Learning Together: A Mixed Methods Study of Interprofessional Mental Health Simulation in Undergraduate Medical and Nursing Training
Thomas Davies, Sung Yeon Kwak, Laura Sevenoaks, Shreiya Narayanan, Chris Jacobs

TL;DR
This study shows that mental health simulations improve confidence and collaboration among medical and nursing students.
Contribution
The study introduces a mixed-methods approach to evaluate interprofessional mental health simulation in undergraduate training.
Findings
Students showed significant confidence improvements after the simulation.
Themes included collaboration, role understanding, and communication.
IPSL enhanced understanding of managing mental health crises.
Abstract
Introduction:Interprofessional education (IPE) involves learners from two or more health professions creating a collaborative learning environment. With the growing use of simulation in medical education, interprofessional simulated learning (IPSL) has had increasing focus on its role in interdisciplinary collaboration, especially in the undergraduate setting. Methods: This mixed methods study was conducted across two universities in South West England, incorporating Year 5 medical students and Year 3 nursing students. The IPSL experience was designed as three different simulation scenarios focusing on the assessment and management of mental health (MH) patients, with an emphasis on interprofessional collaboration. Study participants were asked to complete pre-session and post-session questionnaires with Likert scale and free-text questions used to collect the quantitative and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
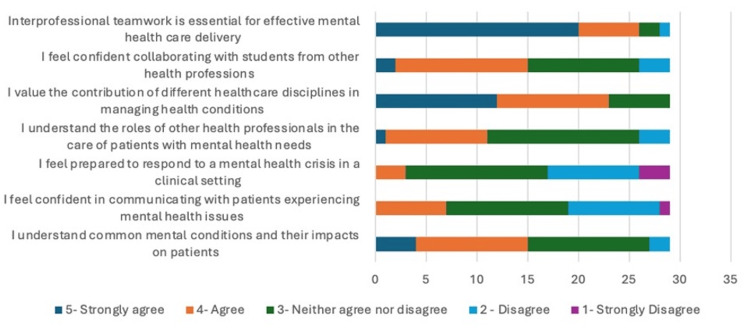 Figure 1
Figure 1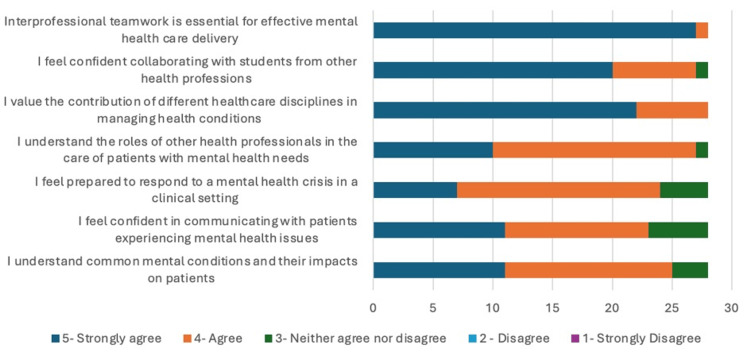 Figure 2
Figure 2| Item | n | Median (Pre) | Median (Post) | Median change | Effect size (r) | p |
| I understand common mental conditions and their impacts on patients | 28 | 3.5 | 4.0 | 0.5 | 0.62 | 0.001 |
| I feel confident in communicating with patients experiencing mental health issues | 28 | 3.0 | 4.0 | 1.0 | 0.75 | <0.001 |
| I feel prepared to respond to a mental health crisis in a clinical setting | 28 | 3.0 | 4.0 | 1.0 | 0.83 | <0.001 |
| I understand the roles of other health professionals in the care of patients with mental health needs | 28 | 3.0 | 4.0 | 1.0 | 0.73 | <0.001 |
| I value the contribution of different healthcare disciplines in managing health conditions | 28 | 4.0 | 5.0 | 1.0 | 0.61 | 0.001 |
| I feel confident collaborating with students from other health professions | 28 | 3.5 | 5.0 | 1.5 | 0.78 | <0.001 |
| Interprofessional teamwork is essential for effective mental healthcare delivery | 28 | 5.0 | 5.0 | 0.0 | 0.47 | 0.013 |
| Item | Beta programme | 95% CI (programme) | p_programme | Beta year | 95% CI (year) | p_year |
| I understand common mental conditions and their impacts on patients | -9.38 | -14.69 to -4.08 | 0.001 | 2.86 | 2.14 to 3.59 | <0.001 |
| I feel confident in communicating with patients experiencing mental health issues | -12.15 | -17.19 to -7.11 | <0.001 | 2.65 | 1.96 to 3.34 | <0.001 |
| I feel prepared to respond to a mental health crisis in a clinical setting | -9.45 | -14.55 to -4.35 | <0.001 | 2.86 | 2.16 to 3.56 | <0.001 |
| I understand the roles of other health professionals in the care of patients with mental health needs | -5.0 | -10.16 to 0.16 | 0.057 | 3.2 | 2.49 to 3.91 | <0.001 |
| I value the contribution of different healthcare disciplines in managing health conditions | -4.06 | -8.27 to 0.16 | 0.059 | 3.27 | 2.69 to 3.85 | <0.001 |
| I feel confident collaborating with students from other health professions | -6.82 | -11.59 to -2.06 | 0.007 | 3.06 | 2.41 to 3.71 | <0.001 |
| Interprofessional teamwork is essential for effective mental healthcare delivery | -5.54 | -7.47 to -3.61 | <0.001 | 3.16 | 2.89 to 3.42 | <0.001 |
