Professional fulfillment in interventional radiology
Lindsay Eysenbach, Mark Loper, Gabe Li, David S. Shin, Eric J. Monroe, Matthew Abad-Santos, Eunjee Lee, Hyeonjeong Lim, Anthony Hage, Jeffrey Forris Beecham Chick, Mina S. Makary

TL;DR
This study explores job and career satisfaction among interventional radiologists, finding that professional fulfillment is low despite some positive factors like patient interaction.
Contribution
The paper introduces a validated assessment of professional fulfillment in interventional radiology, a field previously understudied.
Findings
Only 50% of interventional radiologists reported high global specialty satisfaction.
Job and career satisfaction scores were lower, with 35.8% of respondents indicating satisfaction.
Patient interaction and work-life balance were identified as key factors influencing professional fulfillment.
Abstract
There have been several analyses conducted demonstrating a sharp decrease in general physician fulfillment and satisfaction. Other studies have demonstrated that burnout, anxiety, and moral injury are prevalent among interventional radiologists specifically, however there is a paucity of literature examining professional fulfillment within the profession. The purpose of this study was to characterize professional fulfillment through job, career, and specialty satisfaction scores among interventional radiologists using a validated assessment tool. There were 106 respondents included in the analysis: 97 (91.5%) practicing interventional radiologists and 9 (8.5%) interventional radiology trainees, including 87 (82.1%) males and 19 (17.9%) females. Respondents included those in academic (40; 37.7%), private practice (46; 43.4%), and hybrid/other settings (20; 18.9%), as well as at various…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
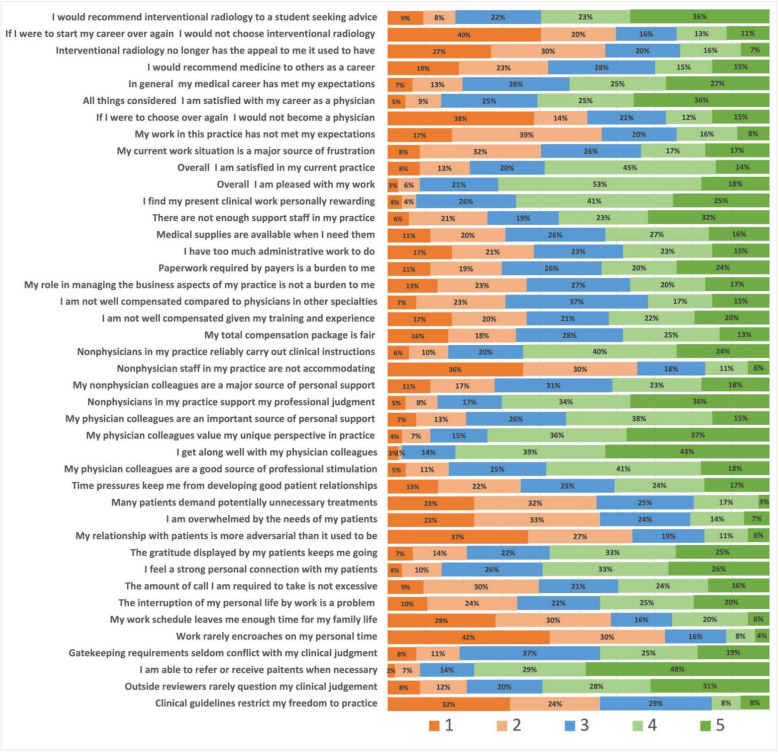 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRadiology practices and education · Healthcare professionals’ stress and burnout · Diversity and Career in Medicine
Background
Professional fulfillment is made up of the levels of satisfaction one holds in their job, career, and specialty. As described by Brown & Gunderman, satisfaction is a term used for an activity being sufficient on a surface level, whereas fulfillment is a holistic feeling of accomplishment and completion [1]. Among physicians, these intersecting ideas have garnered attention due to their direct association with healthcare outcomes, patient happiness, and physician burnout. As an example, a survey conducted by Al Rekabi et al., similar to the one detailed here, found an increase in burnout among UK-based interventional radiologists alongside high levels of emotional exhaustion, depersonalization, and lack of personal accomplishment [2]. Follow-up dialogues regarding this important paper lend astute insight into potential alternate approaches and solutions of this complex problem, such as the differing yet synergistic views of Uberoi et al. and Reekers on the importance of increasing workforce in the field vs recognizing the lack of independence of the field itself and how that contributes a multidomain approach to burnout [3, 4]. Other previous works in addition to these conclude a physician’s satisfaction and well-being, or lack thereof, permeates into his or her encounters with patients, thus affecting more than solely the provider’s mood [1, 5–8]. Professional fulfillment considers additional factors alongside burnout in addressing this growing problem. Various frameworks have been validated to characterize and assess professional fulfillment as it pertains to physicians specifically separate from prior burnout assessments [5]. Specialty-agnostic assessment tools that define specific domains of physician experiences (relationships with patients, pay, administration, etc.) have been utilized to examine how these individual domains correlate with overall job, career, and specialty satisfaction [9, 10].
