Lack of physiotherapy resources restricts exercise prescription for patients with chronic kidney disease—the EUropean SUrvey on REnal EXercise (EUSUREX)
Naomi Clyne, Adamasco Cupisti, Clemens Grupp, Evangelia Kouidi, Eva Segura-Ortí, Pasquale Fabio Provenzano, Vicent Esteve-Simó, Giovanni Tripepi, Carmine Zoccali, David Plate, David Plate, Horst Berger, Andreas Fürsch, Thomas Döltz, Norgit Meyer, Cosima Pohle, Dominik Kahle

TL;DR
A European survey found that lack of physiotherapy resources and reimbursement is the main barrier to prescribing exercise for chronic kidney disease patients, despite healthcare professionals recognizing its benefits.
Contribution
This study identifies structural healthcare system limitations as the primary barrier to integrating exercise for CKD patients in Europe.
Findings
Most healthcare professionals believe exercise is beneficial, but only 59% prescribe it regularly.
Only Sweden has adequate physiotherapy resources and reimbursement for CKD patients.
Between 9% and 37% of patients received exercise programs, with only one- to two-thirds continuing to exercise.
Abstract
We hypothesized that the main barriers to integrating exercise in routine care of patients with chronic kidney disease (CKD) were structural within European healthcare systems rather than due to resistance among healthcare professionals or patients. This descriptive cross-sectional study used anonymized questionnaires to investigate nurses’ and physicians’ attitudes and practice towards exercise in patients with CKD, structural support within the healthcare system, and patients’ experience of exercise prescriptions. Kidney units were randomly selected in Germany, Greece, Italy, Spain, and Sweden. In total, 352 (35% male) nurses; 143 (54% male) physicians participated; 96% and 98%, respectively, believed exercise was beneficial. Of them, 59% (CI 50%–67%) prescribed exercise ‘always or often’ (I2 91%), ranging from 15% in Germany to 86% in Sweden. Of the facilities, 48% (CI 39%–56%) did…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
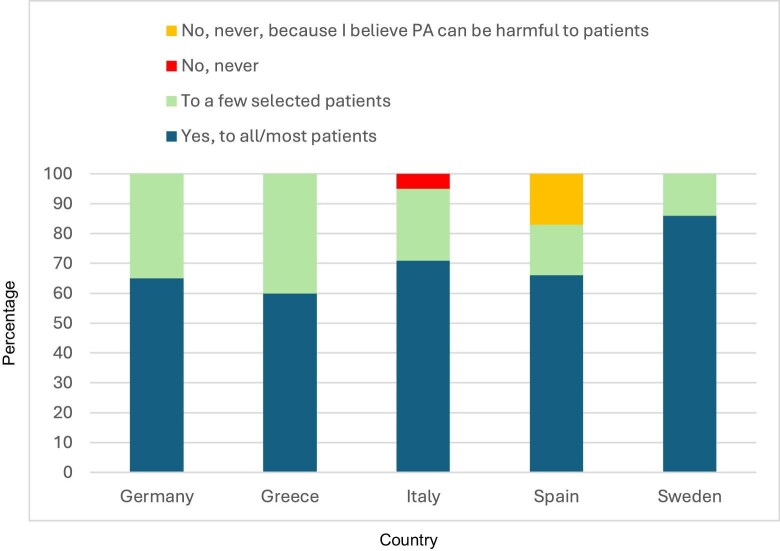 Figure 1
Figure 1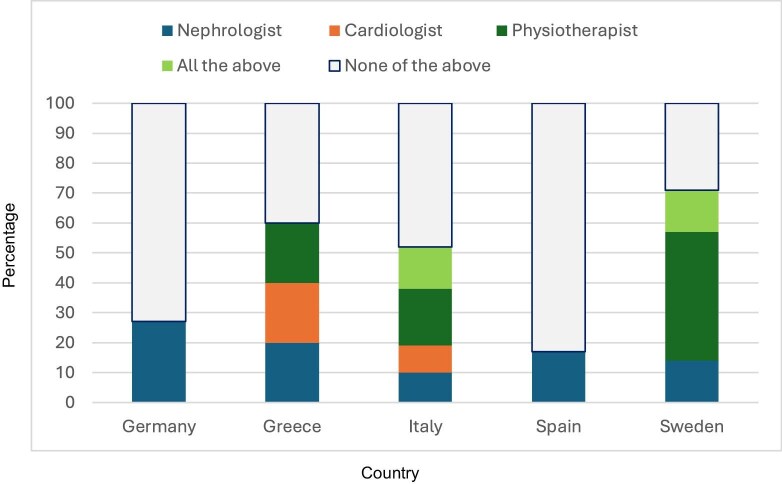 Figure 2
Figure 2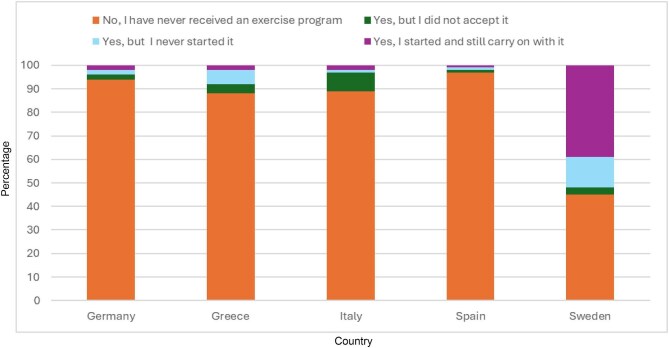 Figure 3
Figure 3| All countries | Germany | Greece | Italy | Spain | Sweden | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Nurses | Physicians | Nurses | Physicians | Nurses | Physicians | Nurses | Physicians | Nurses | Physicians | Nurses | Physicians | |
|
| 352 | 143 | 102 | 44 | 7 | 5 | 198 | 84 | 20 | 6 | 25 | 7 |
| Sex, M/F, % | 35/65 | 54/46 | 11/89 | 59/41 | 0/100 | 60/40 | 56/44 | 48/52 | 20/80 | 33/67 | 0/100 | 57/43 |
| Age years | 45 ± 11 | 46 ± 12 | 43 ± 14 | 51.4 ± 9 | 33 ± 8 | 46 ± 15 | 47 ± 9 | 44 ± 12 | 44 ± 13 | 44 ± 13 | 44 ± 11 | 46 ± 13 |
| Weight kg | 65 [58–75] | 66 [59–80] | 65 [60–75] | 76 [64–84] | 65 [60–70] | 80 [63–95] | 65 [57–75] | 63 [57–75] | 61 [56–72] | 60.5 [54–97] | 64 [56–70] | 73 [63–78] |
| Height cm | 167 ± 10 | 171 ± 9 | 168 ± 8 | 177 ± 9 | 169 ± 7.3 | 173 ± 8 | 167 ± 11 | 169 ± 8 | 165 ± 10 | 172 ± 12 | 164 ± 6 | 175 ± 9 |
| BMI | 24 ± 4 | 24 ± 4 | 24 ± 4 | 24 ± 3 | 23 ± 2.8 | 26 ± 4 | 24 ± 4 | 23 ± 4 | 25 ± 4 | 23 ± 4 | 24 ± 3 | 23 ± 2 |
| Smoker: non-/ex-/current, % | 60/21/19 | 76/10/14 | 79/6/15 | 84/7/5 | 43/14/43 | 0/20/80 | 49/28.8/21.2 | 75/10/15 | 45/30/25 | 67/33/0 | 84/16/0 | 86/0/14 |
| Physical exercise, % | 61 | 58 | 78 | 79 | 57 | 40 | 48 | 45 | 70 | 50 | 92 | 100 |
| Duration, min/week | 180 [120–240] | 120 [90–180] | 152 [100–240] | 120 [90–180] | 80 [65–110] | 105 [90–120] | 180 [120–240] | 120 [90–180] | 140 [120–218] | 180 [90–540] | 240 [180–285] | 200 [142–300] |
