Laparoscopic Drainage of a Gas-Forming Liver Abscess in a Hostile Abdomen: Surgical Feasibility Does Not Guarantee Survival
Amador Humberto Falconi Santiago, Michelle Cruz Méndez, Emilio Mondragón Rosas, Marian V Iniesta Vallejo, Andrea Navalón Calzada, Alfonso Sandoval, Daniela Vega Hernández, Yael G Concha Sampedro, María C Gaspar Verduzco, Luis M Canal de Velasco, José Emiliano González Flores

TL;DR
A complex liver abscess case in a patient with a hostile abdomen was treated laparoscopically, but the patient died despite successful drainage.
Contribution
Demonstrates laparoscopic drainage feasibility in hostile abdomens but highlights that survival depends on systemic stability.
Findings
Laparoscopic drainage was technically feasible in a complex, gas-forming liver abscess.
Technical success did not prevent mortality due to multiorgan failure in a systemically decompensated patient.
Early recognition of sepsis and individualized management are critical in such cases.
Abstract
A pyogenic liver abscess (PLA) is a potentially fatal intra-abdominal infection. Prognosis worsens when gas formation, multiloculated cavities, or multidrug-resistant organisms, such as extended-spectrum β-lactamase (ESBL)-producing Escherichia coli (E. coli), are involved. Management becomes more complex in patients with a “hostile abdomen,” characterized by extensive adhesions from prior surgeries or chronic inflammation. We report the case of a 54-year-old man with type 2 diabetes mellitus, a previous open appendectomy, and a history of viral hepatitis who presented with jaundice, right upper quadrant (RUQ) pain, and systemic inflammatory response. Imaging with computed tomography (CT) revealed a 13 cm gas-forming, multiloculated hepatic abscess. Despite anatomical complexity and clinical deterioration, laparoscopic drainage was achieved using an open Hasson technique with extensive…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
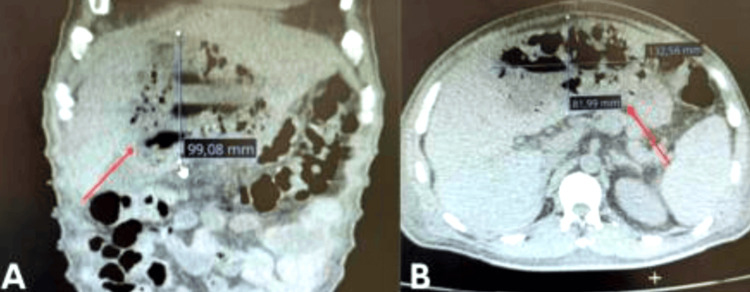 Figure 1
Figure 1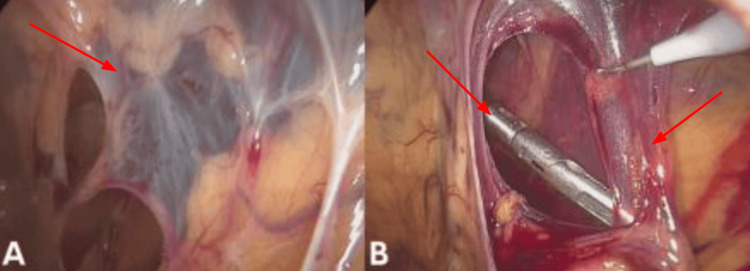 Figure 2
Figure 2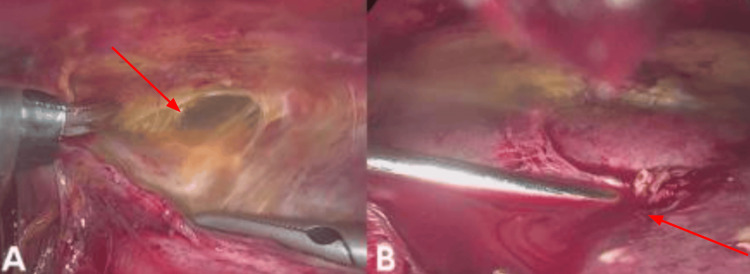 Figure 3
Figure 3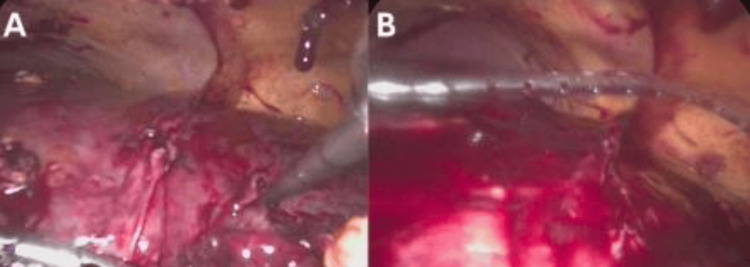 Figure 4
Figure 4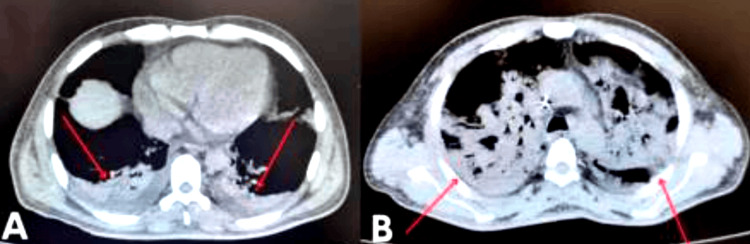 Figure 5
Figure 5| Parameter | Day 1 Values | Day 3 Value | Normal Range |
| TP (seconds) | 12.7 | 15.4 | 11–14 |
| INR | 1.15 | 1.4 | 0.8–1.2 |
| TTP (s) | 29.9 | 29.4 | 25–35 |
| LEU (×10³/µL) | 26.4 | 19.86 | 4.0–10.0 |
| NEU (%) | 83.5 | 90.69 | 40–70 |
| Hb (g/dL) | 10.2 | 8.23 | 13.5–17.5 |
| HTO (%) | 29.7 | 22.6 | 41–53 |
| PLAQ (×10³/µL) | 95.5 | 174.4 | 150–450 |
| GLU (mg/dL) | 144.3 | 186 | 70–110 |
| BUN (mg/dL) | 85.7 | Not analyzed | 7–25 |
| UREA (mg/dL) | 183 | Not analyzed | 15–50 |
| CREA (mg/dL) | 3.73 | 4.31 | 0.6–1.3 |
