidneys, brain, and adrenal glands, driving multi-organ failure, high early mortality, and long-term disability [13]. Inherited cases with protein C deficiency are prone to recurrent thrombotic events, and surviving infants may suffer neurological or visual impairment. New lesions may continue to appear for up to two weeks in post-infectious cases [15].
Conclusions
In conclusion, this case highlights the wide-ranging and sometimes misleading presentations of meningococcal disease, from pharyngeal symptoms to severe purpura fulminans. It underscores the importance of maintaining a high level of clinical suspicion, initiating prompt broad-spectrum antibiotic therapy, and managing complications aggressively to improve outcomes. Moreover, this case serves as a reminder of the critical role of vaccination and robust public health strategies in preventing this potentially fatal yet largely avoidable infection.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global epidemiology of invasive meningococcal disease Popul Health Metr Jafri RZ Ali A Messonnier NE 1711201310.1186/1478-7954-11-17PMC 384879924016339 · doi ↗ · pubmed ↗
- 2Sepsis and septic shock N Engl J Med Meyer NJ Prescott HC 21332146391202410.1056/NEJ Mra 240321339774315 · doi ↗ · pubmed ↗
- 3Global epidemiology of meningococcal disease Vaccine Harrison LH Trotter CL Ramsay ME 06327200910.1016/j.vaccine.2009.04.06319477562 · doi ↗ · pubmed ↗
- 4A cluster of meningococcal serogroup W 135 infections: a case series Cureus Al-Anbagi U Al Maslamani M Al-Khal A 017202510.7759/cureus.80747 PMC 1200403140248523 · doi ↗ · pubmed ↗
- 5Increase in endemic Neisseria meningitidis capsular group W sequence type 11 complex associated with severe invasive disease in England and Wales Clin Infect Dis Ladhani SN Beebeejaun K Lucidarme J 57858560201510.1093/cid/ciu 88125389259 · doi ↗ · pubmed ↗
- 6How I diagnose and treat acute infection-associated purpura fulminans Blood Bendapudi PK Losman JA 1358136814520253978641610.1182/blood.2024025078 · doi ↗ · pubmed ↗
- 7Proposed classification and pathologic mechanisms of purpura fulminans and skin necrosis Semin Thromb Hemost Adcock DM Brozna J Marlar RA 333340161990228132210.1055/s-2007-1002686 · doi ↗ · pubmed ↗
- 8The cytoprotective protein C pathway Blood Mosnier LO Zlokovic BV Griffin JH 3161317210920071711045310.1182/blood-2006-09-003004 · doi ↗ · pubmed ↗