Lessons Learned From A Geriatric Referral Model in People With HIV
Sarah R Gorvetzian, Kristine M Erlandson, Evelyn Iriarte, Skotti Church, Jacob Walker

TL;DR
A geriatric consultation model for older adults with HIV was implemented but faced challenges in adoption due to structural and financial barriers.
Contribution
This paper presents a novel geriatric referral model for people with HIV and identifies barriers to its implementation.
Findings
Geriatricians made recommendations on referrals, medication changes, and osteoporosis screening.
Most HIV providers expressed willingness to refer future patients to the program.
Limited uptake of the program was observed despite positive outcomes.
Abstract
People with HIV experience geriatric syndromes commonly found in much older populations and may benefit from geriatrician consultation. Multiple clinical models have emerged to address this need. We describe a model at the University of Colorado and the barriers to its robust implementation. The UCHealth Infectious Disease clinic implemented a referral-based model to connect high-risk people with HIV ≥50 years old with the UCHealth Seniors clinic. During geriatric consultation, patients were screened for functional status, preventative care, socioenvironmental factors, and cognitive/mental health concerns. Geriatricians communicated recommendations to the primary HIV provider. HIV providers completed a survey about the program. From January 2018 to July 2019, 11 patients underwent geriatric consultation. The average age was 69 years old (SD = 7.4; range 59–80). Geriatricians made…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
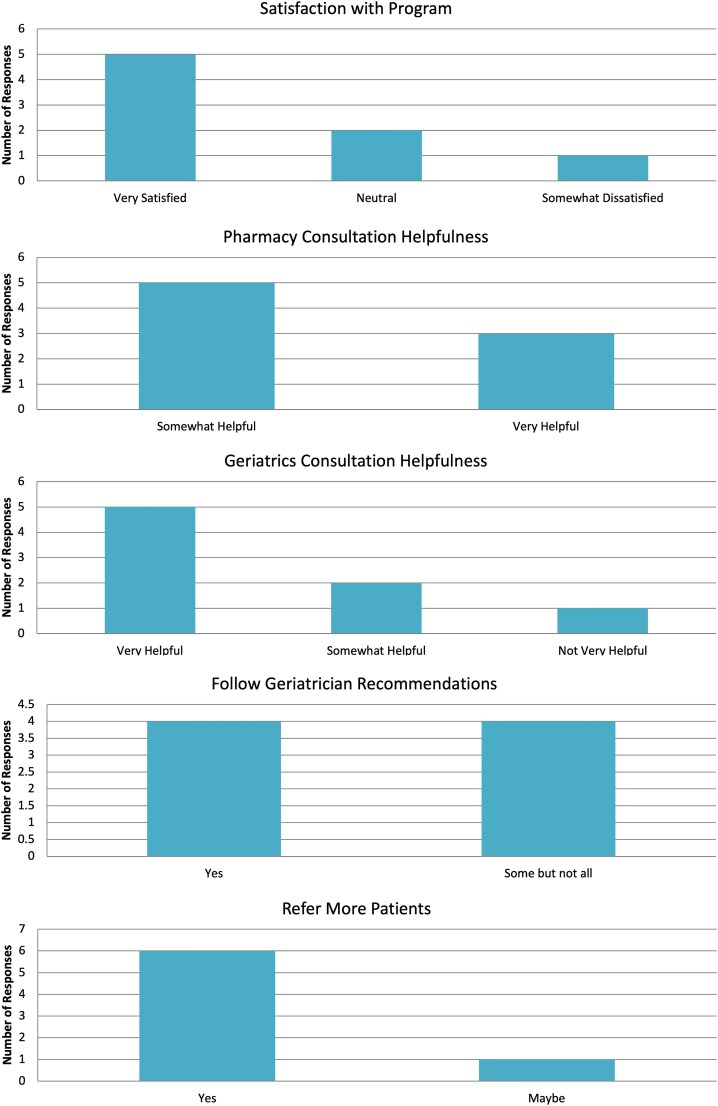 Figure 1
Figure 1| Functional Status | Preventative Care Screenings | Socioenvironmental Factors | Cognition | |
|---|---|---|---|---|
|
| Patient reports of: | Chart review for completion of: | Patient reports of: | Cognition screening tools: |
| Patient | High-Risk Medications By Beers Criteria | Drug-drug Interactions | Medication Added/altered By Geriatrician | Geriatrician Recommended Discontinuing Medication | Geriatrician Recommended Adding Medication | Geriatrician Recommended Altering Medication | Geriatrician Recommended Alternate Agent | 5-m Follow Up |
|---|---|---|---|---|---|---|---|---|
| 1 | Diazepam, quetiapine | - | Increased quetiapine, split into twice daily dosing | Provided slow and detailed diazepam taper | Vitamin D, vitamin B12 | − | − | Benzodiazepine taper, remains on quetiapine |
| 2 | − | - | - | - | - | - | - | - |
| 3 | Hydromorphone, cyclobenzaprine | … | … | Hydromorphone, cyclobenzaprine | - | - | - | Patient declined discontinuation of medications |
| 4 | Clonazepam, indomethacin, ranitidine, tizanidine | Atazanavir/ritonavir interactions with bupropion, clonazepam, clopidogrel, ranitidine, and vardenafil | - | Controlled clonazepam taper, consider SNRI/SSRI during taper | - | - | - | Patient declined benzodiazepine taper |
| 5 | Cyclobenzaprine, gabapentin, hydrocodone-acetaminophen, ibuprofen, pregabalin, tramadol, tizanidine, ziprasidone, zolpidem | - | - | Cyclobenzaprine, gabapentin, hydrocodone-acetaminophen, ibuprofen, pregabalin, tramadol, tizanidine, ziprasidone, zolpidem | - | - | - | Cyclobenzaprine and tizanidine removed from medication list |