| Patients | |||||||
|---|---|---|---|---|---|---|---|
| Nurses | Physicians | CKD 4–5 | PD | HHD | IHD | KT | |
| I engage in regular exercise, % | 61 (55–94) | 58 (50–66) | |||||
| Importance of info to patients on regular exercise, % | 96 (94–98) | 98 (94–100) | |||||
| Importance of exercise as integrated therapy for patients, % | |||||||
| Nurses | 88 (85–89) | 91 (87–94) | 83 (79–87) | NA | 83 (78–87) | 90 (86–93) | |
| Physicians | 93 (91–95) | 94 (89–97) | 95 (90–98) | NA | 89 (83–94) | 94 (89–98) | |
| I have received an exercise programme, % | 14 (8–21) | 37 (22–54) | 14 (4–32) | 11 (7–12) | 33 (24–44) | ||
| Importance of info to patients on nonsmoking, % | 96 (94–98) | 98 (94–99) | |||||
| Importance of info to patients on alcohol consumption, % | 95 (93–97) | 98 (94–99) | |||||
| Importance of info to patients on healthy diet, % | 99 (97–100) | 99 (95–100) | |||||
| Question | Response | All countries, % | Germany, % | Greece, % | Italy, % | Spain, % | Sweden, % |
|
|---|---|---|---|---|---|---|---|---|
| Do you refer to a specialist, or prescribe directly, and remind your patients to engage in exercise? | Always/Often | 59 (50–67) | 15 (6–29) | 40 (5–85) | 78 (68–87) | 66 (22–95) | 86 (42–99) | 91.1 |
| Sometimes | 22 (15–29) | 29 (16–45) | 60 (15–95) | 18 (10–28) | 17 (0.4–64) | 0 | 30.8 | |
| Rarely | 8 (4–14) | 17 (7–32) | 0 | 4 (0.8–10) | 17 (0.4–64) | 14 (0.4–58) | 43.3 | |
| Never | 11 (7–18) | 39 (24–55) | 0 | 0 | 0 | 0 | 91 | |
| Never, I believe exercise is harmful for patients | 0 | 0 | 0 | 0 | 0 | 0 | NA | |
| Do you ask your patients about their level of exercise? | Always/Often | 73 (65–80) | 81 (66–91) | 0 | 71 (60–84) | 67 (22–95) | 43 (9–81) | 24.1 |
| Sometimes | 21 (15–29) | 17 (7–31) | 0 | 25 (16–36) | 33 (4–77) | 57 (18–90) | 12.9 | |
| Rarely | 6 (3–12) | 2 (0.1–13) | 100 (48–100) | 4 (0.8–10) | 0 | 0 | 99.4 | |
| Never | 0 | 0 | 0 | 0 | 0 | 0 | NA | |
| Do you regularly advise your patients to increase their level of exercise? | Yes, to all/most patients | 69 (61–77) | 65 (48–78) | 60 (15–95) | 71 (60–81) | 66 (22–95) | 86 (42–99) | 0 |
| To a few selected patients | 27 (20–35) | 35 (22–52) | 40 (5–85) | 24 (15–35) | 17 (0.4–64) | 14 (0.4–57) | 0 | |
| No, never | 3 (0.8–7) | 0 | 0 | 5 (1–12) | 0 | 0 | NA | |
| No, never, because I believe PA can be harmful to patients | 1 (0.02–4) | 0 | 0 | 0 | 17 (0.4–64) | 0 | NA | |
| Do you consider assessing level of physical performance important? | Yes, in CKD 4–5, no KRT | 26 (22–31) | 25 (17–33) | NA | 28 (22–33) | 34 (13–59) | 24 (9–45) | 0 |
| Yes, HD | 24 (20–28) | 25 (17–33) | 100 (48–100) | 22 (17–27) | 22 (6–47) | 24 (9–45) | 96.1 | |
| Yes, PD | 25 (21–29) | 25 (17–33) | NA | 25 (20–31) | 22 (6–47) | 24 (9–45) | 0 | |
| Yes, KT | 24 (20–28) | 21 (15–30) | NA | 25 (20–31) | 22 (6–47) | 28 (12–49) | 0 | |
| No | 1 (0.4–3) | 4 (1–9) | NA | 0 | 0 | 0 | NA | |
| Do you or an exercise professional objectively assess level of physical performance? | Yes, informally | 41 (32–49) | 10 (3–24) | 60 (48–70) | 33 (4–77) | 20 (0.5–71) | 87.8 | |
| Yes, routinely with questionnaires | 2 (0.5–6) | 5 (0.6–17) | 40 (5–85) | 1 (0.3–6) | 67 (22–95) | 20 (0.5–71) | 0 | |
| Yes, routinely with tests | 2 (0.5–6) | 5 (0.6–17) | 20 (0.5–71) | 1 (0.3–6) | 60 (15–94) | 0 | ||
| Yes, only in selected patients with questionnaires | 3 (0.8–7) | 3 (0.1–13) | 40 (5–85) | 4 (0.8–10) | 0 | |||
| Yes, only in selected patients, with tests | 6 (3–11) | 3 (0.1–13) | 34 (24–45) | 0 | ||||
| No, never | 46 (37–54) | 74 (58–87) | 1 (0.3–6) | 72.1 | ||||
