Understanding Surgeon Professionalism in Indonesia: A Qualitative Study in a Multicultural and Resource-Limited Context
DANIEL ARDIAN SOESELO, RETNO ASTI WERDHANI, TOAR JEAN MAURICE LALISANG, AGUS PURWADIANTO, WIRSMA ARIF HARAHAP, RENNIE YOLANDA, THEDDEUS OCTAVIANUS HARI PRASETYONO, DIANTHA SOEMANTRI, ARDI FINDYARTINI

TL;DR
This study explores how surgeon professionalism is perceived in Indonesia, highlighting cultural and systemic influences on non-technical aspects of professionalism.
Contribution
The first national-level qualitative study on surgeon professionalism in Indonesia, emphasizing cultural and systemic influences.
Findings
Four non-technical themes of surgeon professionalism were identified: fulfilling roles, integrity, communication, and collaboration.
Cultural values and systemic challenges, such as resource disparities, influence perceptions of professionalism.
The findings suggest the need for culturally sensitive interventions to improve surgical care quality and patient safety.
Abstract
Surgeons’ professionalism is vital for ensuring safe surgical care, particularly in Indonesia, where cultural and systemic factors present unique challenges to healthcare delivery. Professionalism affects surgical outcomes, patient safety, and interprofessional collaboration directly. This study represents the first national-level exploration of surgical professionalism, involving culturally diverse participants from various regions. To explore how healthcare professionals and patients perceive surgeon professionalism in Indonesia, emphasizing cultural and systemic influences. This qualitative study employed a phenomenological approach to capture the lived experiences and perspectives of informants regarding surgeons’ professionalism. This study was conducted at public, private, and military healthcare institutions in Indonesia, including type B, C, and D hospitals, as well as…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
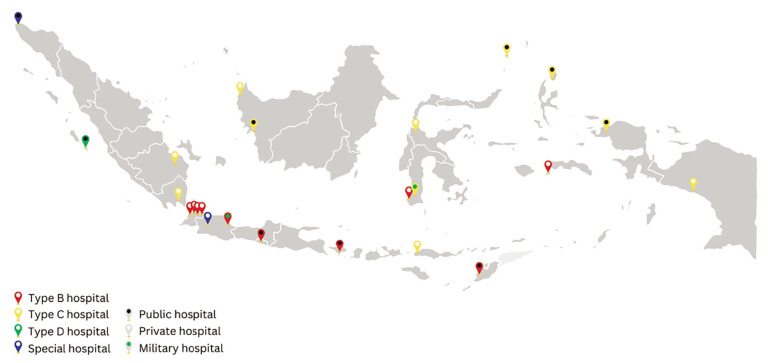 Figure 1
Figure 1| Characteristic | Number of Respondents (%) | Mean (SD) |
|---|---|---|
| Profession (N=27) | ||
| Surgeon | 4 (14.8) | |
| Anesthesiologist | 3 (11.1) | |
| Pediatrician | 3 (11.1) | |
| Internist | 3 (11.1) | |
| Operating room (OR) nurse | 4 (14.8) | |
| Ward nurse | 2 (7.4) | |
| Hospital management | 5 (18.5) | |
| Patient representative | 3 (11.1) | |
| Age (years) (N=27) | 46.0 ± 8.97 | |
| Years of Experience (years) (N=24) | 11.7 ± 6.70 | |
| Geographical Distribution (N=24) | ||
| Sumatra | 4 (16.6) | |
| Java | 7 (29.1) | |
| Kalimantan | 2 (8.3) | |
| Sulawesi | 4 (16.6) | |
| Bali, Nusa Tenggara | 3 (12.5) | |
| Papua, Maluku | 4 (16.6) | |
| Hospital Classification (N=24) | ||
| Type B | 10 (41.6) | |
| Type C | 11 (45.8) | |
| Type D | 1 (4.1) | |
| Special hospital | 2 (8.3) | |
| Hospital Ownership (N=24) | ||
| Public | 9 (37.5) | |
| Private | 13 (54.1) | |
| Military | 2 (8.3) | |
| No. | Professionalism Theme | Professionalism Sub-Themes | Professionalism Behavior Definition | Exemplar of quotes |
|---|---|---|---|---|
| 1 | Fulfilling the role and responsibilities as a surgeon | Working according to Standard Operating Procedures (SOP) | Performing work according to Standard Operating Procedures (SOP) |
|
| Managing risks/complications of surgical procedures | Being responsible in attitude, financially, and morally for risks/complications associated with surgery |
| ||
| Considering benefits and risks | Considering benefits and risks before deciding on surgery |
| ||
| 2 | Upholding integrity and personal responsibility | Being honest about surgery fees and emergency criteria | Being honest in determining surgery fees and emergency criteria |
|
| Controlling emotions | Controlling emotions in unpleasant situations |
| ||
| Displaying professional identity | Wearing a doctor’s coat/scrubs appropriately |
| ||
| Adhering to schedules | Following surgery, clinic, and visiting times |
| ||
| 3 | Good communication skills | Communicating effectively with clarity to the patients | Building communication clearly, openly, and transparently with patients |
|
|
| ||||
| 4 | Collaborating effectively in multidisciplinary team | Being open-minded and collaborate with multidisciplinary team | Building good relationships with colleagues, nurses, and medical staff |
|
| Fostering respectful relationships with colleagues | Respecting professional equality |
| ||
| Teaching willingness | Participating in educating other healthcare professionals |
