Real-world Effectiveness and Safety of Bictegravir/Emtricitabine/Tenofovir Alafenamide in Comparison With Other Regimens in People With HIV Starting Therapy With AIDS-Defining Conditions: Results From the CoRIS Cohort—The ACTUAS II Study
Ignacio Pérez-Valero, Diana Corona Mata, Angela Camacho Espejo, Marina Gallo, Alejandro G García-Ruiz de Morales, Chiara Fanciulli, Luz Martín-Carbonero, Sonia Calzado Isbert, Cristina Hernández Gutiérrez, Víctor Asensi, Antonio Rivero Juarez, Antonio Rivero, Santiago Moreno

TL;DR
This study finds that BIC/FTC/TAF is more effective and better tolerated than other HIV treatments in people with AIDS at 24 weeks.
Contribution
The study evaluates BIC/FTC/TAF effectiveness and safety in AIDS patients starting HIV therapy, a previously understudied population.
Findings
BIC/FTC/TAF showed higher viral suppression rates at 24 weeks compared to other regimens.
Treatment discontinuation rates were significantly lower with BIC/FTC/TAF at both 24 and 48 weeks.
By 48 weeks, differences in viral suppression and immunological recovery between regimens disappeared.
Abstract
The comparative effectiveness and tolerability of bictegravir/emtricitabine/tenofovir alafenamide (BIC/FTC/TAF) has not been sufficiently evaluated in people with AIDS who initiate therapy. The aim of the current study was to compare the effectiveness and tolerability of BIC/FTC/TAF with other first-line antiretroviral therapy (ART) regimens in treatment-naive adults from the CoRIS cohort who initiated ART with AIDS. Logistic regression models were used to estimate odds ratios (ORs) of association between initial regimen and achievement of viral suppression (VS), defined as human immunodeficiency virus RNA <50 copies/mL, and immunological recovery (IR), defined as CD4 count >200 cells/μL. Time to VS and the proportion of treatment discontinuations were also evaluated and compared, with all analyses conducted at weeks 24 and 48 after initiation of ART. We analyzed 90 individuals…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
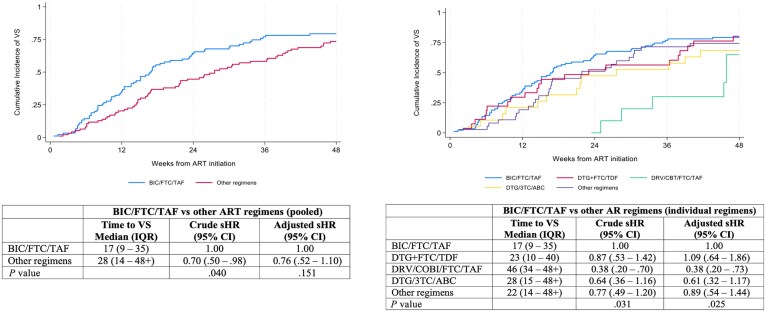 Figure 1
Figure 1| Characteristic | BIC/FTC/TAF (n = 90) | Other Regimens (n = 94) |
|
|---|---|---|---|
| Sex | .931 | ||
| Male | 77 (85.6) | 80 (85.1) | |
| Female | 13 (14.4) | 14 (14.9) | |
| Age, y | |||
| Median (IQR) | 42 (35–54) | 43 (35–53) | .633 |
| <30 | 10 (11.1) | 13 (13.8) | .778 |
| 30–49 | 53 (58.9) | 51 (54.3) | |
| ≥50 | 27 (30.0) | 30 (31.9) | |
| Transmission category | .083 | ||
| Men who have sex with men | 53 (58.9) | 43 (45.7) | |
| Heterosexual | 30 (33.3) | 35 (37.2) | |
| Intravenous drug use | 2 (2.2) | 1 (1.1) | |
| Other/unknown | 5 (5.6) | 15 (16.0) | |
| Country of origin | .203 | ||
| Spain | 55 (61.1) | 48 (51.1) | |
| Outside of Spain | 34 (37.8) | 46 (48.9) | |
| Unknown | 1 (1.1) | 0 | |
| CD4 count, cells/μL | |||
| Median (IQR) | 58 (26–153) | 78 (29–207) | .230 |
| <50 | 33 (36.7) | 28 (29.8) | .553 |
| ≥50 | 41 (45.6) | 45 (47.9) | |
| Unknown | 16 (17.8) | 21 (22.3) | |
