Impact of nasal and inhaled corticosteroids on SARS-CoV-2 infection susceptibility
Christian Rosas-Salazar, Tebeb Gebretsadik, Max A. Seibold, Camille M. Moore, Samuel J. Arbes, Leonard B. Bacharier, Steven M. Brunwasser, Carlos A. Camargo, William D. Dupont, Glenn T. Furuta, Rebecca S. Gruchalla, Ruchi S. Gupta, Daniel J. Jackson, Christine C. Johnson

TL;DR
Nasal and inhaled corticosteroids may increase SARS-CoV-2 infection risk in adults but not in children, according to a surveillance study.
Contribution
This study is the first to show age-dependent associations between corticosteroid use and SARS-CoV-2 infection risk in adults and children.
Findings
NCS and ICS use were linked to higher SARS-CoV-2 infection risk in adults.
No association was found between corticosteroid use and infection risk in children.
The associations were modified by age, with stronger effects observed in adults.
Abstract
It is unknown whether nasal corticosteroid (NCS) or inhaled corticosteroid (ICS) use impacts the susceptibility to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. We sought to examine the associations of NCS and ICS use with the risk of SARS-CoV-2 infection among individuals with allergic rhinitis or asthma. This is a prospective, multicenter, SARS-CoV-2 surveillance study of households with children. Nasal swabs were obtained from participants every 2 weeks with additional collections based on coronavirus disease 2019–related symptoms. In our primary adjusted models, we examined the association of NCS or ICS use at study entry (in participants with allergic rhinitis or asthma, respectively) with the time to the first SARS-CoV-2–positive quantitative PCR testing using Cox proportional hazard regression. There were 2211 participants in the 1113 households…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
