Factors influencing health-promoting lifestyles in young and middle-aged adults with metabolic risk factors: a network analysis
Qun Wang, Sek Ying Chair, Weixiang Luo, Siyi Zhong, Zehao Huang

TL;DR
This study identifies key factors like self-efficacy and knowledge that influence healthy lifestyles in adults with metabolic risks, suggesting these should be targeted in interventions.
Contribution
The study introduces a network analysis approach to identify self-efficacy for psychological well-being as a central factor in promoting healthy lifestyles.
Findings
Self-efficacy and knowledge are strong predictors of dietary behaviors in adults with metabolic risk factors.
Self-efficacy for psychological well-being is a central factor influencing health-promoting lifestyles.
Depression and social support significantly impact stress management behaviors.
Abstract
Metabolic dysfunction is prevalent among young and middle-aged adults and impairs their health. Adopting healthy lifestyles is essential for preventing and managing these issues. By determining modifiable factors that influence health-promoting lifestyles, we can gain valuable insights for developing targeted lifestyle interventions. Therefore, this study aims to identify factors contributing to health-promoting lifestyles among young and middle-aged adults with metabolic risk factors. A cross-sectional study design was adopted. Data were obtained from 402 young and middle-aged adults with metabolic risk factors, recruited via convenience sampling from community health centers in China between October 2022 and April 2024. All participants were measured for knowledge (MetS Knowledge Scale), self-efficacy (Self-Rated Abilities for Health Practices Scale), social support (Social Support…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
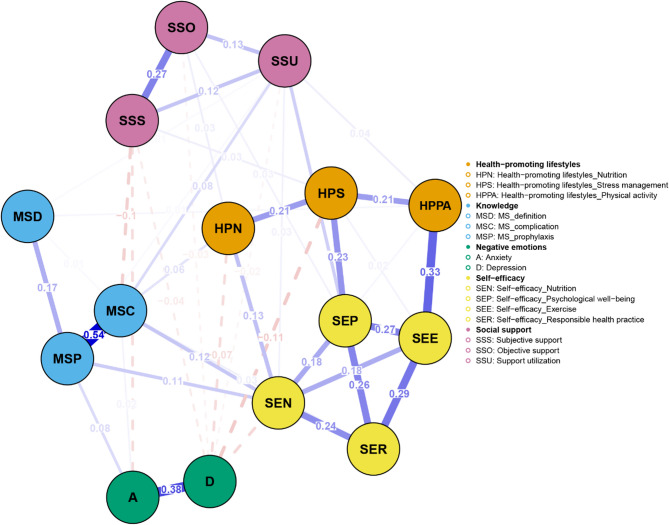 Figure 1
Figure 1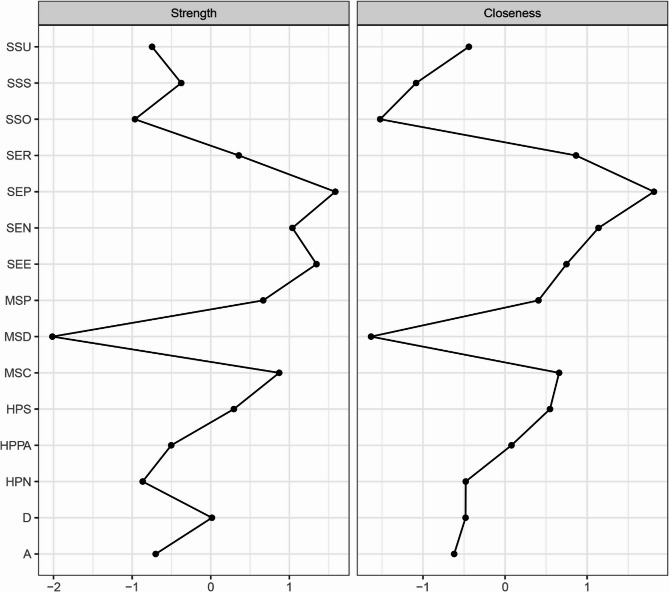 Figure 2
Figure 2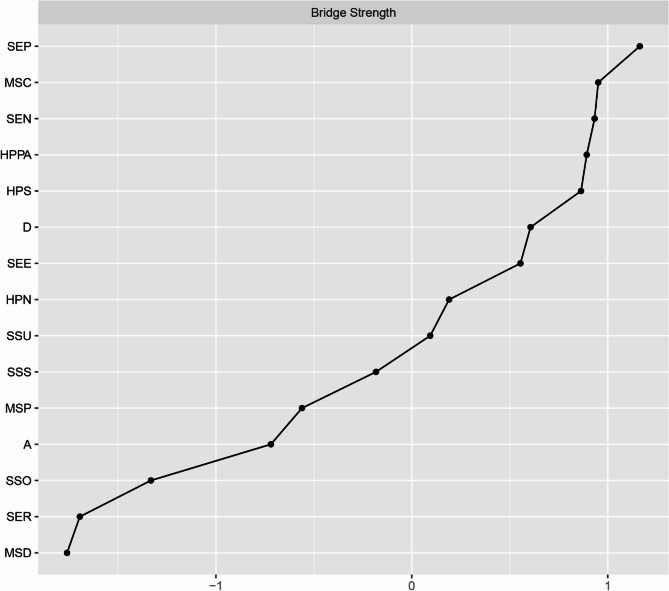 Figure 3
Figure 3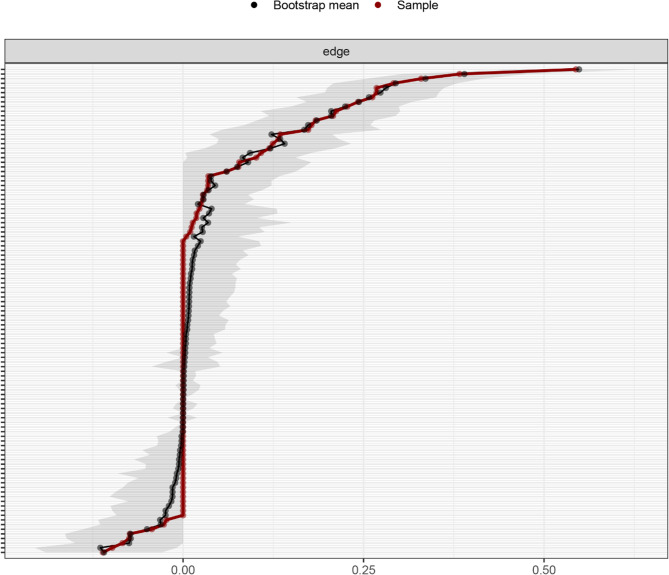 Figure 4
Figure 4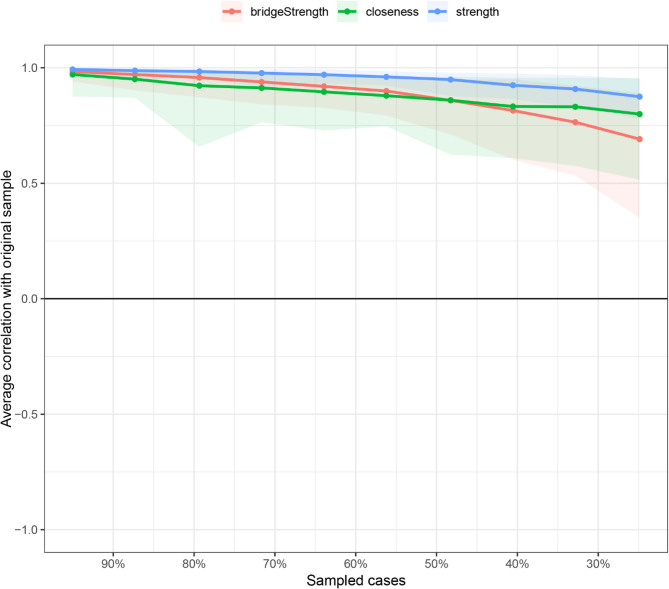 Figure 5
Figure 5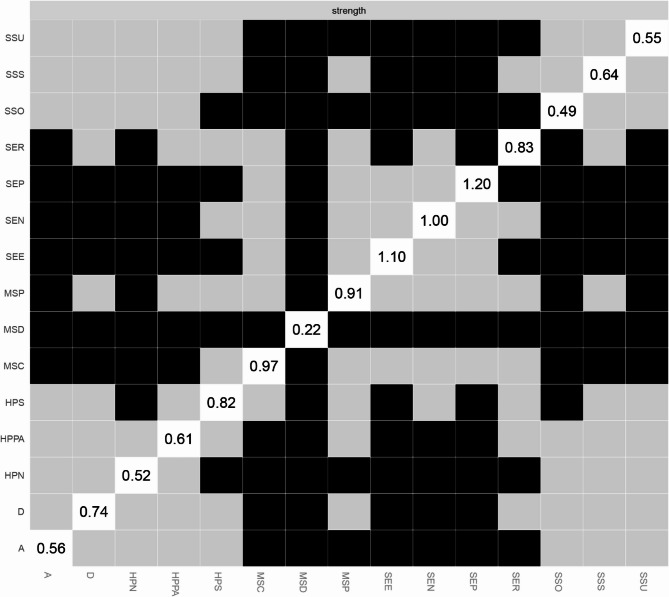 Figure 6
Figure 6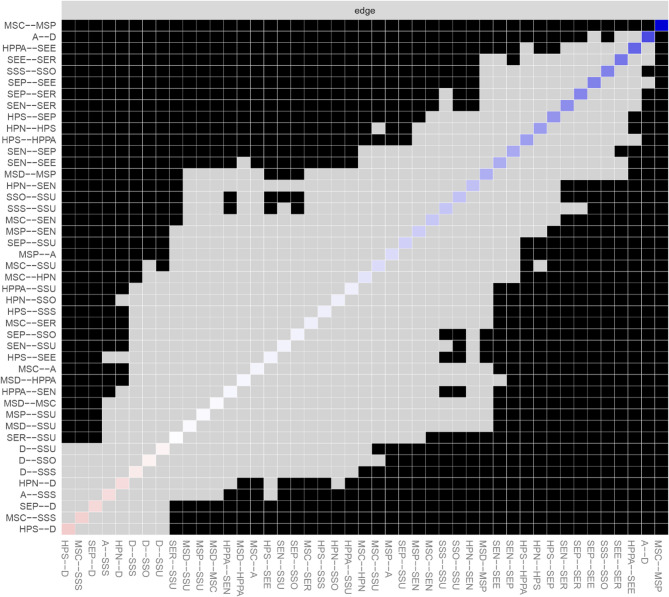 Figure 7
Figure 7- —China's National Natural Science Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealth and Wellbeing Research · Mental Health Research Topics · Health disparities and outcomes
Introduction
Metabolic dysfunction contributes to the onset of various chronic diseases, including chronic kidney disease, diabetes, and heart disease, and leads to increased mortality rates [1–5]. It was reported that common metabolic risk factors such as abdominal obesity, high blood glucose, dyslipidemia, and hypertension account for more than a quarter of global disability-adjusted life years [5, 6]. Importantly, recent studies have revealed a conspicuous global burden of these risk factors among younger populations [7, 8]. It has been reported that the prevalence of metabolically unhealthy obesity among young and middle-aged adults in China is 3.07% and 5.6%, respectively [9]. Weight gain during young and middle adulthood significantly increases the risk of major chronic diseases and reduces the likelihood of healthy aging [10]. Recent data indicates that the prevalence of hypertension in China has increased to 12.8% among young adults and 37.4% in middle-aged group [11]. The prevalence of total diabetes is 3.1% for young Chinese adults and 8.7% for middle-aged individuals [12]. A systematic review reported a pool prevalence of dyslipidemia of 40.1% in young adults and 45.2% among middle-aged adults in China [13]. Lifestyle interventions are crucial for preventing and managing these risk factors [14, 15], focusing primarily on balanced nutrition, regular physical activity, and stress management [14]. Therefore, to develop effective lifestyle interventions for young and middle-aged adults with metabolic risk factors, it is essential to determine the modifiable predictors of health-promoting lifestyles.