| Theme | Quotation number | Quotation | Participant |
| Working collaboratively | 1 | “Understanding more about how to work with doctors ” | P9 |
| 2 | “Collaboration between the team” | P23 | |
| 3 | “Having a chance to work as an MDT with the Drs” | P26 | |
| 4 | “Importance of collaboration” | P5 | |
| Understanding professional roles and skill sets | 5 | “More aware of others roles” | P4 |
| 6 | “Learning what nurses roles are” | P5 | |
| 7 | “Different skill set of the nursing students” | P11 | |
| 8 | “Understanding different roles in varying situations” | P16 | |
| Confidence in managing mental health patients | 9 | “Understanding how to look after patients with MH issues” | P9 |
| 10 | “How to deal with common MH issues” | P7 | |
| Improving communication | 11 | “The importance of clear communication” | P13 |
| 12 | “Learning to be more confident in asking difficult questions” | P1 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSimulation-Based Education in Healthcare · Interprofessional Education and Collaboration · Innovations in Medical Education
Introduction
Interprofessional education (IPE) involves learners from two or more health professions creating a collaborative learning environment [1]. This method of learning is thought to facilitate the preparation of students to provide patient care in a collaborative environment [2]. The benefit of IPE not only lies in the exploration of team roles and attitudes but also in collaborative teamwork and improving communication between professionals [3]. The increasingly complex health needs of patients, requiring input from multiple disciplines and specialities, have highlighted the importance of IPE in healthcare curricula [4]. An increasingly prevalent method of IPE includes interprofessional simulated learning (IPSL) [5] to allow simulated experiences to facilitate student reflection on collaborative practice between different professionals [6].
Simulation is an educational technique where scenarios are designed to recreate events that occur in clinical practice [7]. It creates an environment where students can safely make mistakes and learn from them [8]. Simulation-based education has moved away from the traditional apprenticeship style of healthcare education and draws on constructivist learning theory. Constructivism is the idea that learners construct their own knowledge often through authentic tasks [9]. Simulation is being increasingly used within healthcare education [10] and has been associated with improved patient outcomes [11].
Not only has simulation-based education shown to improve communication and team working skills but also attitudes towards people with mental health [12]. Despite the discussed benefits of IPSL, much of this education is delivered in postgraduate education [13], and research has suggested that more exposure to IPSL should be provided in undergraduate medical education due to its positive impact on inter-disciplinary collaboration [14]. Our study aims to evaluate the impact of a mental health themed IPSL experience for medical, nursing, and allied health professional students. Our study focused not only on the clinical aspects of the simulation but also on the students’ attitudes towards interprofessional learning and collaboration between disciplines.
Materials and methods
Study design and participants
This mixed methods exploratory design study was conducted across two universities in South West England and incorporated fifth-year medical students and third-year nursing students. This quality improvement study was done in accordance with the UK Health Research Authority (HRA) guidelines. The HRA research criteria determine this study as a service evaluation; therefore, the NHS Research Ethics Committee (REC) was not required. All data collected was stored securely and anonymously.