| Viral load, copies/mL | |||
| Median (IQR) | 364 857 (116 000–1 065 259) | 347 406 (113 000–775 000) | .572 |
| <100 000 | 17 (18.9) | 17 (18.1) | .785 |
| ≥100 000 | 61 (67.8) | 61 (64.9) | |
| Unknown | 12 (13.3) | 16 (17.0) |
| ART Regimen | 24 Weeks | 48 Weeks | ||||
|---|---|---|---|---|---|---|
| no./No. With Data (%) | Crude OR (95% CI) | Adjusted OR (95% CI) | no./No. With Data (%) | Crude OR (95% CI) | Adjusted OR (95% CI) | |
| Viral suppression | ||||||
| BIC/FTC/TAF | 65/86 (75.6) | 1.00 | 1.00 | 68/78 (87.2) | 1.00 | 1.00 |
| Other regimens | 48/85 (56.5) | 0.42 (.20–.89) | 0.36 (.16–.78) | 62/76 (81.6) | 0.65 (.30–1.42) | 0.66 (.25–1.74) |
| | .023 | .010 | .283 | .402 | ||
| Immunological recovery | ||||||
| BIC/FTC/TAF | 41/86 (47.7) | 1.00 | 1.00 | 54/77 (70.1) | 1.00 | 1.00 |
| Other regimens | 52/84 (61.9) | 1.78 (.92–3.46) | 2.03 (1.01–4.05) | 62/75 (82.7) | 2.03 (.84–4.89) | 2.25 (.79–6.42) |
| | .087 | .046 | .114 | .130 | ||
| ART Regimen | 24 Weeks | 48 Weeks | ||||
|---|---|---|---|---|---|---|
| no./No. With Data (%) | Crude OR (95% CI) | Adjusted OR (95% CI) | no./No. With Data (%) | Crude OR (95% CI) | Adjusted OR (95% CI) | |
| Viral suppression | ||||||
| BIC/FTC/TAF | 65/86 (75.6) | 1.00 | 1.00 | 68/78 (87.2) | 1.00 | 1.00 |
| DTG + FTC/TDF | 14/26 (53.8) | 0.38 (.11–1.34) | 0.29 (.08–1.02) | 20/24 (83.3) | 0.74 (.32–1.68) | 0.77 (.29–2.03) |
| DRV/COBI/FTC/TAF | 3/11 (27.3) | 0.12 (.04–.41) | 0.16 (.04–.63) | 8/10 (80.0) | 0.59 (.13–2.57) | 0.48 (.09–2.51) |
| DTG/3TC/ABC | 9/17 (52.9) | 0.36 (.12–1.11) | 0.29 (.10–.83) | 10/17 (58.8) | 0.21 (.07–.65) | 0.23 (.05–.99) |
| Other regimens | 22/31 (71.0) | 0.79 (.35–1.79) | 0.75 (.25–2.24) | 24/25 (96.0) | 3.53 (.54–22.96) | 4.34 (.60–31.26) |
| | .004 | .008 | .011 | .049 | ||
| Immunological recovery | ||||||
| BIC/FTC/TAF | 41/86 (47.7) | 1.00 | 1.00 | 54/77 (70.1) | 1.00 | 1.00 |
| DTG + FTC/TDF | 14/26 (53.8) | 1.28 (.50–3.29) | 1.40 (.50–3.92) | 18/24 (75.0) | 1.28 (.45–3.63) | 1.24 (.36–4.27) |
| DRV/COBI/FTC/TAF | 7/11 (63.6) | 1.92 (.41–8.98) | 2.76 (.62–12.30) | 8/9 (88.9) | 3.41 (.60–19.41) | 4.61 (1.30–16.43) |
| DTG/3TC/ABC | 12/17 (70.6) | 2.63 (.73–9.56) | 3.31 (.89–12.33) | 15/17 (88.2) | 3.19 (.61–16.68) | 3.27 (.50–21.44) |
| Other regimens | 19/30 (63.3) | 1.90 (.78–4.62) | 1.82 (.56–5.94) | 21/25 (84.0) | 2.24 (.63–7.88) | 2.89 (.61–13.72) |
| | .322 | .218 | .414 | .190 | ||
| Reason for Discontinuation | BIC/FTC/TAF (n = 90) | No BIC/FTC/TAF |
| ||||
|---|---|---|---|---|---|---|---|
| DTG + FTC/TDF (n = 27) | DRV/COBI/FTC/TAF (n = 11) | DTG/3TC/ABC (n = 19) | Other Regimens | Total (n = 94) | |||
| During the first 24 weeks | |||||||
| Treatment changes | 4 (4.4) | 8 (29.6) | 2 (18.2) | 1 (5.3) | 8 (21.6) | 19 (20.2) | .001 |
| Reason for treatment change | |||||||
| Treatment failure | 0 | 0 | 0 | 0 | 1 (2.7) | 1 (1.1) | .318 |
| Adverse event | 2 (2.2) | 4 (14.8) | 2 (18.2) | 0 | 2 (5.4) | 8 (8.5) | .059 |
| Simplified treatment available | 0 | 1 (3.7) | 0 | 0 | 0 | 1 (1.1) | .318 |