| Na (mmol/L) | 127.05 | 133.79 | 135–145 |
| K (mmol/L) | 4.3 | 3.26 | 3.5–5.1 |
| Cl (mmol/L) | 98.2 | 97 | 98–107 |
| Ca (mg/dL) | 6.88 | 0.92 | 8.6–10.2 |
| Mg (mg/dL) | 2.11 | 2.13 | 1.6–2.6 |
| FO (mg/dL) | 5.94 | 5.89 | 2.5–4.5 |
| AU (mg/dL) | 8.2 | Not analyzed | 2.5–7 |
| COL (mg/dL) | 296 | Not analyzed | <200 |
| TGL (mg/dL) | 301 | Not analyzed | <150 |
| Parameter | Day 1 Values | Day 3 Values | Normal Range |
| BT (mg/dL) | 12.4 | 7.79 | 0.1–1.2 |
| BD (mg/dL) | 7.89 | 4.75 | 0–0.3 |
| BI (mg/dL) | 4.6 | 3 | 0.2–1.2 |
| PT (g/dL) | 4.27 | Not analyzed | 6.0–8.3 |
| AST (U/L) | 188 | Not analyzed | 10–40 |
| ALT (U/L) | 292 | Not analyzed | 10–40 |
| FA (U/L) | 783 | Not analyzed | 30–120 |
| GGT (U/L) | 440 | Not analyzed | 10–60 |
| DHL (U/L) | 434 | Not analyzed | 100–190 |
| AMIL (U/L) | 9.65 | Not analyzed | 28–100 |
| LIP (U/L) | 5.43 | Not analyzed | <300 |
| PCR (mg/dL) | 19.8 | Not analyzed | <0.5 |
| pH | Not analyzed | 7.5 | 7.35–7.45 |
| PCO₂ (mmHg) | Not analyzed | 26 | 35–45 |
| PO₂ (mmHg) | Not analyzed | 41 | 80–100 |
| Lactate (mmol/L) | Not analyzed | 1.9 | 0.5–2.2 |
| HCO₃⁻ (mmol/L) | Not analyzed | 20.3 | 22–26 |
| HGB (g/dL) | Not analyzed | 8.23 | 13.5–17.5 |
| MCV (fL) | Not analyzed | 87.7 | 80–100 |
| PLT (×10³/µL) | Not analyzed | 174.4 | 150–450 |
| BNP (pg/mL) | Not analyzed | 824 | <100 |
| Source | Diagnostic Method | Sensitivity | Specificity | Indications | Limitations | Level of Evidence |
| Mexican Institute of Social Security (IMSS) [ | Abdominal ultrasound (US) | ~70–80% | ~85% | Initial study in suspected cases due to accessibility and speed | Reduced sensitivity in obese patients or with intestinal gas | Level V |
| Wang et al. [ | Computed tomography scan (CT) | ~90–97% | ~95% | Assessment of multiloculated or gas-forming abscesses and to define the extent | High cost, contrast requirement, and radiation exposure | Level III |
| Mexican Institute of Social Security (IMSS) [ | Magnetic resonance imaging (MRI) | ~75-90% | ~90–95% | Cases with a poor ultrasound window or unresolved diagnostic uncertainty | Limited availability and high cost | Level V |
| Curran et al. [ | Culture and blood culture | <50% positive | — | Microbiological identification of the causative pathogen | False negatives in patients already on antibiotics | Level I-II |
| Author | Clinical presentation (history) | Comorbidities | Diagnostic method | Antibiotic therapy | Culture result | Surgical treatment | Postoperative complications | Follow-up | Level of evidence |
| Li et al., 2021 [ | Adolescent with T2DM, high fever, RUQ pain, altered mental state | T2DM | CT, USG, culture | Cefalosporins + carbapenem | Hypervirulent | Surgical drainage + intensive support | Multiorgan failure, death | Death in ICU | IV – Case report |
