Rising Above Lumbar Scars: Thoracic Spinal Anesthesia With Hypobaric Bupivacaine for Hip Replacement
Richa Chandra, Kartik Sonawane

TL;DR
Thoracic spinal anesthesia with hypobaric bupivacaine is a safe alternative for hip replacement in patients with prior lumbar spine surgery.
Contribution
Demonstrates the effectiveness of thoracic spinal anesthesia with hypobaric bupivacaine in challenging patients.
Findings
Two geriatric patients with prior lumbar spine surgery successfully underwent hip replacement using TSA.
TSA with hypobaric bupivacaine provided effective anesthesia and smooth recovery.
TSA is a viable alternative when lumbar spinal anesthesia is not feasible.
Abstract
Neuraxial anesthesia is widely practiced for lower limb, abdominal, and pelvic surgeries due to its favorable risk-benefit profile compared with general anesthesia (GA). However, patients with previous lumbar spine surgery and instrumentation present significant challenges for conventional lumbar spinal anesthesia. Altered anatomy, epidural scarring, and the presence of metallic implants often preclude successful needle placement or result in patchy anesthesia. In such patients, GA may be considered, but it carries substantial risks in elderly individuals with significant comorbidities. Thoracic spinal anesthesia (TSA), once regarded with apprehension, has recently re-emerged as a feasible and safe technique, particularly when hypobaric local anesthetics are used to direct drug spread toward the lumbar and pelvic dermatomes. We present two geriatric patients with prior lumbar spine…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
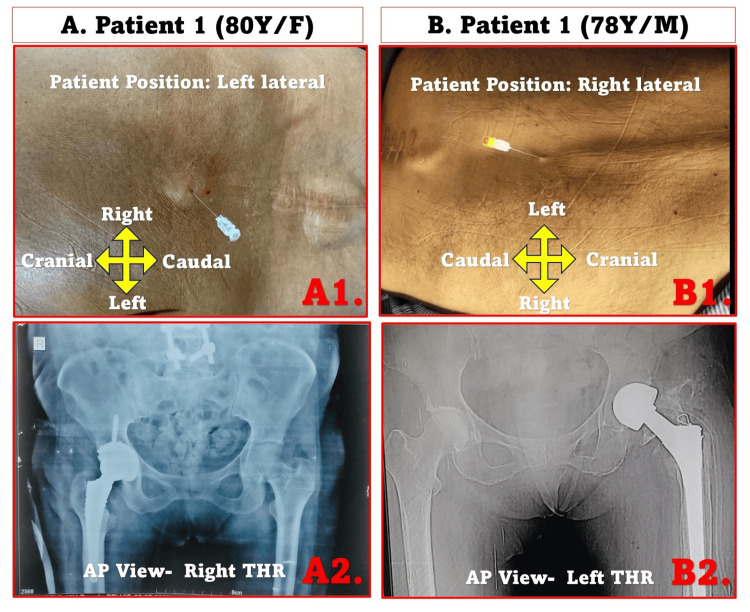 Figure 1
Figure 1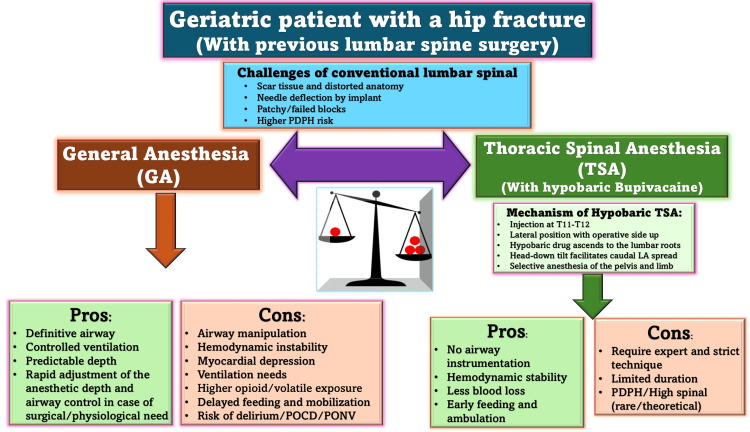 Figure 2
Figure 2| Parameter | Reference Range | Patient 1 (80Y/F) | Patient 2 (78Y/M) |
| Hemoglobin | 11.5 – 15.0 g/dl | 10.2 | 9.8 |
| Total Leukocyte Count | 4,000 – 11,000/cu.mm | 5300 | 6800 |
| Polymorphs (%) | 40 – 75 | 72 | 71 |
| Lymphocytes (%) | 20 – 45 | 25 | 25 |
| Eosinophils (%) | 1 – 6 | 3 | 4 |
| Monocytes (%) | 1 – 8 | 0 | 0 |
| Basophils (%) | 0 – 1 | 0 | 0 |
| Total RBC Count | 4.5 – 6.5 million/cu.mm | 3.8 | 3.5 |
| PCV (HCT) | 36 – 46 % | 32.4 | 31.2 |
| MCV | 80 – 99 fL | 83.1 | 81.9 |
| MCH | 26 – 32 pg | 26.3 | 26.1 |
| MCHC | 32 – 36 g/dl | 31.7 | 31.2 |
| Platelet Count (PLT) | 1.5 – 4.0 lakh/cu.mm | 2.17 | 1.93 |
| Prothrombin Time (PT) | 10 – 14 sec | 13 | 12 |
| Control PT | — | 14 | 14 |
| INR | — | 0.92 | 0.85 |
| Serum Creatinine | 0.4 – 1.4 mg/dl | 1.8 | 1.6 |
| SGOT (AST) | 8 – 40 IU/L | 26.5 | 31.2 |
| SGPT (ALT) | 5 – 40 IU/L | 31.1 | 43.7 |
| Plasma Glucose (Random) | 70 – 140 mg/dl | 162.4 | 172.9 |
| Parameter | Case 1: 80-year-old Female | Case 2: 78-year-old Male |