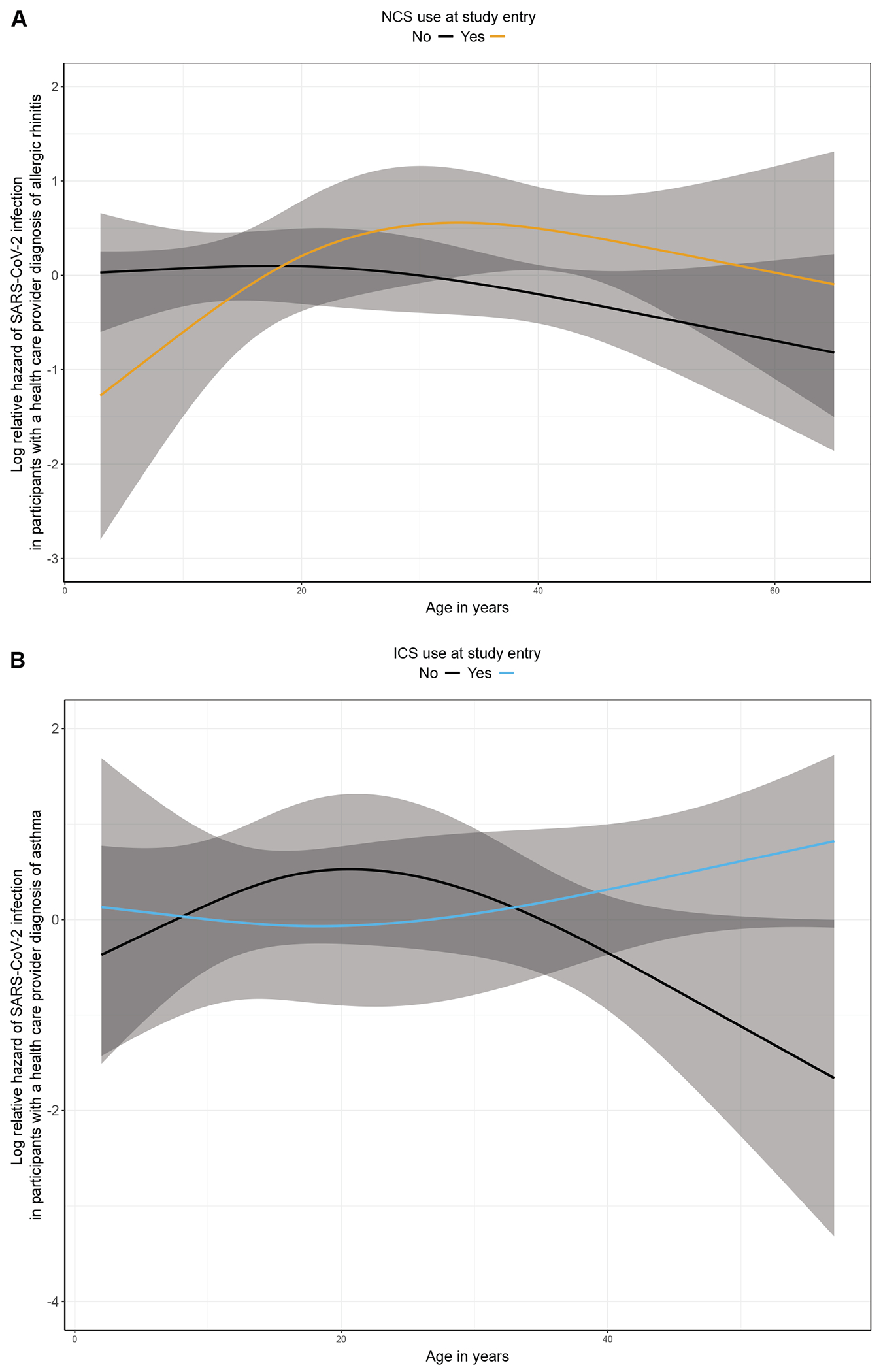 Figure 1
Figure 1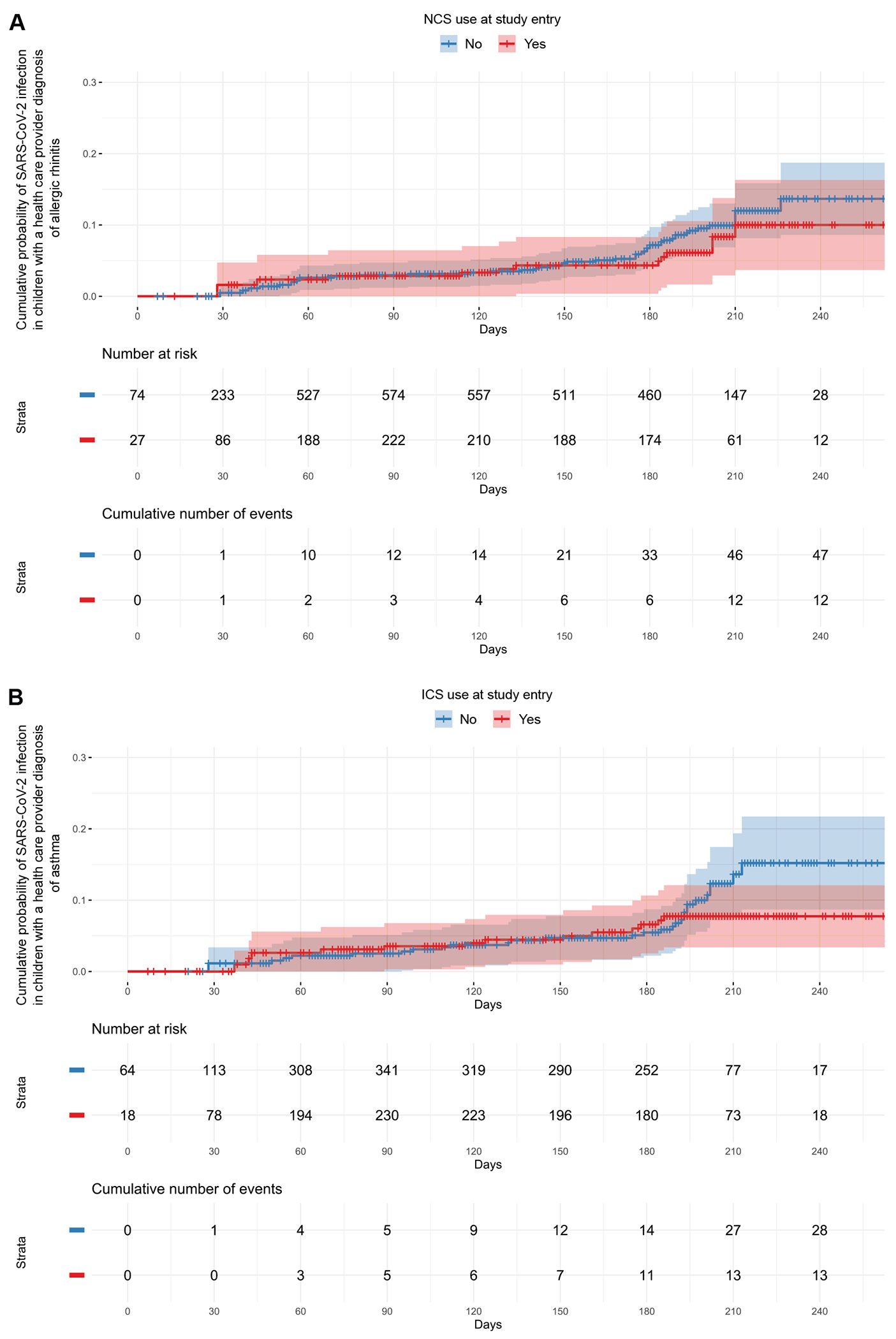 Figure 2
Figure 2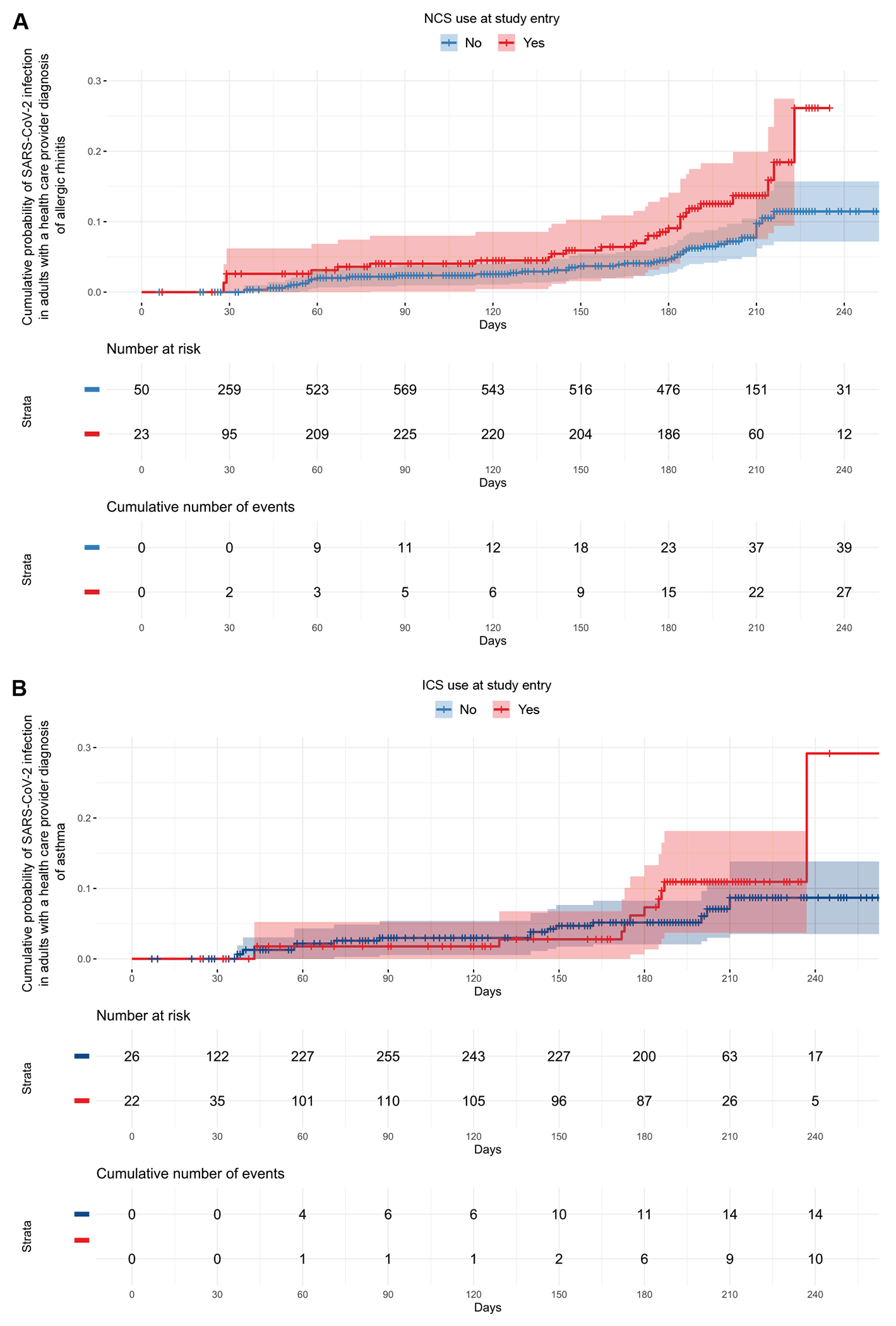 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSARS-CoV-2 and COVID-19 Research · Respiratory viral infections research · COVID-19 Clinical Research Studies
The upper respiratory tract (URT) is typically the site of primary infection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the respiratory virus responsible for the coronavirus disease 2019 (COVID-19) pandemic.^1,2^ Following airborne exposure to SARS-CoV-2, certain host factors (such as differences in the expression of cell receptors, intracellular signaling, and other host defense pathways) can determine the effective entry of SARS- CoV-2 into the URT cells and the establishment of infection.^2–4^
Topical airway corticosteroids (such as nasal corticosteroids [NCS] or inhaled corticosteroids [ICS]) are the mainstay of treatment for the long-term management of allergic rhinitis and asthma.^5,6^ These commonly used medications may influence the SARS-CoV-2 URT cell entry process and acute immune response,^4,7–11^ leading us to hypothesize that the risk of SARS-CoV-2 infection differs among individuals who use topical airway corticosteroids when compared to those who do not use these medications. This is one of the hypotheses in the design of the HEROS (Human Epidemiology and RespOnse to SARS-CoV-2 Study), a prospective, multicenter, SARS-CoV-2 surveillance study of households enriched for children and adults with allergic rhinitis and asthma.
METHODS
Overview of the study population