| Paramythiotis et al., 2023 [ | Complicated acute cholecystitis with hepatic abscess | HTN | USG, CT | Broad-spectrum empirical + adjustment | Polymicrobial | Percutaneous drainage | Resolved without complications | Outpatient follow-up without relapse | IV – Case report |
| Kokayi et al., 2023 [ | Perforated appendicitis progressing to PLA and septic shock | None reported | CT | Ampicillin/sulbactam + metronidazole | No growth | Surgical drainage | Persistent sepsis | Discharged with antibiotics | IV – Case report |
| Wu et al., 2023 [ | Gas-forming hepatic abscess with prolonged fever | None reported | Contrast-enhanced CT | Meropenem | Klebsiella pneumoniae | Surgical drainage | None reported | Complete resolution | IV – Case report |
| Malla et al., 2023 [ | Hepatic abscess complicated by hepatoduodenal fistula | None reported | CT, endoscopy | Ampicillin + aminoglycoside | Negative | Drainage + fistula repair | Postoperative biliary stenosis | Successful surgical follow-up | IV – Case report |
| Lin et al., 2021 [ | History of prior biliary surgery | Postoperative biliary disease | CT, USG | Cefalosporins | Enterobacteriaceae predominant | Percutaneous drainage in selected cases | Not reported | Imaging follow-up without recurrence | III – Retrospective study |
| Nie et al, 2021 [ | Fever, abdominal pain, jaundice; multiple comorbidities | T2DM, chronic liver disease | USG, CT, labs | Carbapenem + metronidazole |
| Percutaneous + surgical drainage | Recurrent abscesses | Follow-up by labs and imaging | III – Retrospective study |
| Yin et al., 2022 [ | Fever, RUQ pain, sepsis; large multiloculated abscess | T2DM, advanced age | CT, USG, culture | Prolonged IV empirical therapy | Klebsiella pneumoniae | Surgical drainage | Prolonged hospitalization | Complete recovery | III – Retrospective study |
| Liu et al., 2021 [ | Post ERCP with PLA development | Cholangiopathy | CT post-ERCP | Ampicillin/sulbactam | E. coli | Percutaneous drainage | Mild recurrence | Resolution in short-term follow-up | IV – Case series post-ERCP |
| Alasso et al., 2023 [ | PLA with secondary biliary fistula | None reported | CT, fistulography | Ceftriaxone + metronidazole | Polymicrobial | Laparoscopy + biliary drainage | Total clinical improvement | Biliary drainage control | IV – Case report |
| Meister et al., 2023 [ | Abscess without apparent cause, malignancy ruled out | None reported | CT + exploratory laparoscopy | Broad empirical + adjustment | Negative | Surgical exploration + drainage | Neoplasia ruled out | Prolonged follow-up without recurrence | IV – Case report |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAmoebic Infections and Treatments · Gallbladder and Bile Duct Disorders · Liver Disease and Transplantation