Our previous research revealed that patients with metabolic risk factors often lacked sufficient knowledge about the diagnosis and complications of metabolic syndrome, as well as information on how to prevent it [16]. Addressing these issues may facilitate better adoption of health-promoting lifestyles among young and middle-aged adults with metabolic risk factors [17, 18]. Self-efficacy in executing health behaviors is one of the essential predictors of health-promoting lifestyles [19]. A prior investigation demonstrated that enhancing self-efficacy contributes to improved daily physical activity and eating behaviors among adults with or at high risk of metabolic syndrome, while evidence of its impact on stress management is scarce [19]. Moreover, social support serves as an important element in promoting healthy lifestyles [20], with research indicating that providing support has a direct effect on healthy eating in patients with metabolic syndrome [18]. However, evidence for its impact on other health-promoting behaviors in this population is limited. Adults with metabolic risk factors such as hyperglycemia and increased triglycerides, as well as decreased high-density lipoprotein, have a higher risk of developing depression and anxiety [21]. Depression is significantly negatively associated with stress management in adults with metabolic syndrome, while evidence regarding its relationship with physical activity and dietary behaviors remains inconclusive [22]. Anxiety may correlate with health-promoting lifestyles in this clinical cohort; however, current evidence is sparse [23]. Due to the insufficient evidence on the predictors of health-promoting lifestyles among young and middle-aged adults with metabolic risk factors, further investigation is necessary.
Traditional methods, such as regression analysis, are limited in their ability to elucidate the interrelationships between multiple variables. Network analysis allows for the estimation of complex patterns of relationships, and examining the network structure can uncover its core characteristics, offering valuable insights for developing targeted lifestyle interventions [24]. Therefore, this study aimed to explore the predictors of health-promoting lifestyles among young and middle-aged adults with metabolic risk factors using both regression and network analysis.
Methods
Study design and participants
This was a cross-sectional study conducted in Shenzhen, China, from October 2022 to April 2024. The Strengthening of Reporting of Observational Studies in Epidemiology checklist for cross-sectional studies was followed [25]. We consecutively enrolled young and middle-aged adults with metabolic risk factors using convenience sampling. The inclusion criteria were as follows: (1) the presence of at least one metabolic syndrome risk factor (central obesity, elevated triglycerides, reduced high-density lipoprotein cholesterol, elevated blood pressure, and hyperglycemia); (2) age between 18 and 59; (3) ability to communicate in Chinese; (4) ability to complete the questionnaires; (5) ability to provide written consent. Patients were excluded if they met any of the following criteria: (1) a diagnosis of diabetes, coronary heart disease, or stroke; (2) clinical diagnoses of psychiatric disorders; or (3) pregnancy or breastfeeding. To achieve sufficient statistical power, a minimum sample size of 250 to 350 participants is needed if the network consists of 20 nodes or fewer [26]. In this study, data from 402 valid questionnaires were used.
Data collection and outcome measures
Data collection was conducted in six community health centers (CHC) in the Baoan, Nanshan, and Longhua districts of Shenzhen. Online and offline posters were distributed by the healthcare professionals of six CHCs. Those who responded to the invitation were screened by the research team. An introduction letter with the study objectives and procedures was given to potential participants. After receiving the written informed consent, the research team scheduled time for data collection. Trained investigators administered data collection in the CHC. The participants were recommended to complete the questionnaires by themselves. The trained investigators also assisted if necessary. The Chinese versions of the instruments have been validated.