The HEROS study population included households with children (ages <21 years) participating in 20 National Institutes of Health–funded cohorts focused on atopic diseases in 12 US cities between May 2020 and February 2021. Enrollment in HEROS required the participation of the cohort-participating child and 1 primary adult caregiver living in the same household. Two other household members (1 child and 1 other adult caregiver) could also enroll. To minimize confounding by indication, we restricted the study population to participants who self-reported a prior health care provider diagnosis of allergic rhinitis (for the analyses of NCS use) or asthma (for the analyses of ICS use). Participants were followed for at least 24 weeks and up to 28 weeks after enrollment. The detailed methods for HEROS have been previously reported.^12,13^ The US Department of Health and Human Services Office for Human Research Protections and the Institutional Review Boards of all participating institutions deemed the study a public health surveillance study. Primary adult caregivers were provided an online study information fact sheet, which was a consent-like document containing components of the US Federal Policy for the Protection of Human Subjects. To enroll, primary adult caregivers were required to agree that they read, understood, and reviewed this online study information fact sheet with all participating household members. This sheet included an option to select having the study site contact the primary adult caregiver to answer any questions.
Study questionnaires and NCS and ICS ascertainment
Primary adult caregivers completed study entry and end-of-study questionnaires that collected comprehensive information on sociodemographic factors, current and past medical history (including a prior health care provider diagnosis of allergic rhinitis or asthma), and current use of medications (including use of topical airway corticosteroids). These questionnaires were primarily developed from previously validated instruments (including selected items from the International Study of Asthma and Allergies in Childhood questionnaire^14^) and were used to ascertain self-report use of NCS and ICS at study entry and end of study. In addition, primary adult caregivers completed biweekly questionnaires to capture potential exposures to SARS-CoV-2 and weekly questionnaires to capture symptoms related to COVID-19. Similar to the 2020 US Census Operational Plan, primary adult caregivers completed each questionnaire on behalf of all household members.^15^ The questionnaires were completed remotely via online platforms, short text messages, or telephone communications with the study site staff.
SARS-CoV-2 testing
Self- or caregiver-collected nasal swabs were obtained from participants every 2 weeks between May 2020 and February 2021, which was the COVID-19 pandemic period almost entirely before SARS-CoV-2 vaccine availability. In addition, participants completed weekly symptom questionnaires. If any household member developed symptoms related to COVID-19 during this time, a prespecified algorithm prompted an additional self or caregiver nasal swab collection from all participants. SARS-CoV-2 quantitative PCR testing was conducted in all nasal swabs collected using the US Centers for Disease Control and Prevention SARS-CoV-2 N1/N2 and ribonuclease P housekeeping gene assays as previously described.^12,13^
Blood allergen-specific IgE testing
Self- or caregiver-collected capillary blood samples were obtained from participants ages >2 years at least once during the study using the Tasso home collection device (Tasso Inc, Seattle, Wash). Multiplex specific IgE testing to 112 aeroallergens and foods from 48 different sources was conducted in the capillary blood samples collected using the ImmunoCAP ISAAC assay (Phadia AB, Portage, Mich).
