Reversible Bradycardia and Transient Loss of Consciousness With Undiagnosed Hypothyroidism: A Case Report
Amir Khan, Muhammad Umair Sultan, Noor Un Nahar, Anita Rahman, Minahil Mukhtar

TL;DR
A 62-year-old woman with undiagnosed hypothyroidism experienced heart and neurological symptoms that resolved after treatment.
Contribution
Highlights hypothyroidism as a rare cause of bradyarrhythmia and syncope, emphasizing the need for early diagnosis.
Findings
Hypothyroidism was identified as the underlying cause of bradyarrhythmia and syncope in a 62-year-old patient.
Symptoms resolved completely with levothyroxine therapy, confirming the diagnosis.
Delayed diagnosis occurred due to initial investigations focusing on neurological and cardiac causes.
Abstract
Hypothyroidism, or an underactive thyroid, is a common endocrine disorder characterized by insufficient production of thyroid hormones by the thyroid gland. It typically presents with non-specific symptoms and sometimes leads to serious cardiac and neurological symptoms. Due to the subtle onset, clinical recognition can be delayed. We present a case of a 62-year-old lady diagnosed with hypothyroidism presenting with bradyarrhythmia precipitating a syncopal attack. Extensive investigations were carried out to rule out a primary neurological or cardiac disorder, leading to diagnostic delays. A diagnosis of hypothyroidism is primarily established through blood tests showing an elevated thyroid-stimulating hormone (TSH) and low free thyroxine (T4) levels. Management involves long-term thyroid hormone replacement therapy, most commonly with levothyroxine, which effectively restores euthyroid…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
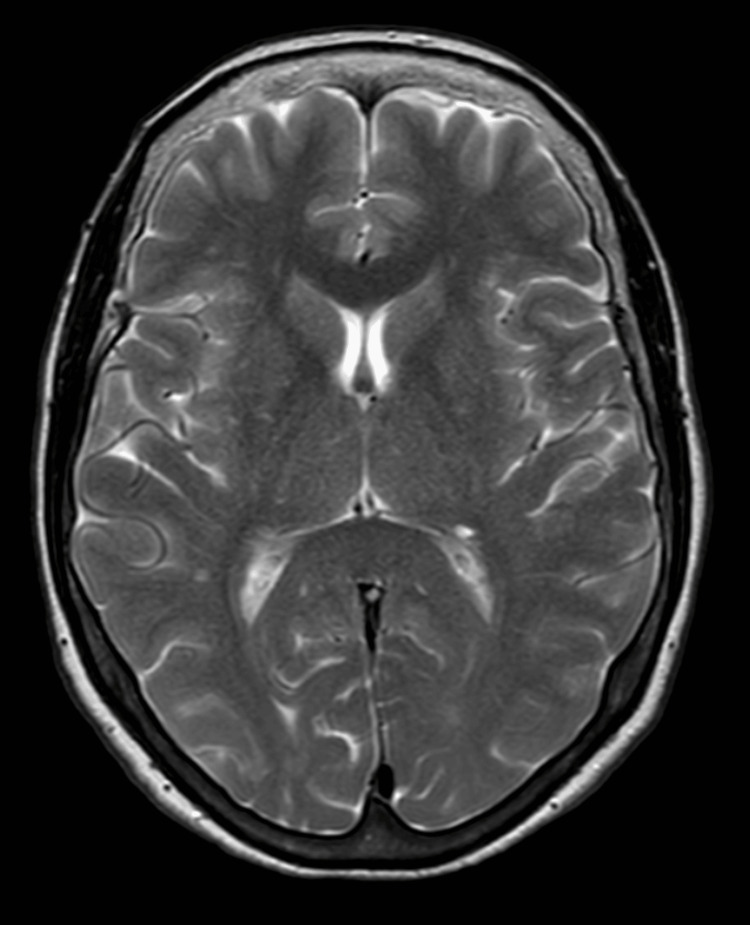 Figure 1
Figure 1 Figure 2
Figure 2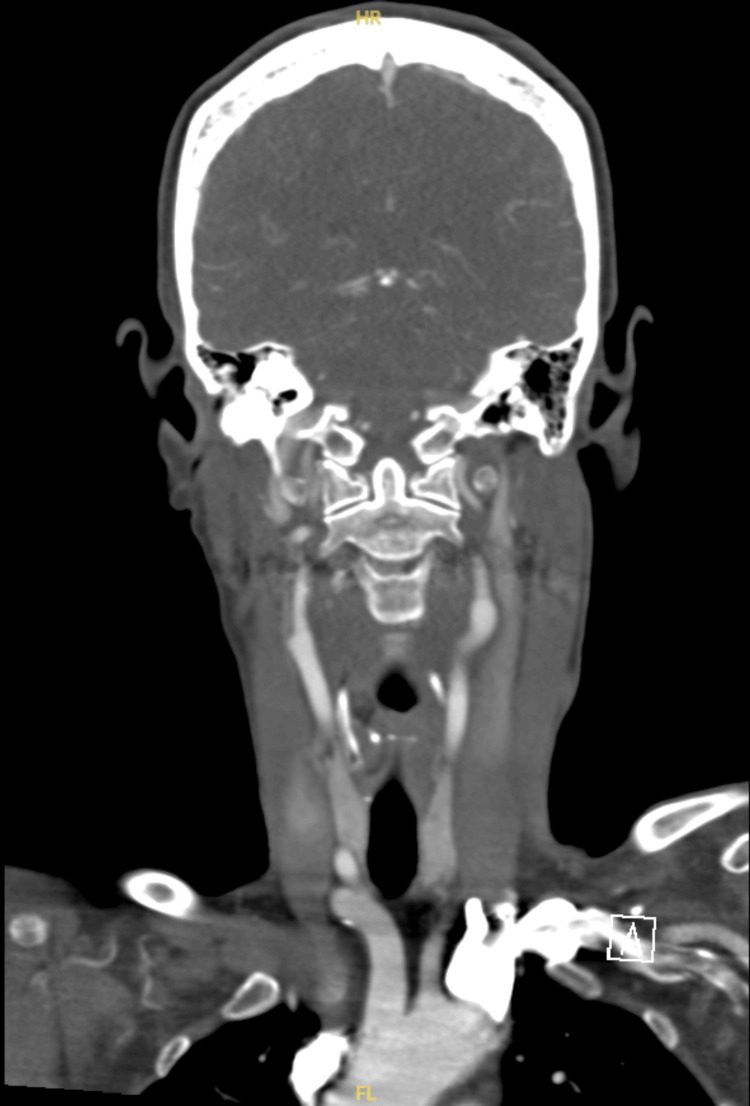 Figure 3
Figure 3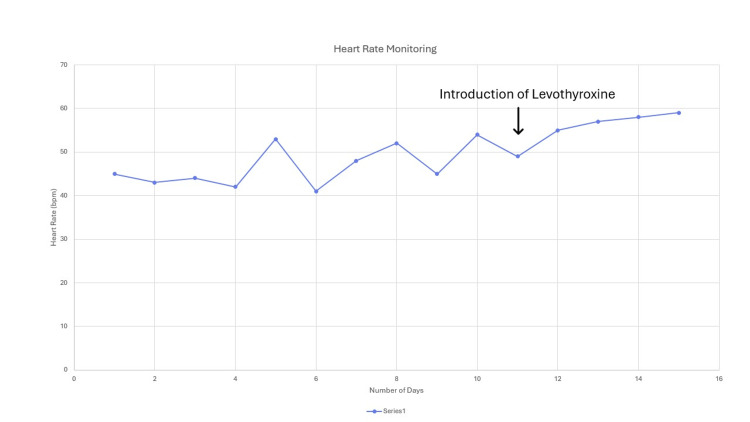 Figure 4
Figure 4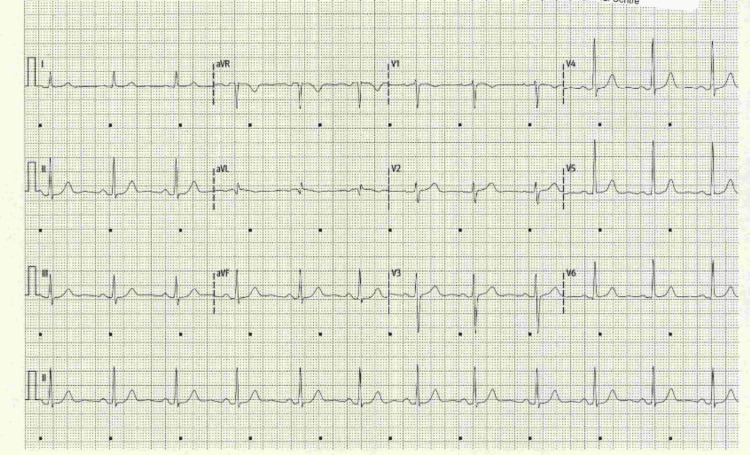 Figure 5
Figure 5| Test | Result | Reference Range | Interpretation |
| Hb (Haemoglobin) | 134 g/L | 120–150 g/L | Normal |
| WCC (White Cell Count) | 4.5 ×10⁹/L | 4.0–11.0 ×10⁹/L | Normal |
| Platelets | 215 ×10⁹/L | 150–400 ×10⁹/L | Normal |