| History of spinal surgery | Lumbar fracture fixation with pedicle screws in situ | Lumbar discectomy, scar present |
| Orthopedic condition | Right hip fracture, scheduled for THR | Left hip fracture, scheduled for THR |
| Comorbidities | CAD (EF 35%), DM, HTN | COPD, DM, HTN |
| Airway | Mallampati II | Mallampati II |
| Regional block adjunct | Fascia iliaca block (operative side) | Fascia iliaca block (operative side) |
| TSA level | T11–T12 | T11–T12 |
| Intrathecal drug | 0.5% isobaric bupivacaine (1.2 ml) + fentanyl 25 μg (hypobaric) | Same |
| Position | Lateral decubitus, operative side up, slight head-down tilt | Same |
| Epidural catheter | Yes (for rescue/prolonged analgesia) | Yes |
| Intraoperative events | Transient hypotension, managed with mephentermine 6 mg | Transient hypotension, managed with mephentermine 6 mg |
| Surgery duration | ~90 minutes | ~90 minutes |
| Postoperative course | Liquids at 2 h, soft diet at 6 h, early mobilization | Similar, uneventful recovery |
| Feature | Hyperbaric Bupivacaine (Conventional) | Hypobaric Bupivacaine |
| Baricity | >1.0000 (heavier than CSF) | <1.0000 (lighter than CSF) |
| Spread direction | Moves downward (dependent side) | Moves upward (non-dependent side) |
| Patient position for unilateral block | Operative side down (often painful in hip fracture) | Operative side up (comfortable positioning) |
| Predictability of spread | More predictable, dense motor/sensory block | Slightly less predictable, requires careful positioning |
| Hemodynamic impact | More sympathetic blockade, higher risk of hypotension | Less sympathetic blockade, greater stability |
| Block selectivity | Dense bilateral block if the patient supine | More selective unilateral block possible |
| Duration of block | Often longer, may delay mobilization | Typically shorter, allows earlier recovery |
| Clinical limitations | Painful positioning, risk of hypotension | Requires preparation of hypobaric solution |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnesthesia and Pain Management · Nausea and vomiting management · Cardiac, Anesthesia and Surgical Outcomes
Introduction
Neuraxial anesthesia remains a cornerstone in anesthetic practice due to its well-documented advantages over general anesthesia (GA). Avoiding airway manipulation reduces the risks of difficult intubation, aspiration, and postoperative respiratory complications [1]. Furthermore, it maintains spontaneous respiration, blunts sympathetic stress responses, and facilitates earlier oral intake, ambulation, and discharge [1]. These benefits are particularly valuable in elderly and frail patients undergoing orthopedic procedures such as hip replacement [2].