| Which assessments do you consider necessary before enrolling a patient in an exercise programme? | Cardiological evaluation | 42 (35–50) | 53 (39–67) | 40 (5–85) | 41 (32–51) | 14 (0.4–58) | 34.8 | |
| Neurological evaluation | 3 (1–7) | 2 (0.1–10) | 60 (15–95) | 5 (2–11) | 17 (0.4–64) | 43 (10–81) | 0 | |
| Physiotherapeutic evaluation | 26 (19–31) | 23 (13–37) | 27 (19–35) | 83 (36–99) | 29 (4–70) | 0 | ||
| All of the above | 25 (19–31) | 13 (6–26) | 26 (18–34) | 14 (0.4–57) | 90.5 | |||
| None of the above | 4 (1–7) | 9 (3–21) | 1 (0.2–4) | 50.9 | ||||
| Which type of exercise do you consider most suitable for patients on HD? | Intradialytic exercise | 21 (15–26) | 31 (22–41) | 40 (5–85) | 5 (1–12) | 33.3 (4–77) | 27 (6–61) | 77.7 |
| Home-based programmes | 49 (42–56) | 34 (25–44) | 60 (15–94) | 72 (60–80) | 33.3 (4–77) | 55 (23–83) | 84.8 | |
| Assisted in-centre | 28 (21–34) | 35 (27–46) | 21 (13–31) | 33.3 (4–77) | 18 (2–51) | 45.9 | ||
| None of the above | 2 (1–5) | 2 (0.8–8) | 87.8 | |||||
| What is your opinion regarding intradialytic exercise | Risks outweigh benefits | 11 (6–17) | 5 (0.6–16) | 14 (7–23) | 40 (5–85) | 52.4 | ||
| Benefits outweigh risks | 51 (42–59) | 78 (62–89) | 60 (15–94) | 37 (20–57) | 60 (15–94) | 43 (10–82) | 62.9 | |
| Benefits and risks are equal | 14 (8–20) | 10 (3–23) | 40 (5–85) | 15 (8–25) | 14 (0.4–57) | 0 | ||
| No opinion | 24 (17–32) | 7 (2–20) | 34 (24–45) | 43 (10–82) | 86.2 |
| Question | Response | All countries, % | Germany, % | Greece, % | Italy, % | Spain, % | Sweden, % |
|
|---|---|---|---|---|---|---|---|---|
| Is there a physiotherapy unit at your hospital/facility? | Yes, but not with exercise programmes for kidney patients | 41 (33–49) | 70 (58–79) | 14 (0.4–57) | 92.4 | |||
| Yes, it is involved with exercise programmes for kidney patients | 6 (3–12) | 1 (0.03–7) | 86 (42–99) | 97 | ||||
| Yes, for patients with neuro-muscular disease | 5 (2–10) | 8 (4–17) | NA | |||||
| No, there is no physiotherapy unit | 48 (39–56) | 100 (91–100) | 100 (48–100) | 21 (13–31) | 100 (54–100) | 97.8 | ||
| Does your kidney unit have dedicated exercise programmes for patients? | On dialysis | 6.3 (3–12) | 7 (2–20) | 100 (48–100) | 9 (3–17) | 14 (0.4–57) | 97.6 | |
| CKD no KRT | 0.7 (0.02–4) | 2 (0.6–13) | 1 (0.03–7) | 0 | ||||
| KT | 0.7 (0.02–4) | 1 (0.03–7) | NA | |||||
| All the above | 7.7 (4–13) | 5 (1–12) | 97 | |||||
| No, none | 84.6 (78–90) | 91 (77–97) | 84 (75–91) | 100 (54–100) | 86 (42–99) | 0 | ||
| Does your hospital/facility have dedicated staff for prescribing and supervising exercise programmes for kidney patients? | Yes, staff from the Nephrology Dept | 2 (0.4–6) | 3 (0.1–13) | 40 (5–85) | 68.8 | |||
| Yes, physiotherapists | 7 (3–12) | 5 (1–17) | 20 (0.5–71) | 4 (1–10) | 71 (29–96) | 86.8 | ||
| Yes, graduates in exercise science | 3 (1–7) | 2 (0.3–8) | 0 | |||||
| Yes, nurses | 18 (12–26) | 63 (47–78) | NA | |||||
| No, none of the above | 70 (62–78) | 29 (16–45) | 40 (5–85) | 94 (86–97) | 100 (54–100) | 29 (4–71) | 93.7 | |
| Which specialist is primarily responsible at your hospital/facility for prescribing physical exercise outside the dialysis unit for patients on dialysis? | Nephrologist | 16 (10–23) | 27 (15–44) | 20 (0.5–72) | 10 (4–18) | 17 (0.4–64) | 14 (0.4–58) | NC |
| Cardiologist | 6 (3–11) | 20 (0.5–72) | 9 (3–17) | 0 | ||||
| Physiotherapist | 14 (9–21) | 20 (0.5–72) | 19 (11–30) | 43 (10–82) | 0 | |||
| All the above | 9 (5–15) | 14 (7–24) | 14 (0.4–58) | 0 | ||||
| None of the above | 55 (46–64) | 73 (56–85) | 40 (5–85) | 48 (36–59) | 83 (36–99) | 29 (4–71) | 70.3 |