There have been several analyses conducted demonstrating a sharp decrease in general physician fulfillment and satisfaction [5]. Other studies have demonstrated that burnout, anxiety, and moral injury are prevalent among interventional radiologists specifically, however there is a paucity of literature examining professional fulfillment within the profession [11–13]. The aim of this study was to characterize professional fulfillment, as well as its potential origins, among interventional radiologists using a validated assessment tool.
Methods
Study population and data collection
This Health Insurance Portability and Accountability Act (HIPAA)-compliant study was exempt from Institutional Review Board (IRB) approval based on institutional assessment of criteria listed in 45 CFR 46.101(b). The study was assessed using STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) guidelines [14]. This survey was disseminated between September 23, 2023 and October 14, 2023 (22 days). The survey was shared multiple times using social media platforms (i.e. X, San Francisco, CA; Facebook, Menlo Park, CA; LinkedIn, Sunnyvale, CA) and society-wide communications (Society of Interventional Radiology Connect, Fairfax, VA). Multiple direct contacts via electronic mail augmented recruitment efforts.
Survey design and evaluation
An anonymous 54-question survey was created using Google Forms (Google; Mountain View, CA). The first section contained 11 questions related to demographics and practice environments. The second section contained 42 questions using a 5-point Likert scale from a previously validated physician satisfaction survey [9, 10]. Following the model of previous researchers [15], six questions not applicable to interventional radiology were removed for clarity (e.g. “Formularies or prescription limits restrict the quality of care I provide”). The final component of the survey included eight specific domains which contribute to patient satisfaction (i.e. relationships with colleagues, relationships with non-physician staff, relationships with patients, personal time, pay, autonomy, administration, and resources), as well as global measures of job, career, and specialty satisfaction. There was also an optional opportunity for open-ended comments at the end of the survey. Practicing interventional radiologists and current interventional radiology trainees were eligible to participate in the study. There were no incomplete submissions as answers to all questions except an optional free-response question were mandatory for survey submission.
Measures and definitions
For the purposes of this study, and in keeping with prior literature, the term professional fulfillment refers to an umbrella term consisting of three individual measures: job satisfaction, career satisfaction, and specialty satisfaction [16]. Job satisfaction refers to the extent to which an individual is satisfied with their current job [16]. Career satisfaction refers to satisfaction with general career trajectory (i.e. work-related experiences). Specialty satisfaction refers to satisfaction with medical specialty (i.e. interventional radiology) [16].
Statistical analyses
Statistical analyses were performed by two statisticians (EL, HL). Cronbach's alpha was calculated for questions within each satisfaction domain, with Cronbach’s alpha > 0.70 considered adequate reliability. There were three domains with Cronbach’s alpha < 0.70 (autonomy, administration, and resources); therefore, each question in this domain was analyzed separately (Table 1). Table 1. Cronbach's alphaCategoryCronbach’s alphaAutonomy0.58Personal time0.77Relationships with patients0.77Relationships with colleagues0.84Relationships with staff0.86Pay0.74Administration0.59Resources0.59Global job satisfaction0.86Global career satisfaction0.89Global specialty satisfaction0.91
Mean satisfaction score was analyzed for each professional fulfillment domain, and a satisfaction “ratio” was generated. A satisfaction score of 4 or 5 on a 5-point Likert scale was considered “satisfied,” based on prior work [17].