Despite these advantages, the administration of spinal anesthesia becomes increasingly complex in patients who have previously undergone lumbar spine surgery with instrumentation. The presence of scar tissue, distorted landmarks, obliteration of epidural spaces, and metallic implants such as pedicle screws and rods complicate needle placement and drug spread. Even if successful needle placement is achieved, the block may remain inadequate due to intradural and extradural adhesions [3].
Traditional alternatives, including lumbar plexus or combined peripheral nerve blocks, may not provide reliable surgical anesthesia for major hip procedures [4]. GA, although technically straightforward, carries a high perioperative risk in elderly patients with multiple comorbidities such as coronary artery disease (CAD), chronic obstructive pulmonary disease (COPD), and diabetes mellitus (DM). Hemodynamic instability, myocardial depression, postoperative delirium, and delayed mobilization often complicate recovery in this vulnerable group [5].
Historically, thoracic spinal anesthesia (TSA) was approached with apprehension because of concerns about potential spinal cord trauma. However, modern anatomical and magnetic resonance imaging (MRI) studies have demonstrated that the posterior subarachnoid space is wider than previously believed at mid-to-lower thoracic levels, particularly around T5-T12, thereby establishing a safe margin for needle placement when performed with fine-gauge needles and meticulous technique [6]. This evolving anatomical understanding has rekindled interest in TSA as a feasible, safe, and segmental alternative in select clinical scenarios.
In this context, TSA with hypobaric bupivacaine emerges as an attractive and innovative option for patients with prior lumbar instrumentation. By exploiting gravitational spread, hypobaric solutions allow comfortable patient positioning with the operative limb upward, provide selective blockade, and minimize hemodynamic compromise [6, 7]. While TSA has been described in various abdominal and breast surgeries [8, 9], its application at the T11-T12 interspace using a low-dose hypobaric bupivacaine-fentanyl combination with an epidural catheter backup for total hip replacement (THR) in patients with altered lumbar anatomy represents a novel approach.
This case report presents two geriatric patients with prior lumbar spine surgery and multiple comorbidities who successfully underwent THR under hypobaric TSA at T11-T12. It highlights both the safety and the clinical feasibility of this technique in circumstances where conventional neuraxial routes are inaccessible and GA poses a significant risk. Through this report, we aim to expand the clinical applicability of TSA using hypobaric bupivacaine and fentanyl, reinforcing its role as a safe, hemodynamically stable, and patient-centered alternative for high-risk surgical populations.
Case presentation
Case 1
An 80-year-old female presented with a displaced right hip fracture following a fall and was scheduled for THR. She had undergone multiple previous operations on the same hip, including proximal femoral nail fixation twice, followed by removal, and lumbar spine surgery with pedicle-screw instrumentation still in situ. Her comorbidities included CAD with an ejection fraction of 35%, type 2 DM, and hypertension. She appeared frail and undernourished but had no neurological deficits. Airway examination revealed Mallampati class II. Given her poor cardiac reserve and complex spinal history, GA was deemed high risk, while lumbar spinal anesthesia was technically unfeasible.
Case 2
A 78-year-old male presented with a left-sided hip fracture requiring replacement. He had a history of lumbar discectomy, leaving a healed midline scar, but no neurological deficits. His comorbidities included COPD, type 2 DM, and hypertension. He was a former chronic smoker. Upon examination, he was of moderate build, with a Mallampati class II airway. Considering his medical comorbidities and altered lumbar anatomy, a TSA technique was chosen.
Baseline hematological and biochemical profiles of both patients, including mild anemia and borderline renal function with otherwise acceptable perioperative values, are summarized in Table 1.
Procedural overview
All procedures were performed by a single anesthesiologist (the first author, RC), who has extensive experience in TSA. Both patients were placed in the lateral decubitus position with the operative side up. The clinical and radiological images are shown in Figure 1. Operative records and clinical photographs reveal a healed midline lumbar surgical scar in both patients. In Patient 1, the outline of pedicle-screw instrumentation is clearly visible beneath the scar (Figure 1A1), which is also corroborated by the postoperative radiograph showing spinal implants (Figure 1A2). Patient 2 had previously undergone a non-instrumented discectomy, with a visible midline scar but no spinal hardware on the radiograph (Figure 1B1-1B2). The interspace selected for TSA corresponded to the first clearly palpable, non-scarred thoracic level above the surgical site (T11-T12), chosen to avoid fibrosis or hardware interference while ensuring segmental coverage appropriate for hip arthroplasty (approximately T12-S4).