Knowledge
The knowledge of MetS was evaluated using the 10-item MetS Knowledge Scale, which includes three domains, namely definition and diagnosis of MetS (five items), complications of MetS (two items), and prevention of MetS (three items). Each item was scored as 10 for a correct response and 0 for an incorrect response or “do not know”. The total score, calculated as the sum of all item scores, ranges from 0 to 100, with higher scores implying a greater understanding of metabolic syndrome [16, 27]. The Cronbach’s α for this study was 0.716.
Self-efficacy
The 28-item Self-Rated Abilities for Health Practices Scale was adopted to assess self-efficacy. It contains four subscales (seven items each): exercise, nutrition, responsible health practice, and psychological well-being. Each item was rated on a 5-point Likert scale, ranging from 0 (not at all) to 4 (completely). Total score is the sum of all item scores, ranging from 0 to 112, with higher scores reflecting greater self-efficacy in health practices [28, 29]. The Cronbach’s α for this study was 0.950.
Social support
The 10-item Social Support Rating Scale was used to measure social support. The scale consists of three domains: objective support (three items), subjective support (four items), and support utilization (three items). The items on the scale include single-choice (a 4-point Likert scale) and multiple-choice options. Total score is the sum of all item scores, with higher scores indicating higher levels of social support [30]. The Cronbach’s α for this study was 0.617.
Depression
The 7-item Hospital Anxiety and Depression Scale-Depression was employed to assess depression. A 4-point Likert scale was used for scoring each item, ranging from 0 to 3. Total scores are the sum of all item scores, ranging from 0 to 21, with higher scores suggesting higher levels of depression [31]. The Cronbach’s α for this study was 0.662.
Anxiety
The 7-item Hospital Anxiety and Depression Scale-Anxiety was used to evaluate anxiety. A 4-point Likert scale was used for scoring each item, ranging from 0 to 3. Total scores are the sum of all item scores, ranging from 0 to 21, with higher scores suggesting higher levels of anxiety [31]. The Cronbach’s α for this study was 0.774.
Health-promoting lifestyles
Three subscales of Health-Promoting Lifestyle Profile II, including nutrition (9 items), physical activity (8 items), and stress management (8 items), were adopted to measure the practice of health-promoting lifestyles. Participants rated on a four-point Likert scale, ranging from 1 (never) to 4 (routinely). The total scores for each subscale were calculated as the means of the responses to all items within that subscale. A higher score indicates better performance in health-promoting lifestyles [17, 32]. The Cronbach’s α for this study was 0.836.
Sociodemographic information
The sociodemographic information includes age, gender, marital status, employment status, educational level, monthly income, and smoking and drinking history.
Data analysis
The statistical analyses were conducted using IBM SPSS version 27.0. A two-sided p < 0.05 is considered statistically significant. The statistical assumption of the normality of continuous variables was examined by quantile-quantile plots and skewness and kurtosis statistics [33]. Normally distributed continuous variables were presented in means and standard deviation (SDs). All the categorical variables were presented as frequency and percentage. Independent t-tests, one-way analysis of variance, or Pearson’s correlation analysis were used to identify potential predictors of health-promoting lifestyles. Hierarchical linear regression analyses were executed to test the relationships between study variables and health-promoting lifestyles while controlling significant sociodemographic variables that correlated with health-promoting lifestyles. We assessed multicollinearity using tolerance and variance inflation factors (VIF), with acceptable criteria set at a tolerance greater than 0.1 and a VIF less than 10 [34].