| Drug interaction | 1 (1.1) | 0 | 0 | 1 (5.3) | 0 | 1 (1.1) | 1.000 |
| Patient's wish/decision | 0 | 0 | 0 | 0 | 0 | 0 | |
| Cost reduction | 0 | 0 | 0 | 0 | 0 | 0 | |
| Toxicity prevention | 1 (1.1) | 2 (7.4) | 0 | 0 | 4 (10.8) | 6 (6.4) | .060 |
| Other | 0 | 1 (3.7) | 0 | 0 | 1 (2.7) | 2 (2.1) | .167 |
| During the first 48 weeks | |||||||
| Treatment changes | 9 (10.0) | 16 (59.3) | 2 (18.2) | 4 (21.0) | 12 (32.4) | 34 (36.2) | <.001 |
| Reason for treatment change | |||||||
| Treatment failure | 2 (2.2) | 1 (3.7) | 0 | 1 (5.3) | 2 (5.4) | 4 (4.3) | .423 |
| Adverse event | 3 (3.3) | 4 (14.8) | 2 (18.2) | 0 | 2 (5.4) | 8 (8.5) | .136 |
| Simplified treatment available | 0 | 7 (25.9) | 0 | 2 (10.5) | 1 (2.7) | 10 (10.6) | .001 |
| Drug interaction | 2 (2.2) | 0 | 0 | 1 (5.3) | 0 | 1 (1.1) | .557 |
| Patient's wish/decision | 0 | 0 | 0 | 0 | 0 | 0 | |
| Cost reduction | 0 | 0 | 0 | 0 | 0 | 0 | |
| Toxicity prevention | 1 (1.1) | 3 (11.1) | 0 | 0 | 5 (13.5) | 8 (8.5) | .020 |
| Other | 1 (1.1) | 1 (3.7) | 0 | 0 | 2 (5.4) | 3 (3.2) | .329 |
| Adverse Event | BIC/FTC/TAF (n = 90) | No BIC/FTC/TAF |
| ||||
|---|---|---|---|---|---|---|---|
| DTG + FTC/TDF (n = 27) | DRV/COBI/FTC/TAF (n = 11) | DTG/3TC/ABC (n = 19) | Other Regimens (n = 37) | Total (n = 94) | |||
| Any adverse event | 3 (3.3) | 4 (14.8) | 2 (18.2) | 0 | 2 (5.4) | 8 (8.5) | .136 |
| Renal | 1 (1.1) | 1 (3.7) | 0 | 0 | 2 (5.4) | 3 (3.2) | .329 |
| Skin | 0 | 1 (3.7) | 2 (18.2) | 0 | 0 | 3 (3.2) | .087 |
| Gastrointestinal | 0 | 0 | 0 | 0 | 0 | 0 | |
| Neuropsychiatric | 1 (1.1) | 1 (3.7) | 0 | 0 | 0 | 1 (1.1) | 1.000 |
| Liver | 0 | 0 | 0 | 0 | 0 | 0 | |
| Other | 1 (1.1) | 1 (3.7) | 0 | 0 | 0 | 1 (1.1) | 1.000 |
| Substitution regimen | DOR + 3TC/ABC | DTG/3TC/ABC | DTG/3TC/ABC | … | DTG/3TC | DTG/3TC/ABC | |
| DTG/RPV | BIC/FTC/TAF | RAL + 3TC/ABC | … | EFV + 3TC/ABC | BIC/FTC/TAF | ||
| DTG + RPV + 3TC | DRV/COBI/FTC/TDF | … | … | … | DRV/COBI/FTC/TDF | ||
| … | DRV/RTV/FTC/TDF | … | … | … | DRV/RTV/FTC/TDF | ||
| … | … | … | … | … | DTG/3TC | ||
| … | … | … | … | … | RAL + 3TC/ABC | ||
| … | … | … | … | … | EFV + 3TC/ABC | ||
- —investigator-sponsored research
- —Gilead Sciences10.13039/100005564
- —Instituto de Salud Carlos III10.13039/501100004587
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHIV-related health complications and treatments · HIV/AIDS drug development and treatment · HIV/AIDS Research and Interventions
Antiretroviral therapy (ART) has transformed human immunodeficiency virus (HIV) infection into a chronic controllable disease with a life expectancy like that of the general population [1, 2]. However, late diagnosis remains a major problem for many people with HIV (PWH) who are diagnosed at later stages of the disease [3]. A particularly serious situation is the concomitant diagnosis of HIV and AIDS-defining conditions. In this case, it is crucial to choose an ART regimen with a good safety profile that achieves rapid viral suppression (VS) and immunological recovery (IR) [4].