Clinical and radiological findings of two geriatric patients undergoing thoracic spinal anesthesia for total hip replacement.(A1) Spinal puncture performed above the lumbar scar in an 80-year-old female, left lateral position. (A2) Anteroposterior (AP) pelvic radiograph showing right total hip replacement (THR). (B1) Spinal puncture in a 78-year-old male, right lateral position. (B2) AP pelvic radiograph showing left THR.AP: anteroposterior; THR: total hip replacement.
Thoracic spinal puncture was performed at the T11-T12 interspace, above the lumbar scar, using a 25-gauge Quincke spinal needle (Becton Dickinson, USA) under full aseptic precautions (Figure 1A1-B1). The interspace was identified using surface anatomical landmarks, including the twelfth rib and spinous processes. Neither ultrasound nor fluoroscopic assistance was employed, as the surface anatomy was well defined and preoperative imaging had already delineated the surgical hardware and scar extent. Free flow of clear CSF was obtained before injection, confirming correct intrathecal placement. A total of 1.2 mL of 0.5% isobaric bupivacaine was mixed with 25 µg fentanyl immediately before administration to prepare the injectate. The solution was injected slowly over 10-15 seconds after confirming continuous CSF flow. An epidural catheter was introduced at the same level for potential supplementation and postoperative analgesia.
Patients were kept in the lateral decubitus position with a slight head-down tilt to achieve adequate segmental spread and administered supplemental oxygen (4-6 L/min). Sensory blockade was assessed bilaterally using cold and pinprick discrimination at two-minute intervals. Adequate surgical anesthesia (T8-L2 dermatomes) was achieved within six minutes of injection. Motor blockade was graded using the modified Bromage scale, achieving Grade 2 on the operative limb by 12 minutes. The block remained stable throughout the 90-minute procedure and regressed fully within two hours. Intravenous fentanyl (50 µg) and midazolam (1 mg) were given for anxiolysis. Transient hypotension (MAP 68-72 mmHg) occurred in both patients, corrected promptly with a single 6 mg bolus of mephentermine. Heart rate remained 60-85 bpm, and oxygen saturation >98%. Neither patient experienced bradycardia, desaturation, respiratory discomfort, or postoperative nausea and vomiting. Arterial blood gas (ABG) values were within normal limits (PaO₂ 110-125 mmHg, PaCO₂ 36-38 mmHg). Both patients underwent non-cemented THR (Figure 1 A2, B2), with surgeries completed within 90 minutes. Intraoperatively, each received approximately 400 ml of plasmalyte solution and one unit of packed red blood cells.
Postoperatively, they were managed in a high-dependency unit, with epidural catheters providing effective analgesia. Neurological examinations were performed at 2-, 6-, and 24-hours post-procedure, confirming complete motor and sensory recovery. Neither patient experienced post-dural puncture headache (PDPH), urinary retention, or new neurological deficits. Oral liquids were tolerated after 2 hours, followed by a soft diet at 6 hours. Early mobilization was initiated per protocol, and both patients were discharged on postoperative day 4. Both patients were followed up daily until discharge and reassessed one month later. No delayed neurological symptoms, hemodynamic instability, or wound-related complications were noted, confirming the safety and stability of the thoracic spinal approach in this subgroup.
The perioperative details of both cases are summarized in Table 2. Both patients and their relatives were thoroughly counseled regarding the anesthetic technique, its potential benefits and risks, and informed consent was obtained for the procedure and for publication, while ensuring anonymity.
Discussion
Patients with previous lumbar spine surgery present one of the most challenging scenarios for anesthesiologists planning neuraxial anesthesia. While spinal and epidural techniques remain the cornerstone of regional anesthesia (RA), their success depends heavily on the presence of normal anatomical landmarks and intact epidural or subarachnoid spaces. Alterations caused by scarring, adhesions, and instrumentation frequently render conventional lumbar approaches unreliable or even impossible. In such circumstances, alternative regional strategies must be considered, with TSA emerging as a promising option.