| CRP (C-Reactive Protein) | 1 mg/L | <5 mg/L | Normal (no inflammation) |
| Vitamin B12 | 217 pmol/L | 133–675 pmol/L | Normal |
| Folate | 12.9 nmol/L | >7.0 nmol/L | Normal |
| Vitamin D (25-OH) | 54.1 nmol/L | >50 nmol/L | Sufficient |
| dsDNA | <9.8 IU/mL | 0–27 IU/mL | Normal (SLE unlikely) |
| Anti-CCP | <8 U/mL | 0–17 U/mL | Normal (RA unlikely) |
| ESR (Erythrocyte Sedimentation Rate) | 6 mm/hr | <20 mm/hr | Normal |
| eGFR | >90 mL/min | >90 mL/min | Normal kidney function |
| ANA (Antinuclear Antibody) | Negative | Negative | Normal (autoimmune disease unlikely) |
| INR (Clotting) | 0.9 | 0.8–1.2 | Normal |
| APTT (Clotting) | 21 sec | 25–35 sec | Slightly low (clinically insignificant) |
| HbA1c | 34 mmol/mol | <42 mmol/mol | Normal glycemic control |
| Sodium (Na⁺) | 141 mmol/L | 135–145 mmol/L | Normal |
| Potassium (K⁺) | 3.9 mmol/L | 3.5–5.0 mmol/L | Normal |
| Urea | 3.3 mmol/L | 2.5–7.8 mmol/L | Normal |
| Calcium | 2.26 mmol/L | 2.2–2.6 mmol/L | Normal |
| Phosphate | 1.26 mmol/L | 0.8–1.5 mmol/L | Normal |
| Cholesterol/HDL Ratio | 2.2 | <4.0 | Favorable lipid ratio – Low cardiovascular risk |
| Test | Result | Reference Range | Interpretation |
| TSH (Thyroid-Stimulating Hormone) | 6.4 mU/L | 0.4-4.0 mU/L | Elevated - Suggests hypothyroidism |
| Free T4 (Thyroxine) | 9.2 pmol/L | 10-22 pmol/L | Low - Hypothyroidism |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Disorders and Treatments · Autoimmune Neurological Disorders and Treatments · Ion channel regulation and function
Introduction
Cardiovascular and thyroid hormone functions are interrelated and are regulated by intrinsic homeostatic mechanisms. Elevated levels of thyroid hormone cause hyperadrenergic states such as tachycardia, and depressed levels cause hypo-adrenergic states such as bradycardia [1]. Bradycardia is one of the manifestations of hypothyroidism, but is often overlooked, as the incidence of arrhythmia in hypothyroidism is lower when compared to hyperthyroid patients [2]. Eventually, when patients present, the initial focus of diagnosis is on conditions other than hypothyroidism [3]. It may present with nonspecific symptoms or even life-threatening events such as syncope or sudden loss of consciousness [4]. Considering a prevalence of 24% in women aged 60 years or older, investigating thyroid functions in the context of unexplained bradyarrhythmia is of high clinical relevance [5].