Bictegravir combined with emtricitabine and tenofovir alafenamide (BIC/FTC/TAF) has shown high effectiveness and a good tolerability profile [5–7], comparable to dolutegravir (DTG)–based regimens up to 144 weeks of follow-up [8, 9]. As a result, BIC/FTC/TAF and DTG-based therapies are now preferred first-line therapies for PWH in most therapeutic guidelines [10, 11].
Clinical trials evaluating BIC/FTC/TAF as initial therapy [6, 7], like most studies on other regimens, including those in PWH with advanced disease [12], systematically excluded or did not report data on PWH with AIDS. Moreover, real-world data on this population remain scarce, and no study to date has focused on PWH with AIDS [13–17]. Consequently, it remains unknown whether the high effectiveness and tolerability on BIC/FTC/TAF in the general population extend to PWH diagnosed in the context of an opportunistic disease, especially given that most ART regimens show reduced efficacy/effectiveness in individuals with advanced HIV disease [18–20]. In PWH with AIDS, interactions between ART and treatments for these conditions may lead to either increased or decreased drug exposure, potentially enhancing the development of drug-related toxicities, which can affect tolerability or the therapeutic response to ART [21]. These considerations underscore the importance of evaluating the effectiveness and tolerability of BIC/FTC/TAF compared to other regimens in PWH with AIDS [22].
METHODS
Study Design
This study was designed to evaluate the effectiveness and tolerability of BIC/FTC/TAF compared to other first-line ART options in PWH enrolled in the Spanish Cohorte de la Red de Investigación en SIDA (CoRIS) cohort, who initiated ART with AIDS between 1 January 2019 and 30 November 2021.
CoRIS is an ongoing, open, multicenter, prospective cohort of adult PWH who were ART naive at study entry, first seen from 1 January 2004, at any of the 48 centers across 14 of Spain's 17 Autonomous Regions. It collects a standardized minimum dataset, including baseline and follow-up sociodemographic, immunological, and clinical data, as well as data on antiretroviral medications. The data undergo periodic quality control procedures to ensure accuracy. Participants are followed up regularly according to routine clinical practice, typically following Grupo de Estudio del SIDA recommendations [11, 23].
Study Population
We included PWH with AIDS, aged 18 years or older, who initiated first-line ART with BIC/FTC/TAF or other ART regimens between 1 January 2019 and 30 November 2021. For all analyses, we excluded (i) individuals who started ART (any regimen) as part of a clinical trial, since treatment selection and patient management in these settings are not fully at the physician's discretion and may not reflect real-life conditions; and (ii) those with no follow-up after ART initiation.
Outcomes
The outcome measures included the proportion of individuals achieving VS, defined as an HIV RNA load <50 copies/mL, at 24 and 48 weeks (±12 weeks) after ART initiation. Other outcomes were (i) the proportion of individuals achieving IR, defined as a CD4 count >200 cells/μL, at 24 and 48 weeks (±12 weeks) after ART initiation; (ii) time to VS during the first 48 weeks after ART initiation; and (iii) the proportion of individuals who discontinued treatment, along with reasons for discontinuation, during the first 24 and 48 weeks of ART. These outcomes were compared between BIC/FTC/TAF and other ART regimens (both as an aggregate group and as individual regimens). Additionally, BIC/FTC/TAF was compared with DTG-based regimens.