Pearson’s correlation analysis was performed between each satisfaction domain and global measures of satisfaction, with p < 0.05 considered statistically significant. Univariate logistic regression was fitted to see the relationship between job satisfaction and relevant variables. To resolve a false positive problem in the multiple testing, Bonferroni correction was performed, and the significance level was adjusted as 0.00385.
Finally, multivariate logistic regression was performed. Some variables were excluded due to high correlation and explored fitting for a full model. However, interpreting regression coefficients became challenging, particularly due to values such as “prefer not to say” in the gender variable, which essentially represent missing data. Therefore, analysis was conducted for the remaining 112 individuals, excluding those who chose “prefer not to say”. Additionally, “unsure” and “no” responses for the “Do you have an institutional practice…” item were combined to create a broader yes/no category. After identifying that the coefficient and odds ratio values for “International” in the “Location of practice” variable were exceptionally large, six observations were excluded to facilitate interpretation. After these refinements, the final number of respondents included in the analysis was 106.
Results
Demographics
Of 106 respondents included in the analysis, 97 (91.5%) were practicing interventional radiologists and 9 (8.5%) were interventional radiology trainees. Ninety-three (82.1%) of the respondents were male, and the majority (n = 63, 59.4%) were white. Respondents included practicing interventional radiologists from different career stages: 21 (19.8%) with practice experience of < 5 years, 19 (17.9%) with 6–10 years, 20 (18.9%) with 11–20 years, and 36 (34.0%) with > 20 years. Additional demographic data are shown in Table 2. Table 2. Demographic and practice characteristics**Category****N (%)**Current level of practiceRadiology trainee9 (8.5%)Radiologist97 (91.5%)GenderFemale19 (17.9%)Male93 (82.1%)EthnicityAsian21 (19.8%)White63 (59.4%)Others23 (20.8%)Location of practiceMidwest23 (21.7%)Northeast25 (23.6%)Southeast20 (18.0%)Southwest11 (10.4%)West27 (25.5%)Practice settingAcademic40 (37.7%)Hybrid/Other20 (18.9%)Private46 (43.4%)Practice in > 1 hospital/setting?Yes69 (65.1%)No37 (34.9%)Institutional leadership position?Yes59 (55.7%)No47 (44.3%)Years in practiceTrainee10 (9.4%) < 5 years21 (19.8%)6–10 years19 (17.9%)11–20 years20 (18.9%) > 20 years36 (34.0%)Time spent reading diagnostic studies < 25%37 (34.9%)25–49%19 (17.9%)50–75%3 (2.8%) > 75%1 (0.9%)None46 (43.4%)Time dedicated to administrative tasks < 25%66 (62.3%)25–49%11 (10.4%)None29 (27.4%)
Practice environments
Respondents practiced in academic (n = 40, 37.7%), private (n = 46, 43.4%), and hybrid/other (n = 20, 18.9%) environments. A majority of respondents (n = 60, 56.6%) did spend some time reading diagnostic studies, but only 4 (3.8%) spent > 50% of their time reading diagnostic studies. A majority (n = 59, 55.7%) reported holding leadership positions. A larger majority (n = 77, 72.6%) spent at least some time on administrative duties, with 13 (12.6%) reported spending > 25% of their time on these duties. Additional practice characteristics data are shown in Table 2.