| 6 | Hydroxyzine | - | - | - | - | Take hydroxyzine at night, switch to less sedating antihistamine if advancing age or falls | - | Changes not noted in chart |
| 7 | − | - | - | - | Add SSRI in addition to existing mirtazapine | - | - | Changes not noted in chart |
| 8 | − | Etravirine and glipizide, levothyroxine, atorvastatin | - | Consider discontinuation of icosapent ethyl | - | - | Combination HIV medication (if pill is not too large) to increase compliance | Changes not noted in chart |
| 9 | Ibuprofen, oxybutynin, ranitidine, tramadol, trazodone | - | - | Limit tramadol and trazodone | - | - | Oxybutynin to mirabegron for decreased anticholinergic effects | Changes not noted in chart |
| 10 | Eszopiclone, lorazepam, morphine, oxycodone, pregabalin | - | IV iron added | Eszopiclone or lorazepam | SNRI (duloxetine) | Vitamin B12 increased | - | Duloxetine started |
| 11 | Ibuprofen | - | - | - | Aspirin | - | Topical lidocaine or diclofenac instead of ibuprofen | Daily aspirin started |
| Patient | New Diagnosis Added | Referrals Placed | Functional Status Interventions | Preventative Care Interventions | Socioenvironmental Interventions | Cognitive/mental Health Interventions |
|---|---|---|---|---|---|---|
| 1 | - | - |
|
|
|
|
| 2 | Hearing impairment, mild cognitive impairment | ENT consult (completed) |
|
| - |
|
| 3 | - | PT vestibular rehabilitation, (completed) |
| - |
|
|
| 4 | Sleep apnea | Sleep study (completed) |
| - | - | - |
| 5 | - | Social work consult (completed) | - | - |
|
|
| 6 | - | - | - |
|
| - |
| 7 | - | Pharmacy to coordinate with home health RN (completed) | - | - |
|
|
| 8 | Frailty | Endocrinology consult (unknown if completed), |
| - |
|
|
| 9 | Dizziness, | Home OT safety eval, consider PT for dizziness (completed) |
|
| - | - |
| 10 | - | - | - |
| - |
|
| 11 | Prostate cancer | … |
|
|
|
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHIV-related health complications and treatments · HIV/AIDS Research and Interventions · Pneumocystis jirovecii pneumonia detection and treatment
Over half of the overall population of people with HIV in the US and Europe is now aged 50 years or older. As a result of multiple factors, including HIV-associated inflammation, long-term side effects of antiretroviral therapy, and socioeconomic factors, many people with HIV are experiencing syndromes commonly found in much older patients, including falls, incontinence, dementia, frailty, cardiovascular disease, and impairment in activities of daily living [1, 2]. Studies show that people with HIV experience both a higher prevalence of geriatric syndromes (ie, “accentuated aging”) as well as earlier onset of these syndromes (ie, “accelerated aging”) when compared with people without HIV [3–5]. As people with HIV become older, many may benefit from a consultation with a geriatrician. Geriatricians, physicians with additional training and expertise in the care of older adults, can offer advice on the management of geriatric syndromes, understanding goals of care, and minimizing medical interventions and treatments that may not prolong the health span [6]. Optimal strategies for implementing geriatric care in this population are not yet clear.