Reasons for discontinuation were classified as treatment failure, adverse event (AE), availability of simplified treatment, drug interaction, patient's wish/decision, cost reduction, toxicity prevention, other, and unknown. AEs were categorized as neuropsychiatric, renal, gastrointestinal, skin, liver, and other.
Statistical Analysis
All participants included in the CoRIS cohort who met the study's selection criteria were analyzed, meaning that outcomes were based on the initial regimen, with any subsequent changes disregarded; thus, once participants started a regimen, they were assumed to have remained on it. Differences in sociodemographic and clinical characteristics based on the initial regimen were assessed using the nonparametric Mann-Whitney test for continuous variables and the χ^2^ test for independence for categorical variables.
Logistic regression models were employed to estimate odds ratios (ORs) for the association between the initial regimen and the achievement of VS and IR at weeks 24 and 48 after ART initiation. For the analysis of time to VS during the first 48 weeks following ART initiation, an individual's follow-up period began at ART initiation and ended at the date of VS, death, last study contact, or after 48 weeks, whichever occurred first. Additionally, for the analyses of VS and IR at 24 and 48 weeks after ART initiation, only cases with available data within the assessment window were included; when multiple measurements were available within that window, the last one recorded was used. We employed the multiple decrement method to calculate the cumulative incidence of VS and used proportional hazards models on the subdistribution hazard to estimate subdistribution hazard ratios (sHRs) for VS, treating deaths before achieving VS as competing events.
Multivariable models were adjusted for the following potential confounders: sex, age at ART initiation, transmission category, educational level, country of origin (Spain, foreign-born), CD4 cell count, and viral load measured within the 6 months prior to ART initiation.
To adjust for the clustering of individuals within centers, robust methods were employed to estimate standard errors, which allowed for the calculation of 95% confidence intervals (CIs) and P values. Wald tests were used to derive P values.
RESULTS
Between January 2019 and November 2021, 184 individuals aged 18 years or older began ART with AIDS. Among them, 90 initiated therapy with BIC/FTC/TAF, while 94 started with other regimens (Supplementary Table 1). Baseline characteristics were similar between participants who initiated ART with BIC/FTC/TAF and those who started with other regimens (Table 1). Regarding the distribution of AIDS, it was homogeneous across both groups (Supplementary Table 2), with 1 notable exception: Nearly all individuals with tuberculosis who initiated ART were treated with other regimens due to the contraindication of using BIC/FTC/TAF in patients receiving or about to receive rifampicin.
Mortality
During follow-up, a total of 12 deaths were reported with 4 occurring in the BIC/FTC/TAF group and 8 in the other regimens group (P = .264). Among the deaths in the BIC/FTC/TAF group, 1 was AIDS related, 1 resulted from a non-AIDS infection, and 2 had an unknown cause. In the other regimens group, 7 deaths were AIDS related, while 1 was due to other causes (Supplementary Table 3).
Viral Suppression and Immunological Recovery
Viral suppression and immune recovery analyses are presented in Table 2. After 24 weeks from ART initiation, the proportion of individuals who achieved VS was higher with BIC/FTC/TAF compared to other regimens (75.6% vs 56.5%; P = .023). However, this difference lost statistical significance at week 48 after ART initiation (87.2% vs 81.6%; P = .283). At week 24, the adjusted odds ratio (aOR) for achieving VS with other regimens was 0.36 (95% CI, .16–.78; P = .01) times lower than with BIC/FTC/TAF.
In contrast, the proportion of individuals who achieved IR at week 24 after ART initiation was numerically lower with BIC/FTC/TAF than with other regimens (47.7% vs 61.9%; P = .087). The aOR of achieving IR with other regimens was 2.03 (95% CI, 1.01–4.05; P = .046) times higher than with BIC/FTC/TAF. At week 48 after ART initiation, the proportion of individuals who achieved IR with other regimens was similar than with BIC/FTC/TAF (70.1% vs 82.7%; P = .114).