Introduction
Pyogenic liver abscess (PLA) is a serious infectious condition characterized by the accumulation of purulent material within the hepatic parenchyma, usually due to a bacterial infection. Although typically polymicrobial, recent years have seen an increasing predominance of Gram-negative organisms such as Klebsiella pneumoniae (K. pneumoniae) and extended-spectrum β-lactamase (ESBL)-producing *Escherichia coli *(E. coli) [1-3]. The incidence of PLA has risen, not only due to a higher prevalence of predisposing comorbidities but also because of advances in imaging techniques and broader access to healthcare services [4-6]. PLA risk factors are diverse, ranging from local to systemic causes. These include diabetes mellitus, biliary tract disease, immunosuppression, abdominal surgeries, complicated appendicitis, acute cholecystitis, and biliary manipulation via endoscopic retrograde cholangiopancreatography (ERCP) [7,8]. In Asian populations, K. pneumoniae is disproportionately prevalent, while in Western countries, E. coli and mixed flora remain the most common pathogens [5,6].
When prior intra-abdominal inflammation is present, surgical patients may develop what is referred to as a “hostile abdomen.” This term describes dense intra-abdominal adhesions, loss of normal anatomical planes, or reactive fibrosis due to previous surgeries, infections, or chronic inflammatory conditions [9-11]. Such anatomical complexity increases the risk of surgical complications, limits minimally invasive approaches, and may worsen patient outcomes. Consequently, diagnosis in these patients becomes particularly challenging, as the hostile abdomen represents a critical complicating factor.
Clinically, PLA often presents with nonspecific symptoms such as fever, right upper quadrant (RUQ) pain, jaundice, malaise, and altered liver function tests, which can delay early diagnosis [12,13]. Imaging studies are essential and include abdominal ultrasound, contrast-enhanced computed tomography (CT), and occasionally magnetic resonance imaging (MRI). Among these, CT is the most sensitive and specific modality for characterizing size, location, gas formation, and abscess complexity [14-18].
The clinical course of PLA can be complicated by sepsis, a life-threatening condition caused by a dysregulated host response to infection [11]. Early recognition and risk stratification are essential to improve outcomes. The Sequential Organ Failure Assessment (SOFA) score and its simplified version, quick SOFA (qSOFA), help objectively estimate the extent of organ dysfunction and predict hospital mortality [19-21]. A SOFA score ≥2 is associated with a worse prognosis and warrants immediate intervention [21].