Professional fulfillment
Mean global job satisfaction score was 3.48; 38 (35.8%) of respondents reported a satisfaction score of ≥ 4. Mean global career satisfaction score was 3.40; 38 (35.8%) of respondents reported a satisfaction score ≥ 4. The mean global specialty satisfaction score was 3.62, with 53 (50.0%) respondents reporting satisfaction score ≥ 4. *Full non-demographic, non-practice-related survey results can be seen in Fig. 1. * Fig. 1. Likert scale results by query in second section of survey
Univariate analysis
Correlation analysis demonstrated a positive correlation between job, career, and specialty satisfaction and the composite satisfaction domains with high reliability (i.e. Cronbach’s alpha > 0.70): relationships with colleagues, relationships with staff, relationships with non-physician staff, personal time, and pay. *Additional results are shown in *Table 3. Table 3. Pearson’s correlation analysisGlobal job satisfactionGlobal career satisfactionGlobal specialty satisfactionRelationships with colleagues0.60(< 0.001)*0.46(< 0.001)*0.48(< 0.001)*Relationships with patients0.60(< 0.001)*0.63(< 0.001)*0.53(< 0.001)*Relationships with non-physician staff0.55(< 0.001)*0.36(< 0.001)*0.44(< 0.001)*Personal time0.54(< 0.001)*0.48(< 0.001)*0.31(< 0.001)*Pay0.48(< 0.001)*0.46(< 0.001)*0.28(< 0.001)Autonomy Clinical guidelines restrict my freedom to practice−0.21(0.03)−0.24(0.01)−0.05(0.64) Outside reviewers rarely question my professional judgements0.32(< 0.001)0.34(< 0.001)0.21(0.03) I am able to refer patients or receive referrals when necessary0.30(< 0.001)0.31(< 0.001)0.29(< 0.001) Gatekeeping requirements seldom conflict with my clinical judgment0.22(0.03)0.17(0.08)0.08(0.42)Administration My role in managing the business aspects of my practice is not a burden to me0.34(< 0.001)0.31(< 0.001)0.32(< 0.001) Paperwork required by payers is a burden to me−0.28(0.01)−0.35(< 0.001)−0.28(< 0.001) I have too much administrative work to do−0.38(< 0.001)−0.43(< 0.001)−0.38(< 0.001)Resources Medical supplies are available when I need them0.44(< 0.001)0.23(0.03)0.27(< 0.001) There are not enough support staff in my practice−0.28(< 0.001)−0.17(0.05)−0.07(0.50)^^Significant result. To resolve a false positive problem in the multiple testing, Bonferroni correction was performed and the significance level was adjusted to p < 0.0036
Logistic regression demonstrated a positive correlation between job, career, and specialty satisfaction and all composite domains analyzed, with the exception of career satisfaction and relationship with non-physician staff. Additional results are shown in Table 4. Table 4. Logistic regression (Odds ratio)Global job satisfactionGlobal career satisfactionGlobal specialty satisfactionRelationships with colleagues1.42(< 0.001)*1.38(< 0.001)*1.35(< 0.001)*Relationships with patients1.33(< 0.001)*1.40(< 0.001)*1.31(< 0.001)*Relationships with non-physician staff1.26(< 0.001)*1.15(0.016)1.21(< 0.001)*Personal time1.35(< 0.001)*1.28(< 0.001)*1.20(0.002)*Pay1.40(< 0.001)*1.35(< 0.001)*1.20(0.008)*Clinical guidelines restrict my freedom to practice0.60(0.009)0.76(0.126)1.07(0.689)Outside reviewers rarely question my professional judgements2.01(< 0.001)*1.33(0.092)1.25(0.150)I am able to refer patients or receive referrals when necessary1.25(0.298)1.67(0.030)1.35(0.131)Gatekeeping requirements seldom conflict with my clinical judgment1.56(0.023)1.40(0.078)1.11(0.550)My role in managing the business aspects of my practice is not a burden to me0.42(0.011)*0.42(0.011)*0.46(0.004)*Paperwork required by payers is a burden to me0.74(0.053)0.65(0.008)0.80(0.142)I have too much administrative work to do0.69(0.021)0.50(< 0.001)*0.62(0.003)*Medical supplies are available when I need them2.18(< 0.001)1.28(0.148)1.41(0.037)There are not enough support staff in my practice0.71(0.032)0.78(0.125)0.89(0.449)^^Significant result. To resolve a false positive problem in the multiple testing, Bonferroni correction was performed and the significance level was adjusted to p < 0.0036
Multivariate logistic regression
In terms of demographics, no variables met statistical significance on multivariate analysis. There was a positive correlation between global job satisfaction and domains of personal time (p = 0.017) and relationships with patients (p = 0.034); there was also a statistically significant relationship with two questions within the “autonomy domain” (“Clinical guidelines restrict my freedom to practice,” “Outside reviewers rarely question my professional judgements”). There was a positive trend between global job satisfaction and pay that did not meet statistical significance (p = 0.064).