| CKD 4–5 | PD | HHD | IHD | KT | |
|---|---|---|---|---|---|
| Total Number of patients | 137 | 40 | 30 | 928 | 100 |
| Germany | 43 | 13 | 26 | 293 | 25 |
| Greece | 0 | 0 | 0 | 49 | 0 |
| Italy | 27 | 20 | 3 | 411 | 19 |
| Spain | 16 | 0 | 0 | 144 | 2 |
| Sweden | 51 | 7 | 1 | 31 | 54 |
| Sex, M/F, % | 85/52 | 60/40 | 63/37 | 59/41 | 62/38 |
| Age, years | 68 ± 15 | 62 ± 19 | 75 ± 9 | 68 ± 14 | 58 ± 13 |
| Marital status, % | |||||
| Married/cohabiting | 61 | 75 | 57 | 60 | 68 |
| Divorced/separated | 7 | 5 | 3 | 8 | 10 |
| Widowed | 17 | 2 | 20 | 16 | 6 |
| Never married/cohab | 15 | 18 | 20 | 16 | 16 |
| Highest educational level, % | |||||
| None | 5 | 0 | 6.7 | 4 | 2 |
| Elementary school | 42 | 10 | 23.3 | 29 | 22 |
| Incomplete high school | 10 | 13 | 6.7 | 11 | 16 |
| High school | 16 | 28 | 0 | 23 | 30 |
| Vocational training | 15 | 20 | 43.2 | 15 | 10 |
| University degree | 7 | 21 | 6.7 | 12 | 17 |
| Postgrad | 3 | 5 | 6.7 | 3 | 3 |
| Other | 2 | 3 | 6.7 | 3 | 0 |
| Distance to renal unit, km | 12|3–25] | 19[8–31] | 10[3–19.5] | 8 [3–6] | 13[4–30] |
| Travel time to renal unit, min | 25[15–35] | 25[15–40] | 17.5[10–25] | 20 [10–30] | 20[15–35] |
| Mobility, % | |||||
| No walking limitations | 71 | 83 | 50 | 64 | 86 |
| Walk with a cane or human support | 25 | 10 | 37 | 27 | 11 |
| Wheelchair | 4 | 7 | 13 | 8 | 3 |
| Bedridden | 0 | 0 | 0 | 1 | 0 |
| Informal support from family member, % | 75 | 90 | 83 | 83 | 83 |
| Formal care by professional, % | 25 | 49 | 30 | 48 | 14 |
| All countries, % | Germany, % | Greece, % | Italy, % | Spain, % | Sweden, % | ||
|---|---|---|---|---|---|---|---|
| CKD | No, I have never received an exercise programme | 86 | 91 | NA | 96 | 100 | 74 |
| Yes, but I did not accept it | NA | ||||||
| Yes, I never started it | 5 | NA | 12 | ||||
| Yes, I started and I still carry on with it | 9 | 9 | NA | 4 | 14 | ||
| PD | No, I have never received an exercise programme | 63 | 91 | NA | 55 | NA | 43 |
| Yes, but I did not accept it | 16 | 9 | NA | 25 | NA | ||
| Yes, I never started it | 5 | NA | 5 | NA | 14 | ||
| Yes, I started and I still carry on with it | 16 | NA | 15 | NA | 43 | ||
| HHD | No, I have never received an exercise programme | 85.7 | 88 | NA | 100 | NA | NA |
| Yes, but I did not accept it | 3.6 | 4 | NA | NA | NA | ||
| Yes, I never started it | 3.6 | 4 | NA | NA | NA | ||
| Yes, I started and I still carry on with it | 7.1 | 4 | NA | NA | NA | ||
| IHD | No, I have never received an exercise programme | 91 | 94 | 88 | 89 | 97 | 45 |
| Yes, but I did not accept it | 4 | 2 | 4 | 8 | 1 | 3 | |
| Yes, I never started it | 2 | 2 | 6 | 1 | 1 | 13 | |
| Yes, I started and I still carry on with it | 3 | 2 | 2 | 2 | 1 | 39 | |
| KT | No, I have never received an exercise programme | 66.4 | 87 | NA | 32 | 100 | 69 |
| Yes, but I did not accept it | 12.2 | 4 | NA | 58 | |||
| Yes, I never started it | 10.2 | NA | 15 | ||||
| Yes, I started and I still carry on with it | 11.2 | 9 | NA | 10 | 16 |
- —Nephrology Research
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDialysis and Renal Disease Management
INTRODUCTION
Observational studies have shown significant associations between decreased mortality and morbidity and level of physical activity in patients with chronic kidney disease (CKD) [1, 2]. Some large, long-term randomized controlled trials (RCT) have shown that exercise increases physical performance in patients with CKD, including the frail and multimorbid [3–6]. Moreover, lower rates of hospitalization were reported in patients who participated in exercise [4, 6].