We present a case with an unusual presentation of hypothyroidism - a bradycardia-induced syncopal episode leading to a high-risk situation, a road traffic collision, where the focus was initially on exploring the underlying neurological disorder. We emphasize the value of thorough evaluation in such patients and picking up subtle signs like consistent bradycardia and long-standing constipation, leading to timely diagnosis and prompt management with complete resolution of symptoms.
Case presentation
A 62-year-old English lady was found to be unresponsive in her car after slumping at the wheel and colliding with multiple vehicles. She had no recollection of the event and was noted by paramedics to have a Glasgow Coma Scale (GCS) of E1V2M5. On arrival at the emergency department, her GCS normalized. She had an early warning score (EWS) of three, which was primarily due to her heart rate of 45 bpm. The remaining observations included a respiratory rate of 18, blood pressure of 128/61 mmHg, saturation of 96% on room air, a temperature of 36.2°C, and an alert status on the Alert, Verbal, Pain, Unresponsive (AVPU) scale.
On taking a thorough history, she had dizziness not related to posture, no symptoms of vertigo, chest pain, headache, ear discharge, tinnitus, vision changes, vomiting, or nausea. She reported no fever, rash, or weakness in any part of the body. There was no noticeable head injury. No urinary or bowel changes were reported by the patient. She mentioned that she suffered from constipation. She complained of lower back pain that started after the collision. She mentioned no recent travels and no family history of note. She denied any alcohol abuse or recreational drug use. Her past medical history included known bradycardia diagnosed during a pre-operative evaluation for knee surgery two years prior. Unfortunately, her general practitioner did not investigate bradycardia, and she was not taking any regular medications.