Multiple institutions across the US and the UK have developed clinic models to address the unique needs of the aging population of people with HIV [7]. Examples of existing models involve a consulting geriatrician via referral from an HIV provider, a joint clinic model with both HIV and geriatric providers, or a provider dually-trained in geriatrics and HIV medicine [8]. Some clinic models do not involve a geriatrician at all, and instead employ nurse-lead teams or a nurse specialist trained in geriatrics [8]. In 2018, the UCHealth Infectious Disease Clinic at the University of Colorado, Aurora, implemented an outpatient referral program called the Positive Aging Consultation program to connect high-risk older people with HIV with specialty geriatric care. Despite a relatively large pool of eligible patients, there was limited utilization of the geriatric consultation model. The purpose of this article is to describe the structure of this clinical model and discuss potential barriers that may have prevented higher participation in the program. Exploration of these barriers can provide key insights into how to improve access to geriatric care for this population.
MATERIALS & METHODS
Setting and Population
The UCHealth Infectious Disease Clinic is an outpatient infectious disease practice located within the University of Colorado, a tertiary care center located in Aurora, CO, USA. The clinic serves as a medical home for more than 2000 people with HIV, is supported by funding from the Ryan White HIV/AIDS Program and is staffed by University of Colorado School of Medicine faculty. Within the UCHealth Infectious Disease Clinic, people with HIV who are ≥50 years old were considered for referral to the Seniors Clinic, an outpatient geriatric primary care practice located on a different floor of the same building as the Infectious Disease clinic. Typically, patients must be ≥75 years of age to be seen in the Seniors Clinic, but an exception was made for the patients participating in the program [9]. During the trial period, the Infectious Disease Clinic had 903 people with HIV ≥50 years old who were eligible to access the Positive Aging Consultation program. There were no additional exclusion criteria.
Procedures
Positive Aging Consultation Program
HIV providers were encouraged to refer patients who were considered high-risk, including those with geriatric syndromes (eg, vision loss, hearing loss, urinary incontinence, mobility issues, falls history, inability to perform activities of daily living [ADLs], and inability to perform instrumental activities of daily living [IADLs]), hyper-polypharmacy (defined as taking ≥10 medications, inclusive of antiretroviral therapy) [10], multimorbidity (defined as ≥2 long-term health conditions in one individual [11]), or in need of assistance with advance care planning. Recruitment of patients occurred via emails to HIV providers, posters in the UCHealth Infectious Disease Clinic, and discussion during clinic staff meetings. Ultimately, referral to the Positive Aging Consultation program was up to the HIV provider's clinical discretion. Referrals were sent via email or through an order in the electronic health record. Additionally, pharmacy residents screened all 903 eligible patients and identified patients taking ≥10 medications and contacted them by phone or via the electronic patient portal to offer Positive Aging Consultation program visits.