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Health Workforce Issues · Global Health and Surgery · Cultural Competency in Health Care
Introduction
Safe surgical care is essential for equitable healthcare access. The Lancet Committee on Global Surgery (LCGS) highlighted the need for skilled surgeons and adequate infrastructure. Professionalism, which encompasses both technical and non-technical skills, plays a key role in ensuring safe surgery. These skills are crucial for maintaining patient safety, improving surgical outcomes, and enhancing the overall quality of care ( 1
- 3 ).
Unprofessional behaviours among surgeons have been linked to surgical complications ( 4 , 5 ), patient complaints ( 6 ), malpractice claims ( 7 ), and procedural errors ( 8 ). Therefore, improving both technical competence and non-technical aspects, such as communication, leadership, and teamwork, is needed ( 9 ).
Professionalism is shaped by cultural norms, societal expectations, and healthcare infrastructure. In non-Western cultures, professionalism is often influenced by religion, family, and social norms ( 10
- 12 ). Indonesia, as an archipelagic country with over 17,000 islands and a population exceeding 261 million, faces unique challenges in healthcare delivery, including geographical disparities and uneven population distribution, with 57% residing on the small island of Java. Understanding surgical professionalism in Indonesia is crucial not only for improving healthcare practices within the country but also for contributing to a broader, contextual understanding of professionalism on a global scale ( 13 , 14 ).
While this study focuses on Indonesia, the challenges surrounding surgical professionalism in culturally diverse and resource-constrained settings are shared across many Southeast Asian countries. However, little research has explored how institutional and cultural factors intersect to shape the surgeons’ professional behaviour in this region. In Indonesia, hospitals are classified from type D (district-level) to type A (national referral centers), based on their service capacity, diagnostic facilities, number of beds, availability of specialist doctors, and level of specialization. These classifications reflect significant disparities in infrastructure and human resources, which directly impact how surgical professionalism is expressed and perceived. By including participants from type B, C, and D hospitals, this study captures a more comprehensive and contextual understanding of surgical professionalism. This study represents the first national-level exploration of surgical professionalism in Indonesia, involving culturally diverse participants from across all regions. These comparative insights highlight institutional-level influences and offer a valuable foundation for future regional studies across Southeast Asia.
Methods
Context
Indonesia, as the world’s largest archipelago, faces unique challenges in delivering equitable healthcare due to its diverse ethnic, cultural, and socioeconomic factors, along with a segmented National Health Insurance System (BPJS). Healthcare services are divided into primary, secondary, and tertiary care services, with primary care being delivered through public health centers (Puskesmas) and Primary Care Clinics. Secondary and tertiary care is provided by hospitals and is classified into types C and D at the district level, type B at the provincial level, and type A at the national level. Surgical services in Indonesia can be provided in hospitals from type A to type D ( 15 , 16 ). However, these services are predominantly delivered in type C and D hospitals, which constitute the majority of hospitals in Indonesia and typically have more limited resources and infrastructure ( 17 ). This disparity in resources and geographical distribution has a significant impact on the overall delivery of surgical services in Indonesia ( 15 , 18 ).
Design and study participants
This qualitative study used a descriptive phenomenological approach to explore professionalism among Indonesian surgeons through in-depth interviews. This approach allowed researchers to capture a contextualized understanding of professionalism based on the experience of the informants ( 19 ). Participants included eight respondent categories, including surgeons, anesthesiologists, pediatricians, internists, operating room (OR) nurses, ward nurses, hospital management, and patient representatives from diverse healthcare settings.