This article presents a case of gas-forming, multiloculated PLA in a patient with a complex surgical history, managed laparoscopically. We analyze the clinical evolution, complications, and outcome, and compare this case with recent literature on prognostic factors, therapeutic strategies, and current management recommendations.
Case presentation
A 54-year-old male patient with a medical history of type 2 diabetes mellitus managed with metformin, remote viral hepatitis of unknown type, 20 years of chronic distilled and fermented alcohol consumption, and tobacco use with a smoking index of 1.25 presented to the emergency department with a 15-day history of RUQ abdominal pain, progressive generalized jaundice, acholia, choluria, persistent fever up to 39°C, and intolerance to oral intake. His surgical history was notable for an open appendectomy via supra- and infraumbilical laparotomy in 2000, complicated by wound dehiscence. He also reported a history of rheumatic fever without prolonged treatment and had received five units of platelet concentrates days before admission due to thrombocytopenia (53,000/mm³), all the laboratory values on Table 1 and Table 2. He denied a history of drug abuse or recent trauma.
On physical examination, the patient was febrile (38.5°C), with marked mucocutaneous jaundice (+++/+++). Cardiopulmonary findings were unremarkable. The abdomen was soft but distended, with deep tenderness in the epigastric region, mesogastrium, and right hypochondrium. Hepatomegaly was palpable (3-4 cm below the costal margin), with an indurated and voluminous mass extending across the midline. No signs of peritoneal irritation were present. Bowel sounds were normoactive. The extremities showed a mild reduction in strength but preserved sensitivity and distal pulses. Abdominal examination revealed negative Murphy’s sign, McBurney’s point tenderness, Rovsing’s sign, and Blumberg’s sign.
Given the patient’s clinical deterioration, the presence of a large indurated mass, and imaging findings consistent with a multiloculated gas-forming abscess, a decision was made to proceed with surgical drainage as the most appropriate therapeutic approach.
Initial management focused on stabilizing the patient and addressing the infectious process. A diagnosis of pyogenic liver abscess was established based on clinical findings, laboratory evidence of severe infection and cholestasis, and abdominal imaging demonstrating a multiloculated gas-forming lesion consistent with a hepatic abscess. Empirical broad-spectrum antibiotic therapy with piperacillin-tazobactam (4.5 g every six hours) and metronidazole (500 mg every eight hours) was initiated promptly after blood cultures were obtained. Despite medical therapy, the patient’s clinical condition progressively deteriorated, with persistent fever, worsening laboratory markers, and increased abdominal tenderness.
Given the severity of the case and progressive deterioration, a diagnostic laparoscopy was performed using an open Hasson technique. Intraoperatively, the patient was found to have a hostile abdomen with dense adhesions classified as Mazuji grade 3, Stülke grade II-III, and Björck 2B. Through careful, blunt, and sharp dissection with diathermy, access to the upper abdominal quadrants was achieved. Two 5 mm trocars were placed, and a multiloculated abscess in hepatic segment IVB and between segments II/III was successfully drained, yielding 300 cc of frank pus. After lavage, a quarter-inch Drenovac was placed and exteriorized through the right flank (Figures 1-4). The patient was transferred to the intensive care unit (ICU), intubated, and supported with vasopressors. Postoperatively, empirical broad-spectrum antibiotic therapy was continued with piperacillin-tazobactam (4.5 g every six hours) combined with metronidazole (500 mg every eight hours) to ensure adequate coverage against Gram-negative, anaerobic, and enteric pathogens commonly associated with pyogenic liver abscess. Blood and pus cultures were obtained; however, no growth was reported during the hospital stay. Consequently, antibiotic therapy remained empirical throughout the treatment course. Clinical improvement was noted within the first 72 hours, with resolution of fever, hemodynamic stabilization, and progressive normalization of inflammatory markers.