On examination, there were no concerning findings apart from lacerations on the arms and tenderness on palpation of the lower back. Complete neurological evaluation and the rest of the systemic examination were unremarkable. She had a postural drop of 21 mmHg.
The patient was admitted, and a set of baseline investigations and a CT head non-contrast was requested to rule out the possibility of a bleed. Given the unremarkable findings on the CT scan of the brain, a CT aortic arch was done to rule out posterior circulation stroke, which was also ruled out. Heading more in the direction of underlying cardiac pathology, we did a 24-hour Holter monitoring and an echocardiogram as well. Table 1 outlines her baseline blood work up.
Figure 1 shows the MRI brain revealing normal brain parenchyma and ruling out the possibility of a posterior circulation stroke.
MRI brain with no evidence of an acute infarct or any other significant abnormality
ECG on presentation showed sinus bradycardia with normal QRS, PR and QTc intervals (Figure 2).
Electrocardiogram on arrival with sinus bradycardia
Figure 3 shows the image from CT aortic arch and arch vessels of normal caliber with satisfactory anterior and posterior circulation and no evidence of vascular malformation, aneurysm or stenosis.
CT aortic arch showing no obvious abnormality
We carried out 24-hour Holter monitoring to explore the possibility of nodal dysfunctions or underlying arrhythmogenic activity, but it was unsuccessful in finding the cause of the syncopal episode. There was sinus rhythm with persistent bradycardia. Her heart rate ranged from a maximum of 75 bpm to a minimum of 35 bpm. Findings included incidental two dropped beats with compensatory pauses post supraventricular ectopics (SVEs), and one ventricular ectopic (VE). PR and QRS intervals remained within normal limits. These findings were incidental and not potentially contributing to the presentation.
Echocardiogram ruled out structural heart abnormalities, and showed normal left ventricular size with borderline low systolic function of 54% and was otherwise unremarkable. These findings can be attributed to underlying hypothyroidism that was later diagnosed.
In view of the reassuring investigations, we further explored the bradycardia by conducting a simple thyroid hormone profile (Table 2).
She was started on levothyroxine 25 mcg once in the morning and monitored for heart rate. Her postural drop settled, and her heart rate improved significantly. Figure 4 shows a graph of her heart rate during admission.
Plot of the patient's daily heart rate monitoring during the hospital stay, showing an improving trend after starting thyroxine therapy
She was referred to Endocrinology on discharge with advice and information of her medication on day 15. She was seen in six weeks time with repeat thyroid stimulating hormone (TSH) level of 1.8 mIU/L and a repeat ECG. She reported complete resolution of her symptoms and had no new concerns during this time. Figure 5 shows the normal sinus rhythm of the ECG.
Normal sinus rhythm of the electrocardiogram at the six-week follow-up
She has been booked in by her General Practitioner to repeat her thyroid function tests regularly and evaluate the need for changes in the levothyroxine dose.
Discussion
We put forward a case with a dramatic and atypical presentation of hypothyroidism manifesting as reversible bradycardia and orthostatic hypotension leading to a road traffic accident. Sinus bradycardia is a cardiac rhythm initiated from the sinus node with a rate of less than 60 bpm, diagnosed by an ECG. While most of the patients are asymptomatic, some of them present with fatigue, dizziness, light-headedness, syncope or presyncope, and cognitive impairment [6]. A study conducted in 2023 reported a 10.3% rate of bradycardia in hypothyroid patients [7]. Although it is one of the symptoms of hypothyroidism, there is no direct comparison of TSH levels to heart rate to assist in therapeutic hormonal management [1].
Thyroid hormones play an important role in cardiac homeostasis; hypothyroidism can lead to decreased cardiac contractility, atrial compliance, preload, and cardiac output, and increased systemic vascular resistance secondary to endothelial dysfunction [8]. There is less β-adrenergic receptor expression and decreased sensitivity to existing receptors, eventually blunting the response to increased catecholamines [9]. Both systolic and diastolic dysfunction are associated with hypothyroidism, and it can accompany arrhythmia such as premature ventricular beats, ventricular tachycardia, or even torsade de pointes [10]. Although diastolic hypertension is common in hypothyroidism, autonomic dysfunction with disruption of the baroreceptor reflex arc can cause orthostatic hypotension, which is proven to be reversible with thyroid hormone replacement [11]. Thyroid hormones, mostly the active form T3 (Triiodothyronine), play an important role in cardiovascular physiology, modulating cardiac contractile performance and contributing to electrophysiological remodeling [12].