Similarly, there was a positive correlation between global career satisfaction and personal time (p = 0.043) and relationship with patients (p = 0.034); there was also a statistically significant correlation with pay (p = 0.047). Analysis of global specialty satisfaction only found a statistically significant correlation with relationships with patients (p = 0.001). Full results are available in Tables 5, 6 and 7. Table 5. Multivariate logistic regression: global job satisfactionCoefficient****Odds-ratiop**-valueClinical guidelines restrict my freedom to practice−1.9330.140.042Gatekeeping requirements seldom conflict with my clinical judgment−0.9670.380.395I am able to refer patients or receive referrals when necessary−0.4360.650.418Outside reviewers rarely question my professional judgements1.9156.790.037Personal time3.37929.30.017Relationships with patients3.17423.90.034Relationships with colleagues0.0151.010.988Relationships with staff0.5811.790.673Pay2.1658.720.064My role in managing the business aspects of my practice is not a burden to me0.5221.690.315Paperwork required by papers is a burden to me0.4821.620.460I have too much administrative work to do0.6571.930.322Medical supplies are available when I need them0.1071.110.867There are not enough support staff in my practice−0.3690.690.543Current level of practice (practicing interventional radiologist)−5.6250.000.101Gender (Male)2.66514.40.157Ethnicity (Others)−0.0860.920.968Ethnicity (White)−0.7400.480.735Location of Practice Northeast−0.4730.620.800 Southeast−2.8440.060.291 Southwest0.4981.640.822 West−1.1770.310.586Description of practice Hybrid + Other−2.9330.050.235 Private−0.8710.420.640 Practicing in more than one hospital setting (Yes)2.59313.370.174 Having an institutional practice leadership position (Yes)3.98453.740.048 How many years have you been in practice0.0081.010.943What percentage of your daily work is reading diagnostic studies > 75%−1.3810.251.000 *25–49%*1.3082.820.537 *50–75%*3.59736.500.902 None4.42683.590.085What percentage of your time is dedicated to administrative non clinical duties 25–49%−5.3670.000.110 None−1.9450.140.343Table 6Multivariate logistic regression: global career satisfactionCoefficientOdds-ratiop-value**Clinical guidelines restrict my freedom to practice0.5491.730.276Gatekeeping requirements seldom conflict with my clinical judgment−0.3240.720.671I am able to refer patients or receive referrals when necessary0.5241.690.299Outside reviewers rarely question my professional judgements−0.8580.420.070Personal time1.5024.490.043Relationships with patients3.17423.90.034Relationships with colleagues1.7315.640.148Relationships with staff−0.3830.680.596Pay1.3033.680.047*My role in managing the business aspects of my practice is not a burden to me0.7192.050.114Paperwork required by papers is a burden to me−0.6270.530.200I have too much administrative work to do−0.4930.670.382Medical supplies are available when I need them−0.6190.540.219There are not enough support staff in my practice−0.2180.800.672Current level of practice (practicing interventional radiologist)−0.1140.320.639Gender (Male)0.4801.620.686Ethnicity (Others)−0.3160.040.088Ethnicity (White)−0.4530.010.023Location of Practice Northeast1.1893.280.023 Southeast1.1893.280.427 Southwest1.6755.340.252 West0.8852.420.626Description of practice Hybrid + Other0.7932.210.653 Private−0.2510.080.155 Practicing in more than one hospital setting (Yes)−0.3340.710.751 Having an institutional practice leadership position (Yes)1.9527.040.071 How many years have you been in practice0.0001.000.990What percentage of your daily work is reading diagnostic studies > *75%*9.69716,267.800.997 25–49%−0.6570.520.655 *50–75%*4.33776.460.745 None−2.6770.070.070What percentage of your time is dedicated to administrative non clinical duties *25–49%1.5654.780.346 None−0.9370.390.519^^Significant result. To resolve a false positive problem in the multiple testing, Bonferroni correction was performed and the significance level was adjusted to p < 0.0036Table 7Multivariate logistic regression: global specialty satisfactionCoefficient***Odds-ratiop-value**Clinical guidelines restrict my freedom to practice0.3081.360.327Gatekeeping requirements seldom conflict with my clinical judgment−0.4110.660.427I am able to refer patients or receive referrals when necessary−0.0430.960.896Outside reviewers rarely question my professional judgements−0.1020.900.755Personal time0.1291.140.762Relationships with patients2.1858.890.001Relationships with colleagues1.0812.950.074Relationships with staff0.2721.310.566Pay−0.0610.940.867My role in managing the business aspects of my