Challenges of neuraxial anesthesia after lumbar surgery
Spinal and epidural anesthesia are well-established, safe, effective, and operator-friendly approaches that require relatively simple equipment compared to GA. However, in patients with prior lumbar spine surgery, the administration of neuraxial anesthesia becomes complex and sometimes controversial. Scar tissue from previous laminectomies or fusions may distort spinal anatomy, obliterate tissue planes, and hinder needle advancement. It affects both extradural and intradural areas. Extradural adhesions can restrict needle passage or deflect the trajectory, while intradural adhesions alter CSF dynamics and the spread of local anesthetics (LA). Together, these changes increase the risk of technical difficulty, failed insertion, and patchy or incomplete blocks [3]. Sun (1994) emphasized the risk of incomplete sensory blockade in such patients [3]. Metallic instrumentation, such as pedicle screws and rods, adds further complexity by obscuring anatomical landmarks, blocking access to the subarachnoid space, and potentially increasing the theoretical risks of infection spread [3]. Zhu et al. reported the use of ultrasound to facilitate neuraxial access in parturients with prior spine surgery, but this approach requires available unscarred interspaces, which were absent in our patients [10]. An alternative in such patients is to perform GA. However, this option carries significant drawbacks in elderly patients with major comorbidities.
Limitations of general anesthesia (GA) in high-risk patients
GA remains an option when neuraxial techniques fail, but in elderly patients with significant comorbidities, it carries notable risks. Our first patient had ischemic cardiomyopathy with a left ventricular ejection fraction of 35%, while the second had COPD. Both were at risk of perioperative complications such as myocardial depression, arrhythmias, pulmonary compromise, prolonged ventilation, and delayed mobilization. In this context, avoiding airway instrumentation and reducing systemic anesthetic exposure becomes a critical advantage of RA. Radiological evidence of hip prostheses and prior lumbar instrumentation complicated conventional neuraxial access, leading to the choice of TSA. As illustrated in Figure 2, anesthetic management in geriatric patients with prior lumbar spine surgery requires careful balancing between the risks of GA and the advantages of TSA with hypobaric bupivacaine. However, both GA and TSA can be appropriate, depending on anatomical feasibility and the patient’s profile.
Clinical decision-making in a geriatric patient with a hip fracture and prior lumbar spine surgery.A schematic comparison between general anesthesia (GA) and thoracic spinal anesthesia (TSA) using hypobaric bupivacaine. The diagram highlights the challenges of conventional lumbar spinal approaches in previously operated spines and summarizes the relative advantages and limitations of both techniques. While GA offers airway control and predictable depth, it carries relatively higher risks of hemodynamic instability and delayed recovery in frail patients. TSA, performed at the T11–T12 level using a hypobaric solution, provides segmental anesthesia with better hemodynamic stability and early recovery but requires expertise and has a limited duration.GA: general anesthesia; TSA: thoracic spinal anesthesia; LA: local anesthetic; PDPH: post-dural puncture headache; POCD: postoperative cognitive dysfunction; PONV: postoperative nausea and vomiting.Source: This figure was created by the second author, KS.
Re-emergence of thoracic spinal anesthesia (TSA)
TSA was first introduced by Jonnesco in 1909 but was abandoned for decades due to fears of cord trauma [11]. Modern imaging studies have challenged these concerns. Lee and colleagues demonstrated, through MRI, that the posterior subarachnoid space is wider than previously assumed, with favorable margins at T5 and T10 [12]. Similar studies in Indian populations confirmed these as safe thoracic levels [13]. These findings challenge the dogma of prohibitive risk and reestablish TSA as a feasible option when performed with fine needles and meticulous technique.
Clinical experiences further reinforced the safety and feasibility of TSA. Chandra et al. (2023) reported excellent outcomes in more than 2100 laparoscopic cholecystectomies performed under TSA, while Vincenzi et al. (2023) successfully employed hypobaric TSA for breast surgery [14-15]. Together, these data support TSA as a viable option when conventional lumbar routes are unavailable.
Baricity and its clinical implications
The LA baricity plays a decisive role in TSA spread. Hyperbaric solutions, being denser than CSF, descend under gravity, producing dense blocks on the dependent side [7]. While effective for unilateral surgery, this technique requires positioning the operative side down, a maneuver that is painful and often impractical in patients with hip fractures. Moreover, hyperbaric anesthesia may extend more cephalad, leading to excessive sympathetic blockade and hypotension in frail patients.