Statistical analyses
Descriptive statistics are presented as median (interquartile range [IQR]) for continuous variables and frequency (percentage) for categorical variables. We examined the association of NCS or ICS use at study entry with the time to the first SARS-CoV-2–positive quantitative PCR testing by plotting Kaplan-Meier cumulative morbidity curves and by conducting Cox proportional hazard regression with a robust sandwich covariance estimate to account for clustering of participants within a household. The assumption of proportionality of the primary exposure variables was assessed using a global test based on Schoenfeld residuals and visual residual plots checking. Because there was no clear violation of the proportional hazards assumption, we assumed proportional hazards for all variables. To account for geographic differences in SARS-CoV-2 infection risk over time, baseline hazards were stratified by study site. The primary adjusted models included the participant’s age (as a nonlinear term with restricted cubic splines), sex, race and ethnicity (categorized as non-Hispanic White vs other), and body mass index percentile^16^ as a priori selected covariates. We also tested for interactions between NCS or ICS use at study entry and age, sex, and race and ethnicity, separately by adding cross-product terms to the primary adjusted models.
In supplementary analyses, we built secondary adjusted models by adding the following covariates to the primary adjusted models: (1) the area deprivation index (a marker of socioeconomic disadvantage at the neighborhood level that incorporates theoretical domains of income, education, employment, and housing quality),^17^ (2) use of other topical airway corticosteroids at study entry, (3) a modified comorbidity index (based on the Charlson comorbidity index [Table E1 in this article’s Online Repository at www.jacionline.org]^18^), (4) current smoking at study entry, (5) a prior health care provider diagnosis of diabetes type 1 or 2, and (6) use of blood pressure medications (such as angiotensin-converting enzyme [ACE] inhibitors or angiotensin II receptor blockers) at study entry.
To assess whether misclassification of the exposure or the selection of the study population could have impacted our results, we conducted sensitivity analyses by only including participants who had data on NCS and ICS use at both study entry and end of study, as well as only including participants with allergic rhinitis who had evidence of allergen sensitization by blood allergen-specific IgE testing. Likewise, we evaluated the specificity of the associations and potential confounding by the underlying disease severity through sensitivity analyses examining (1) the association of use of other allergic rhinitis medications (eg, leukotriene receptor antagonists, nasal antihistamines, or oral antihistamines) or other asthma controllers (eg, leukotriene receptor antagonists, long-acting muscarinic antagonists, or biologic therapies) at study entry with the risk of SARS-CoV-2 infection, and (2) the relationship between the number of allergic rhinitis medications or asthma controllers used at study entry (as markers of allergic rhinitis and asthma severity, respectively) and the risk of SARS-CoV-2 infection.
Statistical analyses used 2-sided P values and significance was defined as P < .05. Statistical analyses were performed using R version 4.0.1 (R Foundation, Vienna, Austria).^19^
RESULTS
Baseline characteristics of the study population
There were 4142 participants from 1394 households enrolled in HEROS who contributed at least 1 nasal swab between May 2020 and February 2021. The baseline characteristics of these 4142 participants have been described elsewhere.^13^ Of these 4142 participants, 2211 participants (53%) (age range: 0-80 years) from 1113 households had a prior health care provider diagnosis of allergic rhinitis (n = 1892 [46%]) or asthma (n = 1150 [28%]) and comprised the current study population. Among these 2211 participants there were 1164 children (53%, median age 12 [IQR: 7-15] years) and 1047 adults (47%, median age 41 [IQR: 36-47] years). The majority of these 2211 participants were female (1285 [58%]) and non-Hispanic White (1220 [57%]) (Table I). Of the 2211 participants, 145 (7%) developed a SARS-CoV-2 infection during the study period.
In comparison to participants with allergic rhinitis who were not using NCS at study entry, those who were using NCS at study entry were more likely to be of a race and ethnicity other than non-Hispanic White, ever had asthma, and be using ICS at study entry, and less likely to be currently smoking at study entry (Table I). Participants with asthma who were using ICS at study entry were younger and more likely to be of a race and ethnicity other than non-Hispanic White, be using NCS at study entry, and ever had allergic rhinitis than those who were not using ICS at study entry (Table I).