practice is not a burden to me0.5431.720.079Paperwork required by papers is a burden to me0.0951.100.754I have too much administrative work to do−0.3000.740.347Medical supplies are available when I need them0.3071.360.315There are not enough support staff in my practice0.2261.250.461Current level of practice (practicing interventional radiologist)−0.6490.530.713Gender (Male)0.3911.480.637Ethnicity (Others)0.0561.060.956Ethnicity (White)−0.3980.670.671Location of Practice Northeast−1.3310.260.191 Southeast−0.2350.790.809 Southwest−1.1030.330.439 West0.3611.430.731Description of practice Hybrid + Other0.9252.520.403 Private−0.3810.680.670 Practicing in more than one hospital setting (Yes)−0.9840.370.198 Having an institutional practice leadership position (Yes)−0.0800.920.907 How many years have you been in practice0.0151.010.752What percentage of your daily work is reading diagnostic studies > *75%*13.8471,031,846.70.997 *25–49%*0.7462.110.418 50–75%−17.7110.000.991 None0.0281.030.974What percentage of your time is dedicated to administrative non clinical duties *25–49%1.3613.900.270 None0.1821.200.854^^Significant result. To resolve a false positive problem in the multiple testing, Bonferroni correction was performed and the significance level was adjusted to p < 0.0036
Qualitative analysis
Twenty-four participants (21.2%) provided comments in the optional free-text box at the conclusion of the survey; respondents noted administrative burden and “turf wars” with other specialties as factors negatively impacting their satisfaction.
Discussion
This study demonstrated variable professional fulfillment among interventional radiologists. The mean job, career, and specialty satisfaction scores were 3.48, 3.40, and 3.62, respectively. Within these individual component measures, mean job and career satisfaction fell under the reported range of averages across a prior multispecialty study (3.52–3.81 for job satisfaction and 3.55–3.80 for career satisfaction) [18]. Contrastingly, specialty satisfaction amongst interventional radiologists was on par with the highest reported specialties in the prior study (3.17–3.76). Importantly, this study was from 20 years earlier, and significant interim changes in the practice of interventional radiology and clinical medicine may limit direct comparison. However, this divergence suggests that respondents are committed to their chosen field, but they also may experience challenges in the daily realities of practice that take away from their overall feeling of professional fulfillment.
More granular analysis with multivariate analysis revealed that relationships with patients were positively correlated with all three composite aspects of professional fulfillment. While consistent with research in other specialties [19], this is particularly salient within radiology as it may explain fundamental differences in professional fulfillment between diagnostic and interventional radiology. This is also a finding that might distinguish this subspecialty from diagnostic radiology and guide current and future efforts to enhance engagement and satisfaction within similar specialties. Personal time was correlated with both job and career satisfaction, and pay was correlated with career satisfaction. This is consistent not only with prior radiology-based studies [20, 21], but also non-radiologic specialty-specific research [22]. While perhaps unsurprising that work-life balance is a large factor, this bears reflection from practice and societal leadership moving forward. There is existing literature pertaining to work-life balance and wellness that found lower self-reported scores in those categories for IR physicians [23]. Strategies to improve wellness among the specialty might focus on professional role and identity, maintaining supportive workplaces, and providing resources for both physical and emotional well-being, including mentorship, stress management, and peer support.
Further, some qualitative responses to the survey noted administrative burdens and “turf wars” between specialties. This finding, while restricted to only a few survey respondents, suggests a systemic issue external to the individual interventional radiologist. There are several societal and interpersonal approaches to minimizing these types of conflicts, including the “able, affable, and available” mindset to better communicate interprofessionally. Societally, guidelines pertaining to accurate dictation for procedures, quality measurements for patient care, and patient awareness campaigns regarding the role of IR in patient care might be further employed to better address these concerns.