Intervention
The IPSL experience was designed as three different simulation scenarios focusing on the assessment and management of mental health patients, with an emphasis on interprofessional collaboration. The simulations were created by a group of medical education specialists with nursing and medical backgrounds with the aid of a mental health expert. The simulations ran for 20 minutes and were followed by a 40-minute debrief co-led by a member of nursing faculty and a member of the medical faculty. The simulations covered the topics of eating disorder with electrolyte imbalance, self-harm, and elder abuse. Appendix 1 includes the scenarios used in this learning experience.
Data collection
Study participants were asked to complete a pre-session and post-session questionnaires with Likert scale and free-text questions used to collect the quantitative and qualitative data. The questionnaires were designed by the researchers and peer-reviewed by other medical doctors within the medical education field, and formal validation was not completed. The questionnaire allowed students to record their confidence in the underpinning clinical content of the simulation, as well as their understanding and views of the multidisciplinary team and their confidence working within them. Post-session questionnaires contained the same Likert scales, and qualitative feedback was collected about how valuable students found the session and how the interprofessional aspect affected their learning experience. The questionnaires used are included in Appendix 2.
Data analysis
Thematic analysis was conducted on the qualitative data using the six-step data analysis process of Clarke and Braun [15] to manually generate codes and themes (LS). This process was repeated by another researcher (TD). The researchers were both clinicians working in the field of medical education; therefore, it is important to highlight that the analysis would have been completed with this specific lens. The process involved familiarisation with the data, generation of initial codes, and searching and reviewing themes. The emerging themes were collaboratively generated through an iterative process. Disagreements were resolved through discussion until a consensus was reached (TD, LS). No formal analysis software was used.
Descriptive statistics were calculated using medians and interquartile ranges (IQR) for Likert-scale responses, as these ordinal data do not meet normality assumptions. The Wilcoxon signed-rank test was used to evaluate pre-post changes, appropriate for paired ordinal data with small sample sizes. Statistical significance was set at p<0.05. Effect sizes with values of 0.1, 0.3, and 0.5 indicating small, medium, and large effects were used. Subgroup comparisons between nursing and medical students were performed using Mann-Whitney U tests, although interpretation was limited by unequal group sizes.
Results
Quantitative data analysis
Twenty-nine final-year healthcare students (19 nursing, 10 medical) from two universities participated in a single-day mental health interprofessional learning (IPL) simulation. Complete paired pre-post data were collected from 28 participants (96.6% response rate), with one loss to follow-up. A summary of all the pre- and post-questionnaire findings is highlighted in Appendix 3. An infographic of these findings can be seen in Figures 1, 2.
Pre-Session Questionnaire Summary in Likert Scales
Post-Session Questionnaire Summary in Likert Scales
In the pre-session questionnaire, 20 students (71.4%) strongly agreed that interprofessional team is essential for effective mental healthcare delivery. Following the session, this increased to 27 (96.4%). Prior to the session, 12 students (42.8%) strongly agreed with the statement "I value the contribution of different healthcare disciplines in managing mental health conditions," this increased to 22 students (78.6%) following the simulation.
Our results showed seven students (25%) agreed or strongly agreed that they felt confident collaborating with students from other health professions pre-session, this increased to 23 students (82.1%) post-session. There was also an increase seen in the number of students who agreed or strongly agreed with the statement "I understand the roles of other health professionals in the care of patients with mental health needs" from 11 (39.2%) to 27 (96.4%).
There was also a notable improvement in the student’s confidence with managing mental health crisis following the simulation. Only three students (10.7%) agreed or strongly agreed with the statement "I feel prepared to respond to a mental health crisis in a clinical setting prior to the simulation." When comparing this to the post-session feedback, 24 (85.7%) agreed or strongly agreed. Our results demonstrated an increase from seven students (25%) who agreed or strongly agreed with the statement "I feel confident in communicating with patients experiencing mental health issues" pre-session to 24 (85.7%) post-session. When asked, 15 students (53.5%) agreed or strongly agreed with the statement "I understand common mental conditions and their impacts on patients" prior to the session which increased to 24 students (85.7%) post-session.