Earlier studies have shown that both physicians and nurses believed that patients with CKD are too sick, too tired, or just lack motivation to exercise [7–9]. Interestingly, one study showed that physicians who were physically active themselves were more prone to prescribe exercise compared with sedentary physicians [10]. Recent studies have shown that interest, motivation, and adherence were high both in patients on dialysis and with CKD 3–5 [3–6]. However, an important factor for success is the interest shown by healthcare professionals. Patient adherence requires individualized prescription, regular follow-up, and encouragement [4–6, 11, 12]. Recent surveys have shown a change in the attitude of healthcare professionals towards exercise in which they express belief in the positive effects, while indicating lack of support within the healthcare system [13–15].
Our hypothesis was that the main barriers to an integration of exercise in routine care of patients at all stages of CKD and kidney replacement therapy (KRT) are structural and organizational within the European healthcare systems rather than due to resistance among patients or healthcare professionals.
MATERIALS AND METHODS
This is a descriptive cross-sectional study using anonymized questionnaires to investigate healthcare professionals’ attitudes towards exercise in patients with CKD or on KRT; how healthcare professionals and patients perceive implementation of exercise in practice; the structural support provided by the healthcare system at the kidney unit and national levels in five Western European countries. Countries represented in the European Association of Rehabilitation in Chronic Kidney Disease (EURORECKD) were recruited. Recruitment started in 2019 and ended in 2023. The recruitment period was prolonged due to the COVID-19 pandemic. Of the eight countries invited, Germany, Greece, Italy, Spain, and Sweden participated.
Terminology
The term kidney unit describes kidney care given in hospitals or in freestanding dialysis facilities. The term ‘physiotherapist’ includes exercise physiologists and similar trained exercise professionals. Exercise is a subcategory of physical activity and is planned, structured, and repetitive with the aim of improving physical performance.
Randomization process
To ensure broad geographic coverage while maintaining feasibility, we aimed to include approximately one kidney unit per 4 million inhabitants in each participating country. Using available national registries or listings, a random selection process was conducted (by G.T.) to identify eligible kidney units. Where comprehensive national lists were unavailable—as in Germany—random sampling was performed using geographic stratification by zip code to approximate a representative distribution across regions. The number of selected units per country varied based on population size and logistical considerations. Specifically, two centres were selected and participated in both Greece and Sweden. In Germany, 20 centres were selected to reflect its large population and geographical diversity; of these, 13 agreed to participate. In Italy, 13 units were selected and nine participated. In Spain, 10 were selected and two participated. All physicians, nurses, and patients at the selected kidney units were invited to participate in the study.
Construction and validation of the questionnaires
Five questionnaires were constructed in three steps: first, national experts were involved; second current literature and pre-existing questionnaires were studied; third, questionnaires were constructed targeting organization of and resources for exercise programmes at (i) country level, (ii) kidney unit level, (iii) demographic data of attitudes towards exercise and prescription practices in physicians, (iv) demographic data of attitudes towards exercise in nurses, and (v) demographic data and questions on prescription of exercise in patients.
The questionnaires were validated in two steps: questionnaires 1, 2, and 5 by the national leader using specially constructed validation questions and then by the head of each kidney unit (questionnaire 2), the physicians at the kidney unit (questionnaire 3), and the head nurse(s) (questionnaire 4).
Finally, questionnaires 2–5 were translated into the native language.
Statistics
The data were analysed at CNR-IFC Clinical Epidemiology and Pathophysiology of Renal Diseases and Hypertension Unit for statistical evaluation. Data are expressed as mean and standard deviation, median and interquartile range, or as absolute numbers and percentages, as appropriate. The 95% confidence intervals have been calculated for all key variables. When possible, heterogeneity among countries for the key questions have been calculated by I^2^, which measures heterogeneity by estimating the proportion of variation in prevalence estimates for a given condition that stems from real differences between studies rather than from random chance.
Data analyses were carried out by IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY, USA: IBM Corp. IBM Corp. Released 2020.
Ethics approval
The study was approved by the Ethics Committee: Lund Dnr: 2018/762; Thessaloniki prot. no. 88 880/2018; Tuscany prot. no 19 856; Bavaria BLAEK no. 2020–1034. In Spain, the approval of the principal investigator’s Ethics committee, Sweden, was accepted. The study was registered at ClinicalTrials.gov Identifier NCT03923972. All participants received written and oral information, and gave written consent.