Effect modification by participant’s age
In participants with allergic rhinitis, there was a statistically significant effect modification of the association of NCS use at study entry with the risk of SARS-CoV-2 infection by age (P for interaction = .02) (Fig 1, A). Similarly, the effect of ICS use at study entry on the risk of SARS-CoV-2 infection among participants with asthma was modified by age (P for interaction = .047) (Fig 1, B). There was no statistically significant effect modification of sex or race and ethnicity on the associations of NCS or ICS use at study entry with the risk of SARS-CoV-2 infection among participants with allergic rhinitis or asthma, respectively (P > .05 for all interaction terms). Based on these results, subsequent statistical analyses were conducted separately in children (<21 years of age) and adults (≥21 years of age).
Use of NCS in participants with allergic rhinitis and the risk of SARS-CoV-2 infection
NCS use at study entry was not associated with the risk of SARS-CoV-2 infection among children with allergic rhinitis in our primary adjusted model (adjusted hazard ratio [aHR] = 0.65, 95% CI:0.27-1.57, P = .3) (Table II and Fig 2, A). In contrast, adults with allergic rhinitis who were using NCS at study entry had ~90% higher risk of SARS-CoV-2 infection than those who were not using NCS in our primary adjusted model (aHR = 1.88, 95% CI: 1.14-3.12, P = .01) (Table III and Fig 3, A). In adults with allergic rhinitis, the effect size and statistical significance of the association remained consistent in secondary adjusted models that included the area deprivation index, ICS use at study entry, the modified comorbidity index, current smoking at study entry, a prior health care provider diagnosis of diabetes type 1 or 2, and use of blood pressure medications at study entry as additional covariates (Table III).
In sensitivity analyses, the risk of SARS-CoV-2 infection remained increased among adults with allergic rhinitis using NCS at both study entry and end of study compared to those not using these medications at any time point (Table E2 in this article’s Online Repository at www.jacionline.org). Restricting analyses to the subgroup of adults with allergic rhinitis who had evidence of allergen sensitization by blood allergen-specific IgE testing revealed similar directionality and effect size, although this reduced the size of the study population and the association was not statistically significant (Table E3 in this article’s Online Repository at www.jacionline.org). Use of medications for allergic rhinitis other than NCS or the number of allergic rhinitis medications used (a marker of allergic rhinitis severity) at study entry was not associated with the risk of SARS-CoV-2 infection among adults with allergic rhinitis (Tables E4 and E5 in this article’s Online Repository at www.jacionline.org).
Use of ICS in participants with asthma and the risk of SARS-CoV-2 infection
There was no association of ICS use at study entry with the risk of SARS-CoV-2 infection among children with asthma in our primary adjusted model (aHR = 0.86, 95% CI = 0.40-1.87, P = .7) (Table II and Fig 2, B). Similar results were obtained when restricting analyses to the subgroup of children with asthma ages 5 years and older (Table E6 in this article’s Online Repository at www.jacionline.org). In contrast, adults with asthma who were using ICS at study entry had ~2-fold higher risk of SARS-CoV-2 infection than those who were not using ICS in our primary adjusted model (aHR = 2.15, 95% CI: 1.003-4.63, P = .049) (Table III and Fig 3, B). In adults with asthma, the effect size and statistical significance of this association remained consistent in secondary adjusted models that included ICS use at study entry, the modified comorbidity index, and use of blood pressure medications at study entry as additional covariates (Table III). Likewise, the effect size of this association remained similar in secondary adjusted models that included the area deprivation index, current smoking at study entry, and a prior health care provider diagnosis of diabetes type 1 or 2 as additional covariates but the association was not statistically significant (Table III).
The risk of SARS-CoV-2 infection was not increased among adults with asthma when ascertaining ICS use at both study entry and end of study (Table E7 in this article’s Online Repository at www.jacionline.org). Use of asthma controllers other than ICS at study entry was not associated with the risk of SARS-CoV-2 infection among adults with asthma (Table E8 in this article’s Online Repository at www.jacionline.org). However, the number of asthma controllers used (a marker of asthma severity) at study entry was positively associated with the risk of SARS-CoV-2 infection in this age group (Table E9 in this article’s Online Repository at www.jacionline.org).
In adults with allergic rhinitis or asthma, the combined use of NCS and ICS at study entry did not increase the risk of SARS-CoV-2 infection. However, adults with allergic rhinitis or asthma using only NCS at study entry had a risk of SARS-CoV-2 infection that was intermediate between the risk of those using only ICS at study entry and that of those using both NCS and ICS at study entry (Table E10 in this article’s Online Repository at www.jacionline.org).