Contrast-enhanced abdominal computed tomography in coronal (A) and axial (B) views showing a multiloculated, gas-forming liver abscess, with a maximum diameter of 13.2 × 9.9 × 8.1 cm. Red arrows indicate the main cavity of the abscess. This finding is consistent with complicated abscesses that require surgical intervention, as in the reported case.
Laparoscopic approach in a patient with a hostile abdomen(A) Sealed cavity with dense adhesions between the omentum (arrow) and abdominal wall (arrow); (B) Initial dissection using diathermy (arrow) with progressive access to the upper quadrants and hepatoparietal adhesions (arrow).
Laparoscopic maneuvers in a patient with a complicated liver abscess(A) Blunt dissection of hepatoparietal adhesions (arrow) using laparoscopic forceps, allowing safe access to the left hepatic lobe; (B) Direct puncture of the liver abscess (arrow) with aspiration of frank purulent material for microbiological analysis. These maneuvers confirmed the abscess location and facilitated controlled drainage.
Final stages of laparoscopic management in a multiloculated liver abscess(A) Active drainage of the abscess in segments II/III via direct aspiration (arrow); a previously drained cavity is visible in segment IV; (B) Placement of a Drenovac-type drainage system through the right flank (arrow), allowing postoperative control of residual secretions. These maneuvers ensured evacuation of purulent content and reduction of intra-abdominal pressure in the context of a hostile abdomen.
Within 48 hours, the patient showed partial clinical and biochemical improvement and was successfully extubated without further vasopressor requirement. However, three days later, he developed acute pulmonary failure requiring reintubation and died within 24 hours due to respiratory failure (Figure 5). Despite partial hepatic recovery and a technically successful laparoscopic drainage under challenging conditions, the patient’s clinical course was ultimately fatal due to complications extrinsic to the procedure itself.
Axial slice from non-contrast computed tomography showing bilateral pulmonary complications(A) Basal consolidation secondary to an abdominal infectious process, and (B) partial pulmonary collapse associated with respiratory compromise. These findings were indicative of progression toward respiratory failure in the context of sepsis due to a liver abscess.
Discussion
Etiology and risk factors in context
PLAs are focal collections of pus within the hepatic parenchyma, most commonly caused by bacterial infections. The predominant pathogens include K. pneumoniae and* E. coli*, with an increasing proportion of multidrug-resistant strains, such as ESBL-producing E. coli [1,2]. These strains are associated with diminished antibiotic responsiveness, prolonged hospitalization, and higher morbidity and mortality rates [3]. In our patient, the identification of an ESBL-producing strain significantly complicated empirical management.
Although PLA incidence remains highest in East Asia, global rates have increased due to greater access to advanced imaging, especially CT, and improved survival in patients with chronic illnesses such as diabetes mellitus and immunosuppression (4). Alkomos et al. (2023) noted a progressive rise in cases that parallels demographic aging and the growing burden of comorbidities [4].
Among recognized risk factors, diabetes mellitus is particularly significant. It impairs neutrophil function, alters intestinal permeability, and facilitates bacterial translocation via the portal venous system [6]. Immunosuppression and prior abdominal surgeries, such as our patient’s complicated appendectomy, disrupt anatomical barriers, further predisposing to hepatic abscess formation [9,22]. In this context, the combination of diabetes, chronic liver disease, prior intra-abdominal surgery, and infection by a multidrug-resistant organism placed our patient in a high-risk category for poor outcomes.
Several studies have identified prognostic factors associated with adverse PLA outcomes, including advanced age, multiloculated or gas-forming abscesses, and infections by resistant pathogens [2,7,8]. Gas-forming abscesses, often caused by K. pneumoniae or ESBL-producing E. coli, are especially aggressive and associated with higher rates of tissue necrosis, septic shock, and mortality, reaching up to 30% in some cohorts [12].