The inclusion criteria were as follows: 1) actively practicing specialists (surgeons, anesthesiologists, pediatricians, internists) and nurses (OR nurses and ward nurses) with a minimum of one year of work experience; 2) hospital managers currently serving in medical leadership roles with at least one year of experience; and 3) patients who had undergone surgical procedures and interacted with doctors within the past six months. The exclusion criteria were healthcare professionals who were currently not practicing or on leave, and respondents who were unable or unwilling to participate in the interview process due to communication barriers or time constraints.
Due to the lack of a centralized database, participant recruitment began by sending formal requests to professional organizations to recommend five names per Indonesian region; however, only the nursing association responded. For the other categories, snowball sampling was conducted by contacting colleagues and requesting referrals who met the inclusion criteria, followed by direct outreach to those individuals.
Data collection
The interviews were conducted by an experienced surgeon (DAS) with extensive knowledge of the Indonesian healthcare system and expertise in qualitative data collection. Participants were informed about the researcher’s background and the purpose of the study, which focused on exploring their perceptions of professionalism in surgical care. To address potential bias, researchers’ reflexivity was integral throughout the data collection and analysis. The interviewer and the authors were aware of how their background in surgery and/or medical education might influence interactions or interpretations. To minimize this, they maintained a neutral stance during interviews and held regular team discussions to ensure that participants’ voices were represented authentically.
Data collection occurred between July and November 2024. The interviews (30-40 minutes) were conducted by online meeting, audio-recorded, and transcribed verbatim. The core interview question addressed was: “How are surgeons’ professional behaviours perceived in the context of healthcare services, interactions with other healthcare workers, and their roles as employees in a hospital setting?”.
The study involved eight categories of respondents; we planned to interview three to five participants in each category. A total of 27 participants were recruited, as maximum variation had been achieved (in terms of hospital types, gender diversity, and geographic distribution across Indonesia). No new themes emerged during the final interviews, indicating that data saturation had been reached. All participants gave informed consent before the interviews, and the confidentiality of their identities and affiliated hospitals was strictly maintained throughout the study.
Data analysis
Thematic analysis was conducted by a multidisciplinary research team with expertise in medical education and surgery (DAS, AF, DS, TOHP), using Colaizzi’s seven-step method for phenomenological analysis. The process followed each step systematically: 1) The primary researcher first read all interview transcripts thoroughly to gain an overall understanding of the data; 2) Each team member independently identified significant statements related to surgeons’ professionalism; 3) These statements were interpreted to generate preliminary codes capturing their essential meanings; 4) Similar codes were grouped into broader thematic categories; 5) Each thematic code was defined and refined based on participants’ lived experiences; 6) All thematic codes were discussed collaboratively among all researchers to ensure clarity and consistency; and 7) Member checking was conducted by sharing the findings with selected participants to validate accuracy and credibility. Reflexive discussions and manual documentation were maintained throughout the process to ensure trustworthiness. Taguette software was employed for detailed coding ( 20 ). Themes emerged inductively and were supported by triangulation from multiple sources, including diverse participant roles, supporting documents, and researcher reflexivity. The research team critically examined the data to minimize bias and achieve data saturation. The final analysis clearly presented the major themes while also acknowledging minor themes and variations to capture the complexity of perspectives within the data.
Ethics committee approval code
We obtained ethical approval from The Ethics Committee of the Faculty of Medicine, University of Indonesia, Cipto Mangunkusumo Hospital number KET-741/UN2.F1/ETIK/PPM.00.02/2024.
Results
A total of 27 participants were involved in the study (Table 1). The participants had an average age of 46 years and an average of 11.7 years of experience. They represented diverse regions across Indonesia and worked in type B, C, and D hospitals, as well as specialty hospitals. The participants were selected from public, private, and military healthcare institutions across the country. The data distribution represents all regions of Indonesia, as illustrated in Figure 1.
Geographical Distribution of the Study Participants across Indonesia
The in-depth interviews identified four key themes of professionalism among surgeons, with 11 subthemes. These themes reflect a comprehensive understanding of surgeon professionalism in the Indonesian context. These professionalism themes were further elaborated and exemplified in the specific behaviours detailed in Table 2.