DISCUSSION
Our findings suggest that the risk of SARS-CoV-2 infection is increased in adults who use NCS but not in children. Similar, albeit less consistent, age-dependent findings were observed for ICS use. Our findings are important as topical airway corticosteroids are among the most commonly used medications for the management of pediatric and adult allergic and respiratory disorders,^5,6^ and understanding their safety profile could aid COVID-19 public health measures. These findings, while informative, are constrained by the observational study design and do not imply causation.
We can only hypothesize on the potential mechanisms underlying the association of NCS use and the risk of SARS-CoV-2 infection in adults. The entry of SARS-CoV-2 into the URT cells and eventually host infection starts with its binding to respiratory epithelial cell receptors (such as the ACE2 receptor), subsequent membrane fusion, and ultimately viral replication and release.^1,2^ In addition to blunting the local immune response, NCS can impact many of these steps and lead to major changes in the nasal microenvironment, which could explain our results.^1,9,10^ However, little is known about the relationship between NCS use and the SARS-CoV-2 URT cell entry process in humans. Interestingly, available in vitro data suggest that NCS could decrease the expression of ACE2 receptors in respiratory epithelial cells, as well as impair the SARS-CoV-2 replication process, which—in contrast to our findings—should lower the risk of SARS-CoV-2 infection.^20^ On the other hand, NCS use in atopic adults can decrease the levels of type-2 cytokines (such as IL-13) or eosinophils in the URT, which could then upregulate the expression of ACE2 receptors in respiratory epithelial cells and possibly increase the risk of SARS-CoV-2 infection.^10,21–26^ To our knowledge, while studies examining the effect of NCS use on COVID-19 morbidity in SARS-CoV-2–infected adults have had conflicting results,^27–30^ no other studies have examined the association of NCS use with the risk of SARS-CoV-2 infection in children or adults.
Our findings of a differential effect of NCS use on the risk of SARS-CoV-2 infection in children compared to adults are in line with described age-dependent effects of SARS-CoV-2 on several COVID-19 outcomes.^31,32^ For example, studies early in the COVID-19 pandemic suggested that children were less likely to be infected with SARS-CoV-2 (posited to be due in part to a lower expression of ACE2 receptors in respiratory epithelial cells compared to adults).^33,34^ However, in the HEROS study population, we previously demonstrated that the risk of SARS-CoV-2 infection does not differ between children and adults but rather children are substantially more likely to have asymptomatic or paucisymptomatic COVID-19 and thus clinically underrecognized SARS-CoV-2 infection.^13^
The risk of SARS-CoV-2 infection among adults using NCS remained increased after controlling for various potential confounders, but—as it is the case for all observational studies—our results could have been biased by confounding. To prevent confounding by indication in our analyses of NCS use, we only included participants with allergic rhinitis. However, NCS use can be related to the severity of allergic rhinitis, which may be acting as an additional confounder. To address this, we conducted a separate analysis to examine the association of the number of allergic rhinitis medications (a marker of underlying allergic rhinitis severity) with the risk of SARS-CoV-2 infection in adults and found no association. Yet, the independent effects of NCS use and the severity of allergic rhinitis on the risk of SARS-CoV-2 are difficult to disentangle and we lacked data on other markers of allergic rhinitis severity.