During all visits to the Positive Aging Consultation program, patients were screened for four major categories including functional status, preventative care, socioenvironmental factors, and cognitive concerns/mental health using a standardized provider note template created by the consulting geriatricians with input from an HIV provider. While the provider template included prompts for the formal screening tools described in Table 1, utilization of these tools was not required for completion of a comprehensive geriatric assessment and was ultimately left to the geriatric provider's discretion.
The consulting geriatrician made clinical recommendations, including referrals, imaging studies, or alterations to medications, either via communication with the primary provider or by directly placing orders. The means by which recommendations were made was decided at the discretion of the geriatric provider depending on the nature of the recommendation and clinical context. HIV medications were not altered by the geriatric provider. Patients returned to the care of their primary HIV provider at the end of consultative services. Initial geriatrics consult visits were 60 minutes in length; 40-minute follow-up visits were scheduled at the recommendation of the geriatrician.
Payment for geriatric consultation was done through patient's insurance and was billed as a new patient consult visit (Current Procedural Technology [CPT®] codes 99204, 99205) [19].
Clinical Pharmacy Consultation
Patients taking ≥10 medications were referred for clinical pharmacy consultation, to be completed prior to the Positive Aging Consultation appointment. Patients referred for pharmacy consultation were instructed to bring all medications, both prescribed and over the counter, to their appointment with an infectious disease pharmacist. Visits were conducted within the HIV clinic. Pharmacists performed a detailed assessment of the patient's current medications, with special attention to drug-drug interactions, medications that could potentially be discontinued, or potentially inappropriate medications as identified by Beers Criteria (an explicit list from the American Geriatric Society of potentially inappropriate medications that should typically be avoided in older individuals) [20]. These recommendations were available to the geriatrician to incorporate into the consult visit. All patients who underwent clinical pharmacy consultation also underwent geriatrician consultation.
Data Collection
Written consent was obtained from patients and providers to participate in data collection and follow-up surveys. Data was collected via chart review of all geriatric and pharmacy notes, referrals placed, and follow-up notes with the primary HIV provider or other members of the interdisciplinary team. In addition to functional status, preventative care, socioenvironmental factors, and cognitive/mental health concerns described above, data collection included demographic data (gender, race, ethnicity, and membership in a vulnerable group defined as prisoner, cognitively impaired, other), general medical data (vital signs, number of hospitalizations, number of HIV visits in preceding year, substance use, comorbidities), and HIV status (year of diagnosis, most recent CD4 count and viral load, FIB-4 score, Veterans Aging Cohort Study [VACS] index score, and current HIV medications). A 5-month chart review was performed to document primary provider visits since geriatric consultation and implementation of geriatrician recommendations. Data was recorded in a secure REDCap database. Primary HIV providers were asked to perform a follow-up survey of the Senior Clinic visit, which included overall satisfaction with the geriatric and pharmacy consultation, likelihood of implementing consultant recommendations, and likelihood of referring patients to the program in the future. Analysis of the data was primarily descriptive. Means and standard deviation were used for the description of numerical data elements. Colorado Multiple Institutional Review Board approval was obtained for this study under protocol number 17–2160.