When bradyarrhythmia arises, one should rule out other secondary causes such as medications, infections, hormonal imbalances, abnormalities in conduction, and neurological conditions. In our case, we ruled out infection due to a lack of fever and source; neurological factors were ruled out by scans. However, there was an imbalance in thyroid hormone levels, suggested by blood reports showing high TSH and low T4, which could lead to significant cardiac dysfunction [1] and abnormalities in conduction, as shown by the 24-hour ambulatory ECG recording. In our case, we started levothyroxine 25 mcg with planned titration to avoid rapid cardiac stimulation or precipitation of myocardial ischemia [13], in consideration of the borderline systolic function, which showed gradual improvement in heart rate and blood pressure. Hypothyroidism is one of the rare etiologies for bradycardia that shows complete recovery with treatment [14]. Few cases have been reported which showed a favorable course with complete resolution of the atrioventricular conduction abnormality [15]. With the increase in heart rate, blood flow to the brain increases, leading to an increase cerebral perfusion, preventing a syncopal attack.
In this case, the diagnosis was delayed, as the life threatening presentation shifted the focus more so on ruling out the underlying structural, neurological, and cardiac abnormalities, which in itself is a fair approach; but we emphasize keeping broader differentials like hypothyroidism in context of persistent bradycardia, even in absence of classic systemic symptoms. The patient's bradycardia and orthostatic hypotension significantly improved after starting low dose thyroxine replacement, leading to the complete resolution of the symptoms.
Conclusions
This case emphasizes the importance of considering hypothyroidism in the differential diagnoses of persistent unexplained bradycardia and syncope, particularly in elderly patients. Early diagnosis and treatment with thyroid hormone replacement can lead to complete clinical recovery, preventing potential complications, including injury or fatal accidents. Going for thorough investigations is the right way to approach a syncopal or presyncope episode, but requesting a thyroid profile to rule out a potential cause of bradycardia saves time and extensive investigations, leading to quicker diagnosis and timely management of the patient. There are several cases of hypothyroidism leading to syncope or presyncope reported in the literature, signifying the need for conducting broader studies on investigating thyroid profiles in patients with bradycardia. We hope this case report will help healthcare professionals broaden their differential diagnoses before embarking on extensive investigations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Symptomatic junctional bradycardia due to untreated hypothyroidism after beta-blocker discontinuation: a case report Cureus Rahimi O Lee K Lei K Wahi-Gururaj S Gururaj AV 0152023 https://pmc.ncbi.nlm.nih.gov/articles/PMC 10353883/10.7759/cureus.40605 PMC 1035388337469810 · doi ↗ · pubmed ↗
- 2Thyroid hormones and cardiac arrhythmias Vascul Pharmacol Tribulova N Knezl V Shainberg A Seki S Soukup T 102112522010 https://doi.org/10.1016/j.vph.2009.10.0011985015210.1016/j.vph.2009.10.001 · doi ↗ · pubmed ↗
- 3Unusual presentations of hypothyroidism Am J Med Sci Westphal SA 3333373141997 https://www.sciencedirect.com/science/article/abs/pii/S 000296291540232010.1097/00000441-199711000-000119365336 · doi ↗ · pubmed ↗
- 4Complete atrioventricular block presenting with syncope caused by severe hypothyroidism Cardiol Res Seol SH Kim DI Park BM 23924132012 https://doi.org/10.4021/cr 221w 2834869510.4021/cr 221w PMC 5358139 · doi ↗ · pubmed ↗
- 5The Colorado thyroid disease prevalence study Arch Intern Med Canaris GJ Manowitz NR Mayor G Ridgway EC 52653416020001069569310.1001/archinte.160.4.526 · doi ↗ · pubmed ↗
- 6Sinus bradycardia Stat Pearls [Internet] Hafeez Y Grossman SA Treasure Island (FL)Stat Pearls Publishing 2023 https://www.ncbi.nlm.nih.gov/books/NBK 493201/
- 7A prospective observational study to evaluate cardiovascular changes in patients of hypothyroidism Cureus Sawarthia P Bhosle D Kalra R 015202310.7759/cureus.40201 PMC 1033104037435246 · doi ↗ · pubmed ↗
- 8Myocardial infarction and cardiac arrest in a patient With severe undiagnosed hypothyroidism during bronchoscopy J Cardiothorac Vasc Anesth Awari DW Dhanasekaran M Mudrakola HV Morales DJ Weingarten TN Sprung J 141014143620223371232710.1053/j.jvca.2021.02.025 · doi ↗ · pubmed ↗