Diagnostic and prognostic challenges
The clinical presentation of PLA is frequently nonspecific. The classic Charcot triad, fever, right upper quadrant pain, and jaundice, is observed in less than half of all cases [13]. Our patient exhibited all three, along with hepatomegaly, thrombocytopenia, elevated liver enzymes, and renal dysfunction, features commonly associated with severe disease [14]. In a retrospective cohort of 104 patients, Wang et al. (2023) found fever in 85%, localized abdominal pain in 65%, and jaundice in 42% [11]. The full Charcot triad is known to significantly increase the risk of septic complications, especially in diabetic or immunocompromised patients [5].
Imaging is essential for diagnosis and management planning. Although abdominal ultrasound is often the first-line modality due to its availability, its sensitivity is limited for small, deep, or multiloculated abscesses [15]. Contrast-enhanced CT is the diagnostic gold standard, offering superior detection of abscess size, gas content, loculations, and anatomical extent [11,16,17]. In our patient, CT revealed a 13 cm gas-forming, multiloculated abscess spanning multiple hepatic segments, necessitating urgent drainage.
Microbiological confirmation is often delayed. Blood cultures are positive in fewer than 50% of cases, and aspirated pus may remain sterile, particularly after the initiation of broad-spectrum antibiotics [19]. While our patient’s initial cultures were negative, subsequent identification confirmed the presence of an ESBL-producing E. coli. Notably, K. pneumoniae, especially hypervirulent K1/K2 serotypes, remains the most commonly isolated organism in gas-forming PLA and has been associated with metastatic complications such as endogenous endophthalmitis [20].
Therapeutic strategies and the role of laparoscopy
The combination of type 2 diabetes and multidrug-resistant infection substantially reduces the efficacy of empirical therapy, requiring broader-spectrum agents and often prolonged courses. Li et al. (2023) reported a rapidly fatal case in a diabetic patient infected with ESBL-producing K. pneumoniae, reinforcing the importance of early pathogen identification in high-risk populations [12]. Standard management of PLA involves both antimicrobial therapy and abscess drainage. Empirical regimens typically consist of third-generation cephalosporins or carbapenems, often combined with metronidazole to ensure coverage of both aerobic and anaerobic organisms [15]. In complicated cases, such as those involving gas formation, multiloculation, or suboptimal response, treatment may require up to six weeks of antibiotics [7,17,23]. Infections caused by resistant organisms must be treated based on susceptibility profiles to ensure efficacy (Tables 3, 4) [3].
Drainage is generally indicated for abscesses >3-5 cm, particularly when they are gas-forming or structurally complex. Image-guided percutaneous drainage (PD) is preferred for uniloculated abscesses due to its minimal invasiveness and success rates of 70%-90% [18,27]. However, PD may be inadequate in the presence of thick, septated fluid or when anatomical barriers compromise catheter placement. Surgical drainage is therefore necessary in select scenarios [28].
The Mexican Clinical Practice Guidelines recommend surgical drainage when abscesses exceed 5 cm, PD fails, or contraindications exist [29]. Laparoscopic drainage provides the benefits of surgical access with reduced morbidity, including shorter recovery, decreased postoperative pain, and fewer wound complications compared to open procedures [30]. A “hostile abdomen”, defined by dense adhesions due to prior surgery or inflammation, traditionally poses a challenge for laparoscopy. Nonetheless, recent evidence supports its feasibility when performed by experienced teams, even in complex anatomical settings [11,24]. In this case, laparoscopy was initiated using an open Hasson technique, followed by meticulous adhesiolysis. Approximately 300 mL of purulent material was drained from hepatic segments II/III and IVB. Although initial improvement was noted, evidenced by normalized bilirubin and leukocytes, the patient subsequently developed respiratory failure and succumbed to multiorgan dysfunction on postoperative day four. This clinical course underscores the limits of surgical success in the context of systemic decompensation.