Discussion
This study explored Indonesian surgeons’ professionalism as perceived by Indonesian healthcare professionals and patient representatives. Professionalism in Indonesia is shaped by cultural values and healthcare resource disparities ( 21 ). Our study identified four non-technical themes of surgeons’ professionalism, particularly significant to the Indonesian context: fostering respectful relationships with colleagues and teaching willingness. These two themes were discussed in greater detail due to their distinct relevance to local sociocultural dynamics, whereas the other themes, such as communication and accountability, are widely recognized across cultures and have been extensively explored in the global literature. While global standards such as The Lancet Committee on Global Surgery (LCGS), Accreditation Council of Graduate Medical Education (ACGME), General Medical Council (GMC), and American College of Surgeons (ACS) emphasize the importance of medical expertise, effective communication, and collaboration among healthcare professionals, Asian professionalism faces unique sociocultural challenges and issues related to the national health system ( 1 , 22
- 26 ).
Fostering respectful relationships with colleagues
In Indonesia, cultural norms emphasizing hierarchy and harmony significantly shape surgical professionalism ( 21 , 27 ). Unlike Western models that emphasize individual competencies, Indonesian surgeons prioritize collaborative relationships, demonstrated by respecting professional equality, maintaining the honour of colleagues, and respecting more experienced colleagues. Respecting professional equality is demonstrated by respecting working relationships with colleagues, nurses, and other medical staff. Maintaining the honour of colleagues is reflected in not blaming the diagnoses and surgical actions of other surgeons. Respect for more experienced colleagues is shown by respecting the experience and knowledge gained by senior doctors. These behaviours are deeply embedded in Indonesia’s cultural norms, where hierarchy plays a crucial role within the medical profession ( 13 ).
Indonesian medical practice is influenced by its hierarchical culture, where respect for seniority and authority plays a significant role ( 28 , 29 ). Junior surgeons often delay their surgeries to accommodate seniors, and feedback is carefully managed to avoid conflict ( 27 ). This culture fosters a collective approach to professionalism, ensuring respect and collaboration within the surgical team, and contributes to a distinct Indonesian model of medical professionalism ( 21 ).
In Indonesia, the hierarchical view of physicians as having a higher status than nurses can lead to disparities in professional equality, affecting teamwork and collaboration in clinical settings ( 30 , 31 ). Maintaining the honour of colleagues is crucial, as patients often assign blame when complications arise. Surgeons must respect their colleagues, ensuring that all team members are valued and supported, which enhances the quality of care provided to patients while also promoting a more equitable workplace culture ( 32 , 33 ).
Indonesian hierarchical culture contrasts with Western frameworks that encourage open feedback. While promoting respect and harmony, it can hinder discussions about errors and performance improvement, thereby impacting quality and patient safety. This highlights the need for awareness in developing medical professionalism in Indonesia ( 34 , 35 ), and culturally sensitive approaches in addressing the need for growth and improvement, such as good role-modeling from leaders or those with authority and provision of a safe environment ( 28 , 36 ).
Teaching Willingness
This is a uniquely Indonesian theme that highlights the surgeon’s role beyond the operating room. In Indonesia, surgeons are often expected to engage in teaching, mentoring, and contribute to community-based healthcare. This expectation arises from the country’s vast geographical size, resource limitations, and sociocultural diversity. Surgeons are also expected to take on roles as educators and leaders within their healthcare teams ( 37 , 38 ). Surgeons frequently teach nurses, junior doctors, and other healthcare workers, ensuring that the quality of care is maintained even in regions with limited access to specialized training ( 39 , 40 ).
Surgeons in Indonesia are also often involved in managerial tasks, including navigating the complexities of the National Health Insurance System (BPJS), which provides universal healthcare but offers lower reimbursement rates ( 41 , 42 ). This creates income disparities for surgeons in public hospitals, particularly types C and D, which constitute the majority of hospitals in Indonesia, directly affecting their welfare and their clinical performance ( 18 ). Many surgeons work in multiple hospitals to support their income, potentially affecting post-operative care and overall clinical performance ( 43 , 44 ).
Professionalism in Indonesia is shaped by its vast geographic dispersion, varying healthcare resources, and hospital classifications ( 15 , 45 ). Surgeons in smaller hospitals, particularly type C and D, often face resource limitations, requiring patient referrals to higher-tier hospitals ( 45 , 46 ). Surgeons in remote areas may encounter logistical challenges, including long journeys and assisting patients with financial support, especially under the National Health Insurance System (BPJS). These complexities highlight the dual clinical and administrative roles that surgeons must navigate ( 47 ).
Surgeons in Indonesia demonstrate resilience and adaptability in a complex healthcare system marked by hierarchical norms, resource disparities, and hospital classifications ( 13 ). By addressing the challenges, including referral processes and financial assistance, they improve patient care while exemplifying professionalism rooted in their sociocultural environment ( 41 ). Future efforts to enhance surgical care in Indonesia should consider these unique dynamics while ensuring that professional standards are culturally relevant and responsive to local challenges.