Some of our findings suggest that the risk of SARS-CoV-2 infection could also be increased in adults who use ICS. However, we found a relationship between the number of asthma controllers (a marker of the underlying asthma severity) and the risk of SARS-CoV-2 infection in adults. These findings suggest that confounding could have biased the association between ICS use and the risk of SARS-CoV-2 in adults, which prevents us from establishing firm conclusions about this relationship. Of note, it is certainly possible that only NCS (and not ICS) impact the risk of SARS-CoV-2 in adults, as the URT is the site of primary infection of SARS-CoV-2 and the first line of defense against COVID-19. The URT is not only the entry portal of the airways but also contains the highest percentage of ACE2-expressing respiratory epithelial cells across all the airways.^3,4^ In contrast to NCS, ICS are largely deposited in the more distal and lower airways, which are anatomical regions important in the severity of COVID-19 (an outcome for which ICS have demonstrated success in some but not all clinical trials^28,35,36^) but are likely less relevant for establishing SARS-CoV-2 infection.^1,4,37,38^
The strengths of our study include the prospective surveillance study design, the enrollment of participants across the US, the overall young population, and the careful ascertainment of the exposure and outcome of interest. We should also acknowledge some limitations in addition to confounding. First, it is possible that the effect of using topical airway corticosteroids on SARS-CoV-2 infection could depend on the underlying inflammatory phenotype, the SARS-CoV-2 strain, or on the potency, formulation, or pharmacodynamics of the specific drug, which we could not examine.^11,23,33^ Second, we may not have had sufficient statistical power to detect some associations. Third, there could have been misclassification of the exposure, as we lacked data on medication adherence, or misclassification of the outcome, based on the nasal sampling interval and missed biospecimens. Similarly, we defined allergic rhinitis based on self-report of a prior health care provider diagnosis, which could have led to misclassification of the study population. While we also conducted sensitivity analyses by only including participants with allergic rhinitis who had evidence of allergen sensitization by blood allergen-specific IgE testing, this led to a decreased sample size. Last, because the underlying atopic inflammation in persons with allergic rhinitis or asthma could impact SARS-CoV-2 URT cell entry process,^33^ our results may not be generalizable to those using NCS or ICS for other medical conditions. However, allergic rhinitis and asthma are the most common indications and account for the majority of use of topical airway corticosteroids in both the pediatric and adult population.
In summary, our results suggest the risk of SARS-CoV-2 infection is increased among adults who use NCS and potentially among those who use ICS when compared to those who do not use these medications, whereas we found no association of NCS or ICS use and SARS-CoV-2 infection in children. While the results of this observational study should be interpreted with caution and should not preclude the prescription of topical airway corticosteroids, they emphasize the need to conduct studies to understand potential mechanisms that could explain these findings and confirm whether the age-dependent relationship between NCS use and the risk of SARS-CoV-2 infection is causal. Follow-up studies are important for informing patient care, clinical guidelines, and COVID-19 public health measures.
Supplementary Material
1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gallo O, Locatello LG, Mazzoni A, Novelli L, Annunziato F. The central role of the nasal microenvironment in the transmission, modulation, and clinical progression of SARS-Co V-2 infection. Mucosal Immunol 2021;14:305–16.33244161 10.1038/s 41385-020-00359-2PMC 7690066 · doi ↗ · pubmed ↗
- 2Jackson CB, Farzan M, Chen B, Choe H. Mechanisms of SARS-Co V-2 entry into cells. Nat Rev Mol Cell Biol 2022;23:3–20.34611326 10.1038/s 41580-021-00418-x PMC 8491763 · doi ↗ · pubmed ↗
- 3Alu A, Chen L, Lei H, Wei Y, Tian X, Wei X. Intranasal COVID-19 vaccines: from bench to bed. E Bio Medicine 2022;76:103841.10.1016/j.ebiom.2022.103841 PMC 878560335085851 · doi ↗ · pubmed ↗
- 4Hou YJ, Okuda K, Edwards CE, Martinez DR, Asakura T, Dinnon KH 3rd, SARS-Co V-2 reverse genetics reveals a variable infection gradient in the respiratory tract. Cell 2020;182:429–46.e 14.32526206 10.1016/j.cell.2020.05.042PMC 7250779 · doi ↗ · pubmed ↗
- 5Dykewicz MS, Wallace DV, Amrol DJ, Baroody FM, Bernstein JA, Craig TJ, Rhinitis 2020: A practice parameter update. J Allergy Clin Immunol 2020;146:721–67.32707227 10.1016/j.jaci.2020.07.007 · doi ↗ · pubmed ↗
- 6Levy ML, Bacharier LB, Bateman E, Boulet LP, Brightling C, Buhl R, Key recommendations for primary care from the 2022 Global Initiative for Asthma (GINA) update. NPJ Prim Care Respir Med 2023;33:7.36754956 10.1038/s 41533-023-00330-1PMC 9907191 · doi ↗ · pubmed ↗
- 7Sungnak W, Huang N, Becavin C, Berg M, Queen R, Litvinukova M, SARS-Co V-2 entry factors are highly expressed in nasal epithelial cells together with innate immune genes. Nat Med 2020;26:681–7.10.1038/s 41591-020-0868-6PMC 863793832327758 · doi ↗ · pubmed ↗
- 8Conway FM, Bloom CI, Shah PL. Susceptibility of patients with airway disease to SARS-Co V-2 infection. Am J Respir Crit Care Med 2022;206:696–703.35549839 10.1164/rccm.202111-2547 PPPMC 9799128 · doi ↗ · pubmed ↗