Twenty-nine participants (nursing = 19, medicine = 10) completed both pre- and post-intervention questionnaires. Rank-based regression models were used to examine the effect of programme (medicine vs nursing) and year of study on post-intervention Likert scores. Table 1 provides a summary of these results.
Wilcoxon signed-rank tests demonstrated significant improvements from pre- to post-intervention for six of the seven items (all p ≤ 0.001), with median increases ranging from 0.5 to 1.5 Likert points. The largest median increase was observed for “I feel confident collaborating with students from other health professions” (median change = 1.5, p < 0.001), followed by “I feel prepared to respond to a mental health crisis in a clinical setting” and “I understand the roles of other health professionals in the care of patients with mental health needs” (both median change = 1.0, p < 0.001). “Interprofessional teamwork is essential for effective mental healthcare delivery” showed minimal change (median change = 0.0) but remained statistically significant (p = 0.013), likely due to a high pre-intervention median of 5.0. Effect sizes (r) ranged from 0.47 to 0.83, indicating moderate to large magnitudes of change.
Year of study was a consistent positive predictor of higher post-intervention scores across all items (β range = 2.65-3.27, all p < 0.001), indicating that students in later years reported greater perceived competence and confidence. Full regression results are seen in Table 2.
Programme was a significant predictor for five of the seven items, with medicine students scoring lower than nursing students after adjusting for year of study. For example, medicine students reported lower confidence in communicating with patients experiencing mental health issues (β = -12.15, 95% CI = -17.19 to -7.11, p < 0.001) and in responding to a mental health crisis in a clinical setting (β = -9.45, 95% CI = -14.55 to -4.35, p < 0.001). No statistically significant programme effect was observed for understanding the roles of other health professionals (p = 0.057) or valuing the contribution of different healthcare disciplines (p = 0.059).
Qualitative data analysis
The post-session questionnaire asked the students what they found most valuable about this simulation and four major themes emerged from the codes. Table 3 provides a summary of these four main themes.
Working Collaboratively
This theme emerged from the following codes: working together and learning about the value of collaboration. Students repeatedly highlighted the value of working with other professionals and working as a multidisciplinary team which is keeping with real practice on the wards and in many clinical environments (quotes 1-4).
Understanding Professional Roles and Skill Sets
This theme comprised the following codes: learning about each other’s roles and learning how to split tasks. Both codes were commonly found in student responses about the valuable aspects of the simulation. The code learning about each other’s roles featured more heavily in the medical student’s responses compared to nursing students. Further, medical students appeared to appreciate nursing students' roles and responsibilities (quotes 5-8).
Confidence in Managing Mental Health Patients
This theme originated from the codes, confidence in mental health management, and understanding the scope of mental health presentations. Students highlighted the value of learning how to manage common mental health presentations and how to care for patients experiencing mental health crisis in their responses (quotes 9-10). This theme is also reflected in the students' increased confidence when rating their ability to manage mental health presentations in the pre- and post-session questionnaire.
Improving Communication
This theme encompassed the valuable learning about the importance of clear communication with each other and with the patients. Students found that the simulation provided an opportunity to become more confident in asking questions they perceived as more difficult, and they acknowledged the value in learning how to communicate effectively in situations specific to mental health presentations (quotes 11-12).
Discussion
This mixed methods study aimed to review the role of mental health interprofessional simulations in undergraduate nursing and medical students from two different universities. Following the simulations, the students reported substantial increases in confidence for managing mental health patients, working with other healthcare students and managing those in acute MH crisis. In addition, there was an increase in appreciating the need for an interprofessional approach when managing mental health patients and understanding the different, applicable roles in these circumstances. The qualitative analysis revealed four main themes: working collaboratively, understanding professional roles and skill sets, increasing confidence in managing MH patients, and improving communication.
Our research aligns with current literature regarding the importance of IPE within healthcare. In particular, this study highlights the value of IPSL in increasing student confidence in working with other healthcare professionals and understanding their roles within the clinical setting. This study adds to the importance of maintaining IPSL within the medical curricula to ensure that healthcare professionals work effectively together [16]. This is also additionally supported by the World Health Organisation (WHO) who highlighted that teaching within a multi-professional setting in student years can increase effective teamwork between healthcare professionals [17].