At week 24, the aOR of achieving VS with darunavir/cobicistat/FTC/TAF (DRV/COBI/FTC/TAF) and DTG/lamivudine/abacavir (DTG/3TC/ABC) was 0.16 (95% CI, .04–.63) and 0.29 (95% CI, .10–.83), respectively, both significantly lower (P = .008) than with BIC/FTC/TAF (Table 3). Additionally, the aOR for achieving VS with a DTG-based regimen was 0.4 (95% CI, .17–.95; P = .037) times lower than with BIC/FTC/TAF. At week 48, the aOR of achieving VS with DTG/3TC/ABC was 0.23 (95% CI, .05–.99; P = .049) times lower than with BIC/FTC/TAF. No other significant differences were observed at this timepoint between BIC/FTC/TAF and the other individual regimens, nor between BIC/FTC/TAF and the DTG-based regimens (aOR 0.5 [95% CI, .17–1.47]; P = .207). Finally, the risk of achieving IR with the most prevalent ART options among the other regimens was similar to that associated with BIC/FTC/TAF at both week 24 and week 48. The aOR for achieving IR with DTG-based regimens was significantly higher than with BIC/FTC/TAF at week 24 (1.97 [95% CI, 1.03–3.77]; P = .042), but this statistical significance was lost at week 48 (1.85 [95% CI, .64–5.34]; P = .255).
Time to Viral Suppression
The median time to VS after ART initiation was 17 weeks (interquartile range [IQR], 9–35 weeks) among individuals who started with BIC/FTC/TAF and 28 weeks (IQR, 14 to >48 weeks) among those who initiated other regimens (Figure 1). Starting ART with other regimens, compared to BIC/FTC/TAF, was associated a lower likelihood of achieving VS (sHR, 0.7 [95% CI, .5–.98]; P = .04). However, this difference disappeared after adjusting for potential confounders (adjusted sHR, 0.76 [95% CI, .52–1.1]; P = .151).
Time to viral suppression during the first 48 weeks after antiretroviral therapy (ART) initiation according to initial ART regimen. Abbreviations: 3TC, lamivudine; ABC, abacavir; ART, antiretroviral therapy; BIC, bictegravir; CI, confidence interval; COBI, cobicistat; DRV, darunavir; DTG, dolutegravir; FTC, emtricitabine; IQR, interquartile range; sHR, subdistribution hazard ratio; TAF, tenofovir alafenamide; TDF, tenofovir disoproxil fumarate; VS, viral suppression.
Time to VS was also compared between BIC/FTC/TAF and the most prevalent ART options among other regimens. Significant differences were found in the time to VS with DRV/COBI/FTC/TAF compared to BIC/FTC/TAF (adjusted sHR, 0.38 [95% CI, .2–.73]; P = .025). However, no differences were observed in the time to VS between DTG-based regimens and BIC/FTC/TAF (adjusted sHR, 0.92 [95% CI, .61–1.4]; P = .703).
Treatment Discontinuations
The proportion of treatment discontinuations during the first 24 weeks after ART initiation was significantly lower among individuals starting with BIC/FTC/TAF compared to those initiating other regimens (4.4% vs 20.2%; P < .001). This difference is primarily attributed to the lower proportion of discontinuations due to AEs (2.2% vs 8.5%; P = .06) and toxicity prevention (main reason: tenofovir disoproxil fumarate withdrawal) (1.1% vs 6.4%; P = .06). Discontinuations during the first 48 weeks after ART initiation were similar to those observed in the first 24 weeks (Table 4).
At week 48, 3 participants discontinued BIC/FTC/TAF due to AEs: 1 experienced impaired renal function and was switched to DTG + rilpivirine (RPV) + 3TC; another developed a moderate headache and switched to doravirine + 3TC/ABC; and the third experienced sensory neuropathy and was switched to DTG/RPV (Table 5).
Sensitivity Analyses
Given that nearly all participants with tuberculosis were treated with other regimens, we performed sensitivity analyses excluding these individuals. These analyses showed minimal changes compared to the overall findings: At week 48, the aOR for VS with other regimens lost significance (aOR, 0.68 [95% CI, .23–1.97]; P = .475), while the aOR for IR reached significance (aOR, 2.89 [95% CI, 1.09–7.64]; P = .032).
DISCUSSION
In CoRIS, a real-world European cohort, first-line therapy with BIC/FTC/TAF in PWH with AIDS was associated with high proportions of VS and IR at both 24 and 48 weeks, along with low rates of ART discontinuations. Compared to other regimens, BIC/FTC/TAF was associated with higher odds of achieving VS at week 24 (but not at week 48), a shorter time to VS, and a lower rate of ART discontinuations, likely due to a better tolerability profile. Conversely, participants starting ART with BIC/FTC/TAF had lower odds of achieving IR. These results suggest that BIC/FTC/TAF has a favorable tolerability and durability profile in PWH with AIDS, consistent with prior observations in PWH without AIDS.