Hypobaric solutions, being lighter than CSF, ascend toward the non-dependent side, allowing patients to lie with the injured limb upward- a more comfortable and less distressing position [6]. This approach provides selective blockade of the operative limb, minimizes sympathetic spread, and thereby reduces hypotension [16]. Imbelloni (2014) highlighted that hypobaric agents achieve selective hemianesthesia with fewer hemodynamic consequences [17]. Paliwal et al. described hypobaric spinal anesthesia as “target-specific,” reporting excellent stability in lower limb fractures [18]. Errando et al. (2014) validated its use in elderly patients with hip fractures, showing dose-dependent efficacy while maintaining safety [16]. The key differences between hyperbaric and hypobaric bupivacaine, particularly in the context of TSA for hip surgery, are summarized in Table 3.
Commercial hypobaric formulations are seldom available; therefore, clinicians often rely on practical modifications to achieve relative hypobaricity. This can be accomplished by diluting isobaric bupivacaine with low-density additives such as fentanyl or sterile water rather than warming the solution. Fentanyl, with a baricity of approximately 0.9996 relative to CSF, effectively lowers the overall density of bupivacaine, producing a mildly hypobaric mixture [6]. This simple adjustment has been described in the literature as a reproducible and safe method for achieving selective cephalad spread in lateral decubitus positioning, without the need for specialized equipment or commercial formulations. This method was applied to our patients, offering a simple yet effective solution that did not require specialized equipment.
Alternatives and limitations of other regional techniques
RA for hip surgery can be achieved through lumbar spinal, epidural, combined spinal-epidural, or deep plexus blocks. However, lumbar neuraxial routes may become unreliable or unsafe after spine surgery, and plexus blocks, though valuable, are technically demanding and not always effective as sole anesthetic techniques. Lumbar plexus blocks and related peripheral techniques have been proposed for hip surgery in patients with difficult spines. However, these blocks are technically demanding, lie deep within the psoas compartment, and carry risks of vascular or renal injury [19]. Even under ultrasound guidance, visualization is challenging, and success rates vary widely. Samra et al. (2024) observed that novice anesthesiologists achieved lower success rates with plexus blocks compared to epidural approaches in trauma settings [20]. For major hip replacement procedures, these limitations make plexus blocks less reliable as sole anesthetic techniques. TSA provides a segmental subarachnoid block above the altered lumbar region, avoiding airway manipulation and bypassing scarred spaces. Importantly, our intent is not to claim superiority of TSA over GA or other RA modalities but to highlight its practicality in selected cases where lumbar access is not feasible and general anesthesia carries increased systemic risk.
Clinical outcomes in our patients
In both cases, hypobaric TSA provided excellent surgical conditions, minimal hemodynamic compromise, and a smooth recovery. Only transient hypotension was observed, easily corrected with small doses of mephentermine. The addition of an epidural catheter provided flexibility for rescue anesthesia and effective postoperative analgesia. Both patients tolerated early oral intake, resumed diet within six hours, and mobilized early with physiotherapy. These outcomes demonstrate the tangible benefits of TSA in enhancing recovery and reducing morbidity.
Choice of interspace (T11-T12)
The puncture level at T11-T12 was selected as the first clearly palpable and non-scarred thoracic interspace above the lumbar surgical scar, thereby avoiding dense fibrotic planes or instrumentation that could compromise safety or needle trajectory. This level also ensures segmental coverage of the T12-S4 dermatomes, encompassing the iliohypogastric, femoral, obturator, and sciatic components required for THR. By administering a mildly hypobaric intrathecal mixture in the lateral decubitus position, cephalad spread to T12-L1 and caudal migration to the sacral roots were achieved, providing selective anesthesia of the operative limb with limited sympathetic involvement.
Broader implications
The growing body of literature, including contributions by Chandra, Vincenzi, Imbelloni, Errando, and Paliwal, supports the broader use of TSA with hypobaric solutions in selected patients. Concerns about cord injury remain valid but can be mitigated through careful patient selection, the use of fine-gauge needles, strict adherence to positioning principles, and judicious dosing.
Beyond its immediate application in patients with altered lumbar anatomy, TSA holds promise for several high-risk surgical populations. Studies have demonstrated its feasibility in laparoscopic cholecystectomy, breast surgery, and urological and lower abdominal procedures. These findings suggest that, when performed with appropriate dosing and vigilant monitoring, TSA can achieve segmental, stable, and targeted anesthesia while minimizing airway manipulation and hemodynamic fluctuations. Its use in geriatric and cardiac-compromised patients, where GA carries disproportionate risks, represents an expanding frontier in RA.