Direct comparison with previous studies of radiologist satisfaction is limited given methodological differences—prior studies’ results constitute a wide range of reported satisfaction scores within the three reported domains [20–22, 24]. However, prior studies have reported low wellness scores amongst practicing interventional radiologists, as well high degrees of moral injury which has been defined as a transgression of individual ethical values at a systemic or institutional level [13]. These two findings, when combined, may account for the discrepancy between the relatively low job and career satisfaction scores and the high specialty satisfaction scores. These findings deserve further investigation, as not only have low job satisfaction scores been correlated with physician burnout amongst radiologists, [25, 26], but overall levels among providers have been increasing in recent years and particularly accelerated by the recent Covid-19 pandemic [11, 12, 27]. These findings carry implications not only for the interventional radiology workforce, but secondarily health system care delivery and patient outcomes.
There are several limitations of this study. First, the survey population may be impacted by selection bias and may not be reflective of the general population of interventional radiologists. Prior work has demonstrated 27% of physicians in IR practice in an academic setting, while the sample here found that number to be 37.7%. Our sample also had 43.4% of IR physicians in a private setting, while that number has been found to be above 50% in the literature [28]. Related to this, the work herein was based in the United States, leaving out potential participants on other continents, such as Europe. Also, the small proportion of interventional radiology trainees in this study limits specific insights into this group. Furthermore, both the survey design and small sample population limited this survey’s ability to provide insight into job satisfaction among different groups. Indeed, some previous studies of job satisfaction among physicians have shown variations by race and gender [20, 29–33], though this has not been consistently demonstrated [21, 34]. Further research is needed to further validate recent trends in interventional radiologist satisfaction, as well as address the limitations above.
Overall, the current study demonstrates that while interventional radiologists may derive professional fulfillment from satisfaction with their specialty choice, their relatively low scores in job and career satisfaction have important implications for the field and healthcare delivery. Given the findings discussed here and the paucity of literature on this topic of professional fulfillment in a rapidly evolving and expanding subspecialty, further research is needed to better describe the specific environmental, institutional, and interpersonal factors that influence satisfaction across career stages, practice models, and demographics. More inclusive studies, building on the findings here, are warranted to explore how gender, race, and training status intersect with professional fulfillment in interventional radiology.
Conclusions
This study provides one of the first targeted assessments of professional fulfillment among interventional radiologists using a validated, specialty-agnostic assessment tool. The findings demonstrate that while approximately half of respondents reported being satisfied with their specialty, minority proportions expressed satisfaction with their current job and career trajectory. Patient interactions and work-life balance were positive effectors of professional fulfillment. The quantitative and qualitative findings here not only guide future research but also highlight actionable areas that can be addressed in the near term, including interventions aimed at adjusting personal time and promoting more patient-centered roles, as well as more systemic change such as minimizing administrative hurdles and clarifying scopes of practice. Addressing the factors discussed herein and how they relate to professional fulfillment is not only critical to workforce well-being but may also yield downstream benefits for patient care and health system performance.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Konrad TR, Williams ES, Linzer M, et al. Measuring physician job satisfaction in a changing workplace and a challenging environment. SGIM Career Satisfaction Study Group. Society of General Internal Medicine. Med Care. Nov 1999;37(11):1174–82.10.1097/00005650-199911000-0001010549620 · doi ↗ · pubmed ↗
- 2Woerner AJ, Greenberg CH, Chick JFB, Monroe EJ, Abad-Santos M, Kim H, Lee E, Makary MS, Hage AN, Covello B, Shin DS. Moral Injury Among Interventional Radiologists. Acad Radiol. 2023 Nov 3:S 1076–6332(23)10.1016/j.acra.2023.09.01537926643 · doi ↗ · pubmed ↗
- 3Koo HJ, Do KH. The Manpower Crisis and Burnout in Academic Radiology: Insights from a Survey Study in Korea. J Am Coll Radiol. 2023.10.1016/j.jacr.2023.08.04637778572 · doi ↗ · pubmed ↗
- 4Glymour MM, Saha S, Bigby J, Group So GIMCSS. Physician race and ethnicity, professional satisfaction, and work-related stress: results from the Physician Worklife Study. J Natl Med Assoc. Oct 2004;96(10):1283–9, 1294.PMC 256851815540879 · pubmed ↗