RESULTS
Participants
Between January 2018 to July 2019, of the 903 patients eligible for the referral program, 11 patients were seen in the Positive Aging Clinic. One patient was scheduled but did not arrive to their appointment. The mean patient age was 69 years of age (SD = 7.7; range 58.9–80.3). Patient-identified gender included male (n = 6, 54%) and female (n = 5, 45%). Patient self-described race included Black or African American (n = 3, 27%), White (n = 4, 36%), and unknown/unreported (n = 4, 36%). Patient self-described ethnicity included Hispanic or Latino (n = 2, 18%), not Hispanic or Latino (n = 8, 72%), or unknown/not reported (n = 1, 9%). Patient insurance coverage included Medicare (n = 9, 82%), Medicaid (n = 4, 36%), or both Medicare and Medicaid (n = 3, 27%). Patient employment status included employed (n = 1, 9%), retired (n = 2, 18%), or unknown (n = 8, 72%). Patient-reported use of substances included tobacco (prior cigarette use: n = 5, 45%; current cigarette use: n = 2, 18%; no tobacco use: n = 4, 36%), medical marijuana use (n = 2, 18%), and current cocaine use (n = 1, 9%). No patients reported prior IV (intravenous) drug use, and no patients were uninsured or unhoused. No patients were identified as being members of a vulnerable population. All 11 patients were English-speaking. Additional detailed health data has been omitted to protect patient confidentiality due to the low number of participants. Two faculty geriatricians and one geriatric fellow were involved in the consultative care of these patients. The median number of patient visits with a geriatric provider was 1 (range 1–3).
Medication Changes
All 11 patients were prescribed ≥10 medications and were also referred for pharmacy consultation. The mean number of prescribed medications was 17.7; SD = 7.6; range 10–33. During the pharmacist consultation, two patients had high-risk drug-drug interactions identified. During geriatric consultation, there were 6 episodes of recommending or adding new medications, 6 episodes of recommending alteration to an existing medication, and 18 episodes of recommending discontinuing medications. There were 3 episodes of discontinuation or alteration of medications as recommended by geriatrician (16% of total recommendations) at 5-month follow up. Details of medication changes are described in Table 2.
Summary of Topics Addressed During Geriatrics Consultation
All non-pharmacologic interventions performed during consultation visits are detailed in Table 3. Geriatric assessments performed included timed get-up-and-go (n = 7, 64%), PHQ-2 (n = 5, 45%), Montreal Cognitive Assessment (MOCA) (n = 4, 36%), Mini-Cog (n = 3, 27%), GAD-7 (n = 1, 9%), and grip strength testing (n = 1, 9%). Additional interventions included discussion of advanced care planning (n = 11, 100%), addition of new diagnoses/problems to patient's problem list (n = 5, 45%), referral to other health services (n = 4, 36%), and referral to community-based services such as Meals on Wheels (n = 3, 27%). Specific recommendations were provided by the geriatrician to the patient or primary HIV provider for osteoporosis screening (n = 6, 54%), memory problems (n = 5, 45%), mental health (n = 5, 45%), hearing loss (n = 3, 27%), falls (n = 2, 18%), nutrition/weight loss (n = 2, 18%), urinary incontinence (n = 1, 9%), cancer screening (n = 1, 9%), elder abuse (n = 1, 9%), and mobility (n = 1, 9%). Recommendations included referral for bone mineral density testing or re-initiation of bisphosphonate therapy for osteoporosis, discontinuation of centrally acting medications for memory problems, referral to audiologist or otolaryngology for cerumen disimpaction for hearing loss, referral to vestibular physical therapy or home occupational therapy for falls, referral to social work for weight loss related to food insecurity, and referral to endocrinology for uncontrolled hypothyroidism and diabetes. On chart review at 5 months, 7 geriatrician recommendations related to functional status had been completed (64%); 6 recommendations related to preventative care had been completed (60%); 5 recommendations related to socioenvironmental interventions had been completed (63%); and 6 recommendations related to cognition/mental health had been completed (n = 5, 45%) or partially completed (n = 1, 9%). Out of 10 provider or community referrals recommended or placed, 7 (70%) had been ordered, scheduled or completed at the time of follow up.