RESULTS
Nurses and physicians
In total, 352 (male 35%) nurses and 143 (male 54%) physicians participated. Both the nurses and physicians had on average a normal BMI, >80% were non- or ex-smokers except for Greek physicians of whom 80% were current smokers. Of the nurses, 61% (CI 55%–94%) were physically active for a median of 180 (120–240) minutes per week as were 58% (CI 50%–66%) of the physicians for a median of 120 (90–180) minutes per week (see Tables 1 and 2).
In all countries, 96% (CI 94%–98%) of the nurses and 98% (CI 94%–100%) of the physicians believed it was important to inform patients about the benefits of regular exercise, the positive effects on health of not smoking, moderate alcohol consumption, and a healthy diet. Nurses and physicians, respectively, reported a high rating of importance regarding integrating exercise in routine treatment for patients with CKD 4–5 (91%; 94%), on peritoneal dialysis (PD) (83%; 67%), on institutional haemodialysis (IHD) (83%; 89%), and with a kidney transplant (KT) (90%; 94%) (see Table 2).
Prescription of exercise in practice by physicians
Of the physicians, 59% (CI 50%–67%) prescribed exercise ‘always or often’ (I^2^ 91%), ranging from 15% (CI 6%–29%) of the German physicians to 86% (CI 42%–99%) of the Swedes. I^2^ shows how much of the variation in results reflects true differences in the underlying prevalence, as opposed to random sampling error within an individual study.
Six% (CI 3%–12%) ‘rarely’ inquired about patients’ level of exercise, ranging from 0% in Sweden to 100% in Greece (I^2^ 99%). Another 69% (CI 61%–77%) regularly advised ‘all or most’ patients to increase their level of exercise (I^2^ 0) (see Fig. 1). However, concerning assessment of patients’ level of physical performance, 24% to 26% of the physicians considered it to be ‘important’ for all treatment modalities (I^2^ 0), in Greece the facility comprised patients on IHD only. In all countries, 41% (CI 32%–49%) informally assessed their patients’ level of physical performance themselves or with a physiotherapist (I^2^ 88%). 25% (CI 19%–31%) believed that patients should have a cardiological, neurological, and physiotherapeutical evaluation before enrolling in an exercise programme, ranging from 13% in Germany to 83% in Spain (I^2^ 90%). 49% (CI 42%–56%) believed home-based exercise was most suitable for patients on IHD (I^2^ 85%) and 21% (CI 15%–26%) intradialytic exercise (I^2^ 78%). Regarding intradialytic exercise 51% (CI 42%–59%) believe that ‘benefits outweigh risks’ (I^2^ 63%), and 24% (CI 17%–32%) had ‘no opinion’ (I^2^ 86%) (see Table 3).
Prevalence by country of the responses to the question ‘Do you regularly advise your patients to increase their level of exercise?’
Healthcare structure’s provision of resources for exercise for kidney patients
Forty-eight% (CI 39%–56%) did not have a physiotherapy unit at their hospital/facility (I^2^ 98%), 41% (CI 33%–49%) had one but not dedicated to kidney patients (I^2^ 92%): in Italy 70% (CI 58%–79%) and Sweden 14% (CI 0.4%–57%) did not (I^2^ 92%). Six% (CI 3%–12%) had a physiotherapy unit for kidney patients: Italy had one% (CI 0.03%–7%) and Sweden had 86% (CI 42%–99%) (I^2^ 97%). Seventy% (CI 62%–78%) did not have dedicated staff for prescribing and supervising exercise programmes for kidney patients (I^2^ 94%), seven% (CI 3%–12%) had physiotherapists: Italy had four% (CI 1%–10%) and Sweden had 71% (CI 29%–96%) (I^2^ 87%). Of all kidney units, 85% (CI 78%–90%) did not have dedicated exercise programmes for any of the treatment modalities (I^2^ 0), six% (CI 3%–12%) had them for patients on dialysis only (I^2^ 98%), and eight% (CI 4%–13%) had them for all treatment modalities (I^2^ 97%). Two countries had dedicated exercise programmes for all treatment modalities: Italy had five% (CI 1%–12%) and Sweden had 86% (CI 42%–99%) (I^2^ 97%). Fifty-five% (CI 46%–64%) did not have a dedicated specialist outside the dialysis unit for prescribing exercise to patients on dialysis (I^2^ 70%, see Fig. 2 and Table 4).
Prevalence by country of the responses to the question ‘Which specialist is primarily responsible at your hospital/facility for prescribing exercise outside the dialysis unit for patients on dialysis?’
Healthcare structure’s reimbursement for costs of physiotherapists
In Germany, health insurance is compulsory, provided either through statutory health insurance or substitutive private health insurance. Compliance with regulations is mandatory, otherwise the prescribing doctor is personally liable for recourse payments. The major barriers in Germany are unclear reimbursement policies for exercise in CKD, along with the considerable risk of personal financial liability for the prescribing physician. On the basis of the results from the DiaTT study, a change of this ruling is currently being discussed [6].
Greece, Italy, and Spain have national healthcare systems. The integration of exercise rehabilitation programmes in CKD management is limited as it is not supported by the national healthcare reimbursement systems. There are no standardized national protocols that formally put exercise interventions and the role of the physiotherapist into chronic disease care pathways, resulting in fragmented implementation and limited referral by physicians.
Sweden has county level healthcare services, which is available to all residents; patients pay a fixed maximum contribution per year for healthcare and treatment by a physiotherapist is included. It is up to each hospital and kidney unit to allot resources to a physiotherapist within the budget provided. The National Board of Social Affairs and Health recommends physical activity for people with chronic diseases and has implemented ‘Physical Activity on Prescription’, which enables healthcare professionals to prescribe subsidized physical activity that is included in the budget for pharmaceuticals. There is also an official pharmacopoeia for prescription of physical activity for most chronic diseases.