Since this is the first study to evaluate BIC/FTC/TAF in PWH with AIDS, direct comparisons with previous studies are limited. However, when comparing our results to those of previous studies evaluating BIC/FTC/TAF in individuals with advanced HIV disease, similar rates of VS are observed. Specifically, the rate of VS in participants enrolled in the GS-US-380-1489/1490 clinical trials with advanced HIV disease was 99%, slightly higher than the 87.2% observed in our study [6, 7]. This difference may be due to the exclusion of candidates with AIDS in these 2 trials and the controlled follow-up within a clinical trial setting.
Under real-life conditions, the performance of BIC/FTC/TAF in advanced HIV disease has been evaluated in 3 cohort studies: CoRIS [13], Observational Pharmaco-Epidemiology Research and Analysis (OPERA) [14, 15], and a Taiwanese cohort [16]. All of these studies reported a low rate of ART discontinuations with BIC/FTC/TAF compared to other ART regimens [13–16]. The results in PWH, mostly with advanced disease but without AIDS, were similar to those reported in our study of PWH with AIDS. Our findings support the notion that BIC/FTC/TAF offers greater durability than other regimens, both in individuals with advanced HIV disease, whether or not they have AIDS.
The lower rate of ART discontinuations observed with BIC/FTC/TAF in our study can be attributed to fewer discontinuations due to AEs and to prevent ART-related toxicities. These factors were also associated with a reduced rate of ART discontinuations in the Taiwanese cohort [16], although this association was not observed in the OPERA cohort [14]. This lack of association should be interpreted with caution, as the reasons for discontinuation were unknown for 56% of the participants. Given this, we suggest that the low rate of BIC/FTC/TAF discontinuations due to AEs reported in first-line clinical trials may also apply to PWH with AIDS [6, 7].
In our study, consistent with the OPERA and Taiwanese cohorts [14–16], the likelihood of achieving VS with BIC/FTC/TAF and DTG/3TC/ABC was similar at 48 weeks. Although participants who started with BIC/FTC/TAF achieved VS more quickly than those on DTG/3TC/ABC, the difference was not statistically significant at 48 weeks. This suggests that while BIC/FTC/TAF may provide an advantage in achieving earlier viral suppression, long-term outcomes between these regimens seem comparable. Several factors may explain this, including potential differences in antiviral activity between BIC/FTC/TAF and DTG/3TC/ABC, possibly influenced by the use of TAF or ABC [6]. However, this remains speculative, and adherence differences may also play a role.
Additionally, participants who started therapy with DRV/COBI/FTC/TAF had a lower likelihood of achieving VS at 48 weeks compared to those starting with BIC/FTC/TAF. Further research is needed to confirm whether DRV/COBI/FTC/TAF poses a disadvantage, with results from the Late Presenter Treatment Optimisation Study trial expected to shed light on this [24].
A limitation of BIC/FTC/TAF as first-line therapy in PWH with AIDS is the lower odds of achieving rapid IR compared to other regimens. This finding has not been assessed in previous studies involving advanced HIV disease. In the OPERA cohort, IR rates were reported, but only at 48 weeks after ART initiation. At that timepoint, the rates were comparable between BIC/FTC/TAF (67%) and other regimens (60%–68%) [14]. The slower IR observed in our study up to week 24 may be attributed to selection bias, where BIC/FTC/TAF was chosen for individuals with more advanced disease and poorer immunological status. This hypothesis is supported by the lower CD4 cell counts observed in our study among participants on BIC/FTC/TAF, as well as the fact that the differences in IR were more pronounced when participants with tuberculosis were excluded. This aligns with existing evidence indicating that immune reconstitution in PWH with severe diseases like tuberculosis is generally slower and less effective [25]. Regardless of the validity of this hypothesis, the magnitude of the difference in odds was very small, short-lived, and not associated with worse clinical outcomes (Supplementary Table 3). Therefore, we believe its impact on the selection of BIC/FTC/TAF as a first-line regimen would be minimal.
This study has several strengths. CoRIS is a large prospective cohort that accurately represents the HIV population diagnosed since 2014 in Spain, making the results highly representative of PWH diagnosed with AIDS today. This enables us to obtain an accurate picture of real-world prescription practices and related health outcomes for PWH with opportunistic diseases in our clinical setting.