On completion of a scoping review, only one study by Attoe et al. [18] has looked at the role of mental health simulations in the early stages of professional training. The study emphasises the value of IPSL within undergraduate healthcare students at both an individual and professional level in hope that there would be longer-term benefits seen in clinical care delivered by the participants. Although we have not directly studied the potential future benefits of including IPSL at an undergraduate level, the qualitative data suggests an increasing appreciation for working collaboratively with other healthcare members and an increasing confidence within a mental health setting. Therefore, it is suggestive that the use of these learning exercises in undergraduates is likely to change and adapt patient clinical care in the future, although this is difficult to measure in the long term.
The scenarios used in this study were created in clinical environments such as the emergency department and general practice. This was designed in order to provide overlap between mental health and physical health in patients. All the nursing students involved were adult nursing students, and therefore, placing them in these clinical settings facilitated increased psychological and sociological fidelity. There is evidence to suggest that close alignment with their current roles facilitates important practice change [19].
Limitations
Several limitations are to be acknowledged. The study includes a small sample size of 29 students from two different universities participating in an interprofessional, interuniversity simulation. Therefore, the data is not representative of all UK universities, and we do not know how this study fits within the national context of undergraduate education. The post-session questionnaire was completed immediately following the scenario, and there has not been any long-term follow-up of the students to assess the impact of the IPLS after graduation or how it has affected their clinical work and attitudes.
A further limitation to highlight is the use of independently developed questionnaires in this study. They had not undergone formal validation for reliability or construct validity. Hence, there is a potential for underlying assumptions and researcher bias when completing the thematic analysis.
Future research
Further additional research is required to review the use of IPSL in undergraduate medical and nursing degrees and its role in evaluation of mental health conditions in adult medicine. The differences and impact of its use in undergraduate education should be compared to its use in postgraduate education and its role in both curricula. The timing of introduction into undergraduate education should also be considered in further research.
Conclusions
This study has shown that interprofessional learning through the form of mental health simulation can improve healthcare students’ confidence in managing acute MH crisis, understanding of professionals’ roles, and collaborative working. These findings align with existing literature and further reinforce the value of interprofessional learning to prepare students for clinical environments and working within a multiple disciplinary team (MDT). This area would benefit from further research evaluating the long-term impact of incorporating interprofessional simulation into medical and nursing curricula.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Centre for the Advancement of Interprofessional Education: Interprofessional education: a definition 9 2025 2002 http://www.caipe.org.uk
- 2Interprofessional education: definitions, student competencies, and guidelines for implementation Am J Pharm Educ Buring SM Bhushan A Broeseker A Conway S Duncan-Hewitt W Hansen L Westberg S 59732009 http://pubmed.ncbi.nlm.nih.gov/19657492/1965749210.5688/aj 730459 PMC 2720355 · doi ↗ · pubmed ↗
- 3Evaluations of Interprofessional Education: A United Kingdom Review for Health and Social Care Centre for the Advancement of Interprofessional Education in Primary Health and Community Care Barr H Freeth D Hammick M London Centre for the Advancement of Interprofessional Education 2000
- 4Interprofessional education: the student perspective J Interprof Care Lumague M Morgan A Mak D 2462532020061677779210.1080/13561820600717891 · doi ↗ · pubmed ↗
- 5Simulation: a panacea for interprofessional learning?J Interprof Care Reeves S van Schaik S 1671692620122252415910.3109/13561820.2012.678183 · doi ↗ · pubmed ↗
- 6Simulated interprofessional education: an analysis of teaching and learning processes J Interprof Care van Soeren M Devlin-Cop S Macmillan K Baker L Egan-Lee E Reeves S 43444025201110.3109/13561820.2011.59222921899398 · doi ↗ · pubmed ↗
- 7Simulation as a teaching strategy for nursing education and orientation in cardiac surgery Crit Care Nurse Rauen CA 465124200415206295 · pubmed ↗
- 8Features and uses of high-fidelity medical simulations that lead to effective learning: a BEME systematic review Med Teach Issenberg SB Mc Gaghie WC Petrusa ER Lee Gordon D Scalese RJ 10282720051614776710.1080/01421590500046924 · doi ↗ · pubmed ↗