Primary Provider Satisfaction
Responses were recorded from HIV providers regarding the experience of each patient they referred for geriatric consultation. A total of 8 surveys were completed from 6 unique providers (1 infectious disease nurse practitioner, 5 infectious disease physicians). The responses are summarized in Figure 1. Overall, providers reported being very satisfied (n = 5, 56%), neutral (n = 2, 22%), or somewhat dissatisfied (n = 1, 11%) with the program. Providers found the pharmacy consultation to be very helpful (n = 2, 22%) or somewhat helpful (n = 4, 44%), and the geriatrics consultation to be very helpful (n = 5, 56%), somewhat helpful (n = 2, 22%), or not very helpful (n = 1, 11%). Almost all providers reported that they would follow-through with geriatrician recommendations (“yes” [n = 4, 44%]; “some, but not all” [n = 4, 44%]), and almost all providers reported that they would refer more patients for Positive Aging Consultation (“yes” [n = 7, 78%]; “maybe” [n = 1, 11%]). Narrative comments noted satisfaction with quick appointment times and the identification of several new screenings for a patient. One provider noted that their patient enjoyed the experience but is generally resistant to changes to their medications. One provider wished they had been provided more specific recommendations for medication tapering.
Summary of HIV providers' survey responses. caption: Summary of HIV providers' responses (n = 9) regarding their experiences with the geriatric consultation program. Bars represent the number of providers selecting each response across five domains: overall satisfaction with the program, perceived helpfulness of pharmacy and geriatrics consultations, likelihood of following geriatrician recommendations, and willingness to refer additional patients. Providers generally reported high satisfaction, found consultations helpful, and indicated strong intent to implement recommendations and refer future patients.
DISCUSSION
The Positive Aging Consultation program resulted in 11 people with HIV from the UCHealth Infectious Disease Clinic receiving outpatient consultation from a clinical pharmacist and a geriatric specialist. The program supported a dedicated medication review and access to specialist care for patients who would typically have limited access to geriatric evaluation, based on the age cutoff of 75 years at the Seniors Clinic (80% < 75 years) [9]. Patients benefitted from longer appointment times than a typical HIV clinic visit, which allowed for identification of high-risk medications, referrals to other specialists or services, and recommendations for issues related to functional status, preventative care, socioenvironmental factors, and cognitive concerns/mental health. Providers were satisfied overall with the program and likely to refer patients in the future. Despite these positive outcomes, the most notable outcome of this study was the overall limited utilization of the consultation service, which prompted us to consider barriers to geriatric consultation in people with HIV.
One barrier to implementation of the geriatric consultation model may be the lack of patient and provider awareness of or consensus on the utility of geriatric consultation, particularly in patients who may not self-identify as “geriatric”. The geriatric consultation program represented a comprehensive geriatric assessment (CGA), which can be defined as a multidimensional, multidisciplinary assessment of an older person's functional ability, physical health, cognition, and socioenvironmental circumstances [21]. Studies have shown that CGAs have been linked to improved survival, connection to care, functional status, and quality of life, as well as decreased caregiver burden and hospital readmission rates in older adults [22–25]. Various specialties and subspecialties, including surgery, cardiology, nephrology, and oncology, have shown improvement in outcomes and quality of life with the implementation of CGAs [26–34]. In fact, CGA was shown to be so beneficial in decreasing chemotherapy-related toxicity, surgical complications, and poor functional status in oncology patients that the American Society of Clinical Oncology guidelines now recommend CGA for all older patients undergoing cancer treatment [35].
Regarding CGA for HIV, existing guidelines address components of management of the aging HIV population. In 2011, the American Geriatrics Society, the American Academy of HIV Medicine, AIDS Community Research Initiative of America jointly released the first guidelines for treatment of older HIV patients [36]. Since then, the Department of Health and Human Services, the International Antiviral Society-USA, and the Infectious Diseases Society of America have added sections on caring for aging people with HIV to their guidelines [37–39]. Implementation of geriatric care for HIV patients, however, remains limited, and a gold-standard model of care for this population has not yet been defined [7, 8].