In routine practice, hyperbaric bupivacaine remains the most widely used due to its predictability and availability. However, in geriatric patients with hip fractures and altered lumbar anatomy, hypobaric TSA provides a position-friendly, hemodynamically stable, and target-specific alternative that can expand the boundaries of RA.
Advantages and limitations
Our cases highlight several advantages of TSA with hypobaric bupivacaine. The technique allowed comfortable positioning with the operative side up, avoiding the pain associated with dependent positioning required for hyperbaric anesthesia. Hemodynamic stability was maintained, with only transient hypotension requiring minimal vasopressor support. The addition of an epidural catheter provided flexibility for rescue anesthesia and effective postoperative analgesia. These features, combined with rapid recovery and early mobilization, underscore the clinical utility of hypobaric TSA in elderly patients with altered lumbar anatomy.
However, important limitations must be acknowledged. This report describes only two cases, limiting the generalizability of the findings. Hypobaric formulations are not commercially available and require manual preparation, which may introduce variability. Although no neurological or respiratory complications were observed, TSA carries theoretical risks of cord trauma and high spinal block if performed without meticulous technique. Finally, although the outcomes were favorable in our patients, larger prospective studies are needed to establish standardized dosing regimens, assess long-term safety, and determine the broader applicability of this technique.
Conclusions
These cases illustrate that TSA using a mildly hypobaric mixture of bupivacaine and fentanyl can be a safe and feasible anesthetic option in carefully selected patients with previous lumbar spine surgery, where conventional neuraxial access is technically unfeasible and GA poses an elevated risk. The success of this technique depends on experienced practitioners, meticulous patient positioning, and adherence to strict procedural safety principles. While both cases demonstrated favorable outcomes without neurological or hemodynamic complications, these findings should be interpreted as exploratory observations rather than definitive proof of safety or efficacy. Larger prospective studies with detailed procedural and follow-up data are warranted to establish standardized protocols and confirm long-term safety.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Spinal Anesthesia. [Updated 2022 Jun 27] Olawin AM Das JM Treasure Island, FL Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 537299/30725984 · pubmed ↗
- 2Neuraxial versus general anesthesia in elderly patients undergoing hip fracture surgery and the incidence of postoperative delirium: A systematic review and stratified meta-analysis BMC Anesthesiol Cheung KY Yang TX Chong DY So EH 2502320233748151710.1186/s 12871-023-02196-9PMC 10362612 · doi ↗ · pubmed ↗
- 3Spinal anaesthesia following previous spinal surgery Eur J Anaesthesiol Sun KO 321323111994 https://pubmed.ncbi.nlm.nih.gov/7925338/7925338 · pubmed ↗
- 4Lumbar Plexus Block. [Updated 2023 Jan 29] Polania Gutierrez JJ Ben-David B Treasure Island, FL Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 556116/32310576 · pubmed ↗
- 5Retrospective study of anesthesia-related complications in elderly patients undergoing surgery J Pharm Bioallied Sci Yadav S Jahagirdar A Jamwal P Mishra J Thind GB Shashank C Tiwari R 0516202410.4103/jpbs.jpbs_253_24PMC 1142662939346201 · doi ↗ · pubmed ↗
- 6A comparison of thoracic spinal anesthesia with low-dose isobaric and low-dose hyperbaric bupivacaine for orthopedic surgery: A randomized controlled trial Anesth Essays Res Imbelloni LE Gouveia MA 26318201410.4103/0259-1162.128900 PMC 417359425886099 · doi ↗ · pubmed ↗
- 7Does the baricity of bupivacaine influence intrathecal spread in the prolonged sitting position before elective cesarean delivery? A prospective randomized controlled study Anesth Analg Loubert C Hallworth S Fernando R Columb M Patel N Sarang K Sodhi V 81181711320112189088710.1213/ANE.0b 013e 3182288 bf 2 · doi ↗ · pubmed ↗
- 8Thoracic spinal anesthesia is safe for patients undergoing abdominal cancer surgery Anesth Essays Res Ellakany MH 2232288201410.4103/0259-1162.134516 PMC 417360725886230 · doi ↗ · pubmed ↗