The SOFA score is a validated tool for estimating mortality risk in patients with sepsis. Organ dysfunction involving the respiratory, renal, or hematologic systems is particularly predictive of poor outcomes. A SOFA score ≥2 has been associated with higher in-hospital mortality, depending on the degree of organ dysfunction [21,23]. In our patient, the presence of respiratory failure (PaO₂ < 80 mmHg), acute kidney injury (creatinine > 3 mg/dL), thrombocytopenia (<100,000/µL), and the need for vasopressors resulted in an estimated SOFA score of approximately 9, indicating a high risk of mortality from the time of admission. This finding underscores the patient’s severe baseline condition and helps explain the unfavorable outcome despite timely surgical management.
This case highlights several key considerations: early identification of high-risk features in PLA is essential; laparoscopy is a viable and safe option even in anatomically complex or post-surgical cases; and systemic conditions, such as sepsis and organ dysfunction, often dictate the outcome more than technical procedural success. Further studies are warranted to refine prognostic stratification tools and to establish evidence-based criteria for early surgical intervention in high-risk PLA patients.
Conclusions
This case underscores the complex interplay between host comorbidities, microbial resistance, and surgical challenges in the management of pyogenic liver abscesses. Despite technically successful laparoscopic drainage performed under hostile anatomical conditions, the patient's outcome was ultimately dictated by systemic deterioration and delayed recognition of multiorgan dysfunction. Multiloculated, gas-forming abscesses caused by ESBL-producing pathogens represent a particularly aggressive subset of PLA, often requiring tailored antimicrobial regimens and timely intervention. Clinicians must maintain a high index of suspicion for early decompensation, even in the presence of apparent surgical success. Future efforts should focus on the strict application of existing risk stratification tools, such as the SOFA score, and the implementation of early, aggressive multidisciplinary intervention strategies to improve outcomes in high-risk, surgically complex PLA presentations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clinical features and risk factors for pyogenic liver abscess caused by multidrug-resistant organisms: a retrospective study Virulence Long Q Zhao X Chen C Hao M Qin X 23566801520243876756210.1080/21505594.2024.2356680 PMC 11110708 · doi ↗ · pubmed ↗
- 2Clinical characteristics and management of 1572 patients with pyogenic liver abscess: a 12-year retrospective study Liver Int Yin D Ji C Zhang S 8108184120213331453110.1111/liv.14760 PMC 8048845 · doi ↗ · pubmed ↗
- 3Clinical characteristics and management of 106 patients with pyogenic liver abscess in a traditional Chinese hospital Front Surg Nie S Lin D Li X 1041746920223668435810.3389/fsurg.2022.1041746 PMC 9852512 · doi ↗ · pubmed ↗
- 4Epidemiological, clinical, microbiological, and risk factors of pyogenic liver abscess: an 18-years retrospective single-center analysis J Community Hosp Intern Med Perspect Alkomos MF Estifan E Melki G Adib S Baddoura W 42451120213355241310.1080/20009666.2020.1831745 PMC 7850341 · doi ↗ · pubmed ↗
- 5Epidemiology, clinical features, and outcome of liver abscess: a single-center experience Cureus Sahu V Pipal DK Singh Y 014202210.7759/cureus.29812 PMC 962147036337811 · doi ↗ · pubmed ↗
- 6Clinical management, pathogen spectrum and outcomes in patients with pyogenic liver abscess in a German tertiary-care hospital Sci Rep Wendt S Bačák M Petroff D 129721420243883998010.1038/s 41598-024-63819-w PMC 11153614 · doi ↗ · pubmed ↗
- 7Septic shock secondary to a pyogenic liver abscess following complicated appendicitis Cureus Kokayi A Jr 013202110.7759/cureus.18359 PMC 855337834725610 · doi ↗ · pubmed ↗
- 8Pyogenic liver abscess following perforated appendicitis Rev Soc Bras Med Trop Akyüz B 055202210.1590/0037-8682-0244-2022 PMC 953680536197379 · doi ↗ · pubmed ↗