Because we only conducted surveys of referring providers, we do not know exact reasons why some HIV providers did not participate in the program. We suspect that the lack of an integrated, co-located clinic for geriatric care was another barrier. Despite the Seniors Clinic being in the same building as the Infectious Disease clinic, the need for a separate referral and establishing care in a new clinic likely served as a deterrent to participation in the program. Furthermore, providers often forgot that the consultation service existed without the regular presence of a geriatrician in the clinic. Indeed, a systematic review found that co-located models of HIV and non-HIV medical care had improved linkage to care and antiretroviral therapy outcomes compared to other models [40]. Integrated, multidisciplinary care has been associated with decreased hospitalizations, reduced duplicate testing, and lower healthcare costs for people with HIV [41]. Furthermore, a 2023 survey of people with HIV in the University of Colorado Infectious Disease clinic found that less than half (46%) of responders would be very likely to see a provider that specializes in aging, while 61% would be very likely, if the provider was located within the HIV clinic itself [42]. As such, future models may benefit from a co-located approach to geriatric care to improve patient and provider participation. Notably, with the increased prevalence of telehealth spurred by the COVID-19 pandemic, internet-based models of care may potentially be utilized to optimize delivery of integrated care [43].
We suspect that success in de-prescribing would have driven more referrals. Polypharmacy is commonly encountered among older adults with HIV and contributes to increased risks of falls and frailty [38]. Hyper-polypharmacy was present in all people referred for geriatric consultation in our clinic setting and many medication discontinuation or alteration recommendations were made. However, patients frequently declined these changes: only two medications were removed from a medication list after 5 months, and one benzodiazepine taper was ongoing. This lack of follow-through with geriatric recommendations has been echoed in other studies of HIV patients. For example, a retrospective cohort study of a geriatric consultation model at a New York HIV clinic cited only 32.4% adherence to geriatrician recommendations regarding medications [44]. Multiple systematic reviews have described a variety of barriers to successful medication de-prescribing including fragmented care among multiple providers, high clinical complexity, time restraints, and incomplete information regarding rationales for prescription of certain drugs [45–47]. Many providers lack training or familiarity with tapering and monitoring medications, or may fear potential consequences of de-prescribing, such as withdrawal or undertreatment [48]. Developing clear guidance and demonstrating effective de-prescribing may improve perceived benefits of geriatric consultation.
A major barrier to implementing geriatric care for people with HIV within any healthcare system is the national shortage of geriatricians. The Health Resources and Services Administration predicts that there will be a 50% increase in demand for geriatricians between 2018–2030 in the U.S., and the supply of geriatricians will decrease slightly in that time [49]. As the population ages, access to specialized geriatric care will be difficult even for people ≥75 years of age [49–51]. A thorough geriatric assessment is time-consuming for consulting providers and pharmacists, and many geriatric clinics may lack the ability to expand their patient population to include regular subspecialty consultations [50]. Because of the limited access to specialty geriatric care, all clinicians will need to develop basic skills in how to care for older adults [51, 52]. Dedicated training in geriatric care for HIV providers, or HIV certification for geriatric providers, may be an effective, cost-effective, and efficient way to expand geriatric care to people with HIV [7].
Lastly, financial concerns are often considered a major barrier in implementing geriatric consultation in many settings. Indeed, a barrier for co-location in the present study was the inability for the geriatrician to bill if physically seeing a patient within the HIV clinic. Any visits outside of the geriatric clinic were essentially volunteered [7]. Geriatricians are often viewed by insurers as primary care providers rather than consulting specialists, which may cause confusion around reimbursement and coverage [7, 53, 54]. For instance, the Centers for Medicare & Medicaid Services may not provide reimbursement if a patient has multiple visits for the same services in a single day [7]. Despite multiple benefits of integrated care as discussed above, billing regulations may prevent patients from seeing multiple specialists (ie, infectious disease and geriatrics) in one single integrated clinic [54]. Potential solutions to these financial constraints include the ability to reimburse specialty care for patients who lack adequate insurance coverage, training members of the HIV clinic team to perform some or all of the CGA as part of usual HIV care, or establishing practice agreements that allow geriatricians to bill as an extension of the HIV care team.