Patients
A total of 1235 patients participated from all countries, comprising 137 patients (male 62%) with CKD 4–5, 40 patients (male 60%) on PD, 30 (male 63%) patients on home haemodialysis (HHD), 928 (male 59%) patients on IHD, and 100 (male 62%) patients with KT. The average age ranged from 58 ± 12 years for patients with KT to 75 ± 9 years for patients on HHD. Most patients had no walking limitations (CKD 4–5 71%; PD 83%, HHD 50%, IHD 64%, KT 86%), 75% to 90% reported informal support from a family member, and 14% to 49% had formal care from a professional caregiver (see Table 5).
Patients’ perceptions of prescription of exercise in practice
Of patients with CKD 4–5, 14% reported having received an exercise programme, 37% of patients on PD, 14% on HHD, 11% on IHD and 33% with KT. 9% (CKD), 16% (PD), 7% (HHD), 3% (IHD), and 11% (KT) of all patients in each treatment modality had continued with the exercise programme, constituting a self-reported adherence between 33% and 64%. See Table 6, see Fig. 3 for prevalence in patients on IHD by country.
Prevalence by country of the responses of patients on haemodialysis to the question ‘Have you ever received a rehabilitation/exercise programme from a staff member at your kidney unit?’
DISCUSSION
In this European survey of attitudes towards prescription and implementation of and allocated resources for exercise in patients with CKD 4–5 and on KRT, we found that >95% of the nurses and physicians believed in the benefits of exercise, ∼70% regularly asked patients about their level of exercise and regularly advised them to increase their level of exercise. However, only 25% considered it important to assess patients’ physical performance and <60% prescribed exercise regularly, comprising 15% of the physicians in Germany compared with 78% in Italy and 86% in Sweden. Most patients replied that they had never received an exercise programme, ranging from 63% of patients with PD to 91% on IHD. Of the patients who had received an exercise programme between one- and two-thirds of all patients adhered to it. The patients’ answers reflect the healthcare structure in the respective countries, given that most units did not have physiotherapists who could assess patients’ physical performance, prescribe, and follow progress.
Sweden was the only country with dedicated physiotherapists for patients on IHD and the only country with a reimbursement structure covering the cost of physiotherapists for all stages of CKD and KRT. In no other country studied was reimbursement indisputable for patients with CKD or KRT. In Germany, physicians risk receiving a recourse claim from the health insurance company should they prescribe exercise to patients with CKD or on KRT, for which they are personally liable. In Greece, Italy, and Spain exercise for patients with CKD or on KRT is not reimbursed unless complicated by other comorbidities included in the reimbursement regulations.
There are marked differences in healthcare in the participating countries. Germany has compulsory health insurance; Greece, Italy, and Spain have a national health system; and Sweden has a county health system. The bottom line for each of these systems is that, except for Sweden, there is no reimbursement policy in place to cover the costs of physiotherapists for patients with CKD or on KRT. Moreover, none of the countries, except Sweden, has a national protocol explicitly advocating exercise as an integral part of comprehensive kidney care.
Obviously, the reimbursement system governs what type of healthcare is given, irrespective of the attitudes of the healthcare professionals or patients’ needs and wishes.
This survey found that nurses and physicians strongly believed in the benefits of exercise for all patients irrespective of treatment modality, indicating a profound shift of attitude. Most physicians inquired about their patients’ level of exercise and prescribed exercise. Earlier surveys show that physicians were sceptical of the feasibility of exercise for their patients and were wary of prescribing it as they did not perceive that patients would be interested or have the energy to exercise, nor did they feel convinced of the benefits nor feel confident prescribing exercise [7–9, 16].
During the last decade there have been some important large long-term RCTs in patients on dialysis, unequivocally showing the benefits of exercise on physical performance, hospitalization, and mortality [4, 6], which seem to have affected the attitudes of healthcare professionals, but not reimbursement policies of healthcare providers [7–9].
Few units in this study assessed physical performance or engaged patients in structured exercise. In fact, 85% of all kidney units did not have dedicated exercise programmes for their patients, which is corroborated by most of the patients reporting that they never had received an exercise programme. About 6% of all units had physiotherapists and a physiotherapy unit at their disposal. In Sweden both units studied provided dedicated physiotherapy and leaflets on the benefits of exercise to their patients.
This study showed a marked discrepancy between the importance healthcare professionals attach to exercise and resources allocated. There was also a discrepancy between the strong belief held that exercise is beneficial, which caused physicians to recommend exercise to their patients, and the value attached to assessing each patient’s level of physical performance. Neither the physicians nor the nurses have the training or the time, nor are these tasks part of their job descriptions. Physiotherapists are dedicated professionals trained to assess physical performance and to prescribe exercise programmes to address each person’s weaknesses, physical needs, and goals. Only a very small proportion of patients had the benefit of meeting a physiotherapist.
Several large RCTs with self-administered exercise at home or at a gym have shown that patients on dialysis and with CKD 3–5 have a high rate of adherence over a period of 6 to 12 months [4, 5, 17]. Another large RCT of 12 months’ duration showed that intradialytic exercise was feasible with a high rate of adherence [6]. In these studies, a crucial success factor was regular assessment of physical performance with adjustment of the exercise dose, personal support, and encouragement provided on a regular basis by nurses in the EXCITE trial and by physiotherapists in the RENEXC and DiaTT trials.