Strengths and Limitations of the Study
The strength of this study lies in its use of in-depth interviews with multidisciplinary and multilevel stakeholders, including surgeons, anesthesiologists, pediatricians, internists, OR nurses, ward nurses, hospital management, and patient representatives from diverse healthcare settings. This approach provided nuanced and comprehensive insights into professionalism in various contexts. However, a limitation is the overrepresentation of participants from district-level hospitals (Type C and D), with limited input from national- and provincial-level hospitals (Type A and B), potentially affecting the generalizability of the findings to higher-level healthcare settings. This imbalance may have influenced the types of the themes that emerged, particularly those related to resource limitations, hierarchical dynamics, and day-to-day interprofessional collaboration, which may be more prominent in lower-resourced settings. As a result, the findings may not fully capture the nuances of surgeons’ professionalism in more academic or specialized hospital environments, where organizational culture, expectations, and professional roles can differ significantly. Future research should include a more proportionate representation of participants from higher-level institutions to enhance the transferability and comprehensiveness of the findings.
Despite these limitations, this study serves as the first national-level exploration of surgical professionalism in Indonesia, providing baseline data that can inform future research, curriculum development, and policy planning. These findings are expected to guide future studies and contribute to shaping policies that are more responsive to the unique sociocultural and systemic challenges faced by Indonesian surgeons.
Conclusion
This study offers in-depth insights into surgeons’ professionalism in Indonesia, emphasizing how it is shaped by cultural norms, systemic limitations, and institutional hierarchies. The findings demonstrate that professionalism extends beyond individual competence, encompassing collective values such as respect for seniority, collaborative decision-making, and teaching willingness. These contextual nuances challenge global assumptions and underscore the need for culturally sensitive approaches to promoting professionalism in surgery.
Based on these findings, we propose actionable recommendations for various stakeholders. Policymakers should consider developing national guidelines on surgical professionalism that reflect local cultural dynamics. Hospital administrators, especially in type C and D institutions, should implement interprofessional training programs that foster respectful collaboration and professional equality. Educational institutions should integrate professionalism into curricula using context-specific cases and reflective learning methods. These interventions may contribute to strengthening professionalism in multicultural and resource-limited healthcare settings, ultimately improving patient outcomes and the overall quality of surgical care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Meara JG Leather AJM Hagander L Alkire BC Alonso N Ameh E Aetal Global Surgery 2030: Evidence and solutions for achieving health, welfare, and economic development The Lancet 2015386999356962410.1016/S 0140-6736(15)60160-X 25924834 · doi ↗ · pubmed ↗
- 2Marshall S Nataraja R Chapter 29: Patient safety and surgical education. In: Advancing Surgical Education: Theory, Evidence, and Practice 2019 Singapore Springer 32737
- 3Davis CH Di Lalla GA Perati SR Lee JS Oropallo AR Reyna C Retal A review of professionalism in surgery Proc Bayl Univ Med Cent 202437699373944008710.1080/08998280.2024.2403375 PMC 11492646 · doi ↗ · pubmed ↗
- 4Cooper WO Spain DA Guillamondegui O Kelz RR Domenico HJ Hopkins Jetal Association of coworker reports about unprofessional behavior by surgeons with surgical complications in their patients JAMA Surg 201915498283410.1001/jamasurg.2019.1738 PMC 658502031215973 · doi ↗ · pubmed ↗
- 5Nilsson L Risberg MB Montgomery A Sjödahl R Schildmeijer K Rutberg H Preventable adverse events in surgical care in Sweden: A nationwide review of patient notes Medicine (Baltimore). 20169511 e 304710.1097/MD.0000000000003047 PMC 483990726986126 · doi ↗ · pubmed ↗
- 6Catron TF Guillamondegui OD Karrass J Cooper WO Martin BJ Dmochowski R Retal Patient complaints and adverse surgical outcomes Am J Med Qual Off J Am Coll Med Qual 20163154152210.1177/106286061558415825916627 · doi ↗ · pubmed ↗
- 7Lagoo J Berry WR Miller K Neal BJ Sato L Lillemoe K Detal Multisource evaluation of surgeon behavior is associated with malpractice claims Ann Surg 2019270184902957891010.1097/SLA.0000000000002742 · doi ↗ · pubmed ↗
- 8Cochran A Elder WB Effects of disruptive surgeon behavior in the operating room Am J Surg 20152091657010.1016/j.amjsurg.2014.09.01725454961 · doi ↗ · pubmed ↗