Limitations of our study include a small sample size and a single clinical site, which limits generalizability. The follow-up time was 5 months, which is likely insufficient to draw significant conclusions regarding patient outcomes. The study also lacks robust data regarding patients' perspectives on their experience with geriatric consultation, which will be a valuable component to consider in future studies and has been collected in a separate study [42]. However, we provide a detailed account of clinical interventions resulting from geriatric evaluation and reveal limitations to the clinical model in real-world practice. Barriers to geriatric care in our setting highlight opportunities for improvement in future care models.
CONCLUSION
The Positive Aging Consultation program served as an initial step towards addressing the needs of the aging population of people with HIV in the University of Colorado Infectious Disease Clinic. Despite limited participation of patients and providers, we identified key barriers that face implementation of geriatric care for people with HIV. Recognition of these barriers is essential to designing more scalable models of care moving forward. Future efforts should focus on strategies to mitigate these barriers, which may include educational efforts surrounding the benefits of comprehensive geriatric assessments, more integrated and inclusive clinical models, and working with institutions and insurance to ensure available funding for these endeavors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Smit M, Brinkman K, Geerlings S, et al Future challenges for clinical care of an ageing population infected with HIV: a modelling study. Lancet Infect Dis 2015; 15:810–8.10.1016/S 1473-3099(15)00056-0PMC 452807626070969 · doi ↗ · pubmed ↗
- 2Negredo E, Back D, Blanco JR, et al Aging in HIV-infected subjects: a new scenario and a new view. Bio Med Res Int 2017; 2017:5897298.29430462 10.1155/2017/5897298 PMC 5753008 · doi ↗ · pubmed ↗
- 3Althoff KN, Mc Ginnis KA, Wyatt CM, et al Comparison of risk and age at diagnosis of myocardial infarction, end-stage renal disease, and non-AIDS-defining cancer in HIV-infected versus uninfected adults. Clin Infect Dis 2015; 60:627–38.25362204 10.1093/cid/ciu 869PMC 4318916 · doi ↗ · pubmed ↗
- 4Guaraldi G, Orlando G, Zona S, et al Premature age-related comorbidities among HIV-infected persons compared with the general population. Clin Infect Dis 2011; 53:1120–6.10.1093/cid/cir 62721998278 · doi ↗ · pubmed ↗
- 5Schouten J, Wit FW, Stolte IG, et al Cross-sectional comparison of the prevalence of age-associated comorbidities and their risk factors between HIV-infected and uninfected individuals: the AG Eh IV cohort study. Clin Infect Dis 2014; 59:1787–97.25182245 10.1093/cid/ciu 701 · doi ↗ · pubmed ↗
- 6Kotsani M, Kravvariti E, Avgerinou C, et al The relevance and added value of geriatric medicine (GM): introducing GM to non-geriatricians. J Clin Med 2021; 10:3018.34300184 10.3390/jcm 10143018 PMC 8304813 · doi ↗ · pubmed ↗
- 7Davis AJ, Greene M, Siegler E, et al Strengths and challenges of Various models of geriatric consultation for older adults living with human immunodeficiency virus. Clin Infect Dis 2022; 74:1101–6.10.1093/cid/ciab 682PMC 894677434358303 · doi ↗ · pubmed ↗
- 8Kokorelias KM, Grosse A, Zhabokritsky A, Sirisegaram L. Understanding geriatric models of care for older adults living with HIV: a scoping review and qualitative analysis. BMC Geriatr 2023; 23:417.10.1186/s 12877-023-04114-7PMC 1032935137422631 · doi ↗ · pubmed ↗