Although physicians in this survey are strong advocates of the benefits of exercise for kidney patients, they prescribe or more probably recommend exercise without prior assessment of the patient’s physical performance and without assessing the effects of the therapy. This discrepancy is unsurprising given the lack of physiotherapists to whom patients could be referred. A pharmacological agent would not be prescribed without an assessment of the patient’s baseline status, knowledge of the medication, a definition of the aims hoped to be achieved, and regular follow-up. It is necessary that exercise, a non-pharmacological therapy with evidence-based effects, is managed accordingly.
This European survey clearly shows that the lack of physiotherapeutic expertise and presence at the kidney units is a structural problem within the healthcare systems in the countries studied. In most countries, exercise is not recognized by healthcare providers as an integral part of the care of kidney patients and funding is not provided. These findings are confirmed by recent studies reporting that lack of funding and physiotherapy resources are important barriers [14, 15, 18–20]. Sweden was the exception: both kidney units studied had a dedicated physiotherapist, one unit had a gym adjacent to the dialysis unit and the other unit assessed all patients on KRT biannually and prescribed home- or gym-based exercise. Patients with CKD 4–5 were referred to a physiotherapist in primary care.
This European study substantiates previous findings and highlights the importance of convincing policy makers and healthcare providers of the benefits of exercise in kidney patients. Moreover, it points to a strategy that has shown to be successful in Sweden, with regular assessment and prescription of exercise by dedicated physiotherapists integrated in routine care.
However, if healthcare systems are going to be willing to provide resources, they will want to be convinced that the benefits can be translated into cost reductions. Several trials in patients on dialysis have shown that exercise reduces the number of hospitalizations [4, 6] and other concomitant costs [16]. Several long-term large RCTs in patients with CKD 3–5 and on dialysis have unequivocally shown that all aspects of physical performance improve, which implicitly enhances the patient’s ability to care for themselves and remain mobile making them less dependent on both informal and professional carers [3–6]. To summarize, these benefits translate into less money needing to be spent on in-hospital care and professional caregiving at home or in a care-home.
This study has some limitations. While random selection aimed to reduce selection bias, differential participation rates across countries may have limited full representativeness and introduced some degree of selection bias. Given the pragmatic nature of the study, we did not explore potential for internal bias and heterogeneity of attitudes. The spectrum of views among the healthcare professionals is not fully explored in the current analysis. Future research should investigate these internal differences through in-depth qualitative interviews.
The focus in the present study was healthcare professionals’ attitudes, and the structure of healthcare, patients’ attitudes, and perception of barriers are lacking and will be investigated in a further study. Only Western European countries are represented. Some strengths are the number of healthcare professionals and patients included; that it comprises countries from the north, south, and middle of Western Europe, large and small countries, and countries with different healthcare systems; and that all treatment modalities are included.
In conclusion, healthcare professionals regard exercise as an important element of care in kidney patients, although, they do not assess patients’ physical performance nor provide structured exercise programmes, mainly due to lack of physiotherapy resources and reimbursement strategies within the healthcare system. Sweden is the exception. Thus, it is high time that healthcare systems recognize the beneficial effects of exercise and provide adequate resources. This would improve health and wellbeing for all patients with CKD and on KRT.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mac Kinnon HJ, Wilkinson TJ, Clarke AL et al. The association of physical function and physical activity with all-cause mortality and adverse clinical outcomes in nondialysis chronic kidney disease: a systematic review. Ther Adv Chronic Dis 2018;9:209–26. 10.1177/204062231878557530364521 PMC 6196637 · doi ↗ · pubmed ↗
- 2Tentori F, Elder SJ, Thumma J et al. Physical exercise among participants in the Dialysis Outcomes and Practice Patterns Study (DOPPS): correlates and associated outcomes. Nephrol Dial Transplant 2010;25:3050–62. 10.1093/ndt/gfq 13820392706 · doi ↗ · pubmed ↗
- 3Howden EJ, Coombes JS, Strand H et al. Exercise training in CKD: efficacy, adherence, and safety. Am J Kidney Dis 2015;65:583–91. 10.1053/j.ajkd.2014.09.01725458662 · doi ↗ · pubmed ↗
- 4Manfredini FMF, D’Arrigo G, Baggetta R et al. Exercise in patients on dialysis: a multicenter, randomized clinical trial. J Am Soc Nephrol 2017;28:1259–68. 10.1681/ASN.201603037827909047 PMC 5373448 · doi ↗ · pubmed ↗
- 5Hellberg M, Höglund P, Svensson P et al. Randomized controlled trial of exercise in CKD-the RENEXC study. Kidney Int Rep 2019;4:963–76. 10.1016/j.ekir.2019.04.00131312771 PMC 6609793 · doi ↗ · pubmed ↗
- 6Anding-Rost K, von Gersdorff G, von Korn P et al. Exercise during haemodialysis in patients with chronic kidney failure. NEJM Evidence 2023;2:1–11. 10.1056/EVI Doa 2300057 · doi ↗
- 7Clarke AL, Young HM, Hull KL et al. Motivations and barriers to exercise in chronic kidney disease: a qualitative study. Nephrol Dial Transplant 2015;30:1885–92. 10.1093/ndt/gfv 20826056174 · doi ↗ · pubmed ↗
- 8Moorman D, Suri R, Hiremath S et al. Benefits and barriers to and desired outcomes with exercise in patients with ESKD. Clin J Am Soc Nephrol 2019;14:268–76. 10.2215/CJN.0970081830696660 PMC 6390914 · doi ↗ · pubmed ↗