However, this study also has some limitations. Although the assessment windows for the 24- and 48-week results were broad (±12 weeks), a small percentage of participants lacked data on HIV RNA or CD4 counts during these periods, mainly due to reduced blood draws during the coronavirus disease 2019 pandemic. Another limitation is the relatively narrow eligibility and follow-up period, as BIC/FTC/TAF was approved in Spain in June 2018. Although the number of participants who initiated ART with BIC/FTC/TAF was sufficient to evaluate the study outcomes, future analyses involving a larger participant pool and extended follow-up would provide more robust insights.
Furthermore, we did not analyze immune reconstitution inflammatory syndrome (IRIS) cases, so the impact of IRIS on participants initiating ART with BIC/FTC/TAF or other regimens remains unknown. However, the impact is likely minimal, as no participants discontinued ART due to IRIS.
Finally, as with any observational study, there may be unmeasured biases. Nonetheless, we minimized their impact through rigorous data collection and statistical adjustments.
In conclusion, our study results suggest that BIC/FTC/TAF is a viable first-line therapy for PWH with AIDS. In this population, where rapid viral suppression is crucial, BIC/FTC/TAF demonstrated favorable effectiveness in reducing viral load. While no significant differences in time to VS were observed after adjusting for potential confounders, the regimen showed durability, supported by its favorable safety and tolerability profile.
Supplementary Material
ciaf162_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Samji H, Cescon A, Hogg RS, et al Closing the gap: increases in life expectancy among treated HIV-positive individuals in the United States and Canada. P Lo S One 2013; 8:e 81355.24367482 10.1371/journal.pone.0081355 PMC 3867319 · doi ↗ · pubmed ↗
- 2Lohse N, Obel N. Update of survival for persons with HIV infection in Denmark. Ann Intern Med 2016; 165:749–50.27842400 10.7326/L 16-0091 · doi ↗ · pubmed ↗
- 3Croxford S, Stengaard AR, Brännström J, et al Late diagnosis of HIV: an updated consensus definition. HIV Med 2022; 23:1202–8.36347523 10.1111/hiv.13425 PMC 10100195 · doi ↗ · pubmed ↗
- 4Mocroft A, Neesgard B, Zangerle R, et al Prevalence of and prognosis for poor immunological recovery by virally suppressed and aged HIV-infected patients. Front Med (Lausanne) 2023; 10:1259871.37928477 10.3389/fmed.2023.1259871 PMC 10625403 · doi ↗ · pubmed ↗
- 5Tsiang M, Jones GS, Goldsmith J, et al Antiviral activity of bictegravir (GS-9883), a novel potent HIV-1 integrase strand transfer inhibitor with an improved resistance profile. Antimicrob Agents Chemother 2016; 60:7086–97.27645238 10.1128/AAC.01474-16PMC 5118987 · doi ↗ · pubmed ↗
- 6Gallant J, Lazzarin A, Mills A, et al Bictegravir, emtricitabine, and tenofovir alafenamide versus dolutegravir, abacavir, and lamivudine for initial treatment of HIV-1 infection (GS-US-380-1489): a double-blind, multicentre, phase 3, randomised controlled non-inferiority trial. Lancet 2017; 390:2063–72.10.1016/S 0140-6736(17)32299-728867497 · doi ↗ · pubmed ↗
- 7Sax PE, Pozniak A, Montes ML, et al Coformulated bictegravir, emtricitabine, and tenofovir alafenamide versus dolutegravir with emtricitabine and tenofovir alafenamide, for initial treatment of HIV-1 infection (GS-US-380-1490): a randomised, double-blind, multicentre, phase 3, non-inferiority trial. Lancet 2017; 390:2073–82.10.1016/S 0140-6736(17)32340-128867499 · doi ↗ · pubmed ↗
- 8Wohl DA, Yazdanpanah Y, Baumgarten A, et al Bictegravir combined with emtricitabine and tenofovir alafenamide versus dolutegravir, abacavir, and lamivudine for initial treatment of HIV-1 infection: week 96 results from a randomised, double-blind, multicentre, phase 3, non-inferiority trial. Lancet HIV 2019; 6:e 355–63.10.1016/S 2352-3018(19)30077-331068270 · doi ↗ · pubmed ↗