Network analysis was performed using RStudio 2025.05.0 + 496 to analyze the relationships between the study variables. The network was estimated using the Gaussian Graphical Model with the EBICglasso algorithm and visualized with the “qgraph” package. In the network, nodes represent study variables or their domains, while edges denote the links between the nodes. The thickness of each edge indicates the strength of the relationship, with blue representing positive relationships and red indicating negative correlations. To identify core nodes in the network, centrality analysis was conducted using two centrality indicators: strength and closeness. Strength reflects the extent of direct connections a node has with others, while closeness assesses indirect connections. A node with the highest values of strength and closeness was deemed the core node. Moreover, bridge strength, defined as the total sum of the absolute values of the connections between a given node and all nodes outside its own cluster, was calculated to identify the bridge node that plays a crucial role in connecting different clusters within the network using the “networktools” package. We adopted “bootnet” package to estimate the accuracy and stability of the network. The accuracy of edge weights was evaluated by computing the 95% confidence intervals using a nonparametric bootstrap with 1,000 samples. The stability of the network was estimated by calculating the correlation stability coefficient using a case-dropping subset bootstrap with 1000 bootstrap samples. Cut-off values of 0.25 were considered indicative of acceptable stability, while values of 0.50 were deemed as good stability [24, 35]. Bootstrapped difference tests were conducted to determine if there were differences in node strength and edge weight using the “NetworkComparisonTest” package.
Results
Participant characteristics
Among the recruited subjects, ages ranged from 20 to 59 years, with a mean age of 46.93 years. The majority of participants were male (70.6%), married (89.3%), and employed. The mean scores for knowledge, social support, depression, anxiety, self-efficacy, and health-promoting lifestyles are 28.01 (SD = 12.31), 39.81 (SD = 7.52), 4.60 (SD = 3.25), 5.22 (SD = 3.50), 65.92 (SD = 22.43), and 58.25 (SD = 7.52), respectively. Table 1 shows the details of participant characteristics.
Table 1. Participant characteristics (n = 402)VariablesMean ± SD/N (%)Age (year) (Range: 20 ~ 59)46.93 ± 9.03Gender Male284 (70.6) Female118 (29.4)Marital status Married359 (89.3) Others43 (10.7)Employment status Employed309 (76.9) Unemployed93 (23.1)Educational level Primary school or less157 (39.1) Secondary school119 (29.6) Tertiary school or above126 (31.3)Monthly income (CNY) <250068 (16.9) 2500–5000122 (30.3) 5000–10,000114 (28.4) ≥ 10,00098 (24.4)Smoking history Smoking89 (22.1) Ex-smoker39 (9.7) No274 (68.2)Drinking history Regular drinking44 (10.9) Ex-drinker21 (5.2) Occasional drinking184 (45.8) No153 (38.1)Knowledge28.01 ± 21.31Social support39.81 ± 7.52Depression4.60 ± 3.25Anxiety5.22 ± 3.50Self-efficacy65.92 ± 22.43Health-promoting lifestyles58.25 ± 7.52
Potential predictors of health-promoting lifestyles
As presented in Table 2, we found significant differences in the nutritional domain of health-promoting lifestyles concerning gender, marital status, drinking history, age, knowledge, social support, depression, anxiety, and self-efficacy. The results also showed significant differences in stress management with respect to educational level, knowledge, social support, depression, anxiety, and self-efficacy. Additionally, significant differences in physical activity were noted regarding educational level, knowledge, depression, and self-efficacy.
Table 2. Potential predictors of health-promoting lifestylesVariablesHPLP II _NHPLP II _SHPLP II _PAMean ± SDMean ± SDMean ± SDGenderMale22.20 ± 3.8218.99 ± 4.3916.73 ± 4.50Female23.25 ± 3.9719.53 ± 4.3216.25 ± 4.69 t −2.481−1.1380.974 P 0.0140.2560.330Marital statusMarried22.65 ± 3.8919.19 ± 4.4316.63 ± 4.53Others21.40 ± 3.7618.84 ± 3.8816.28 ± 4.87 t −2.001−0.499−0.472 P 0.0460.6180.637Employment statusEmployed22.34 ± 3.8518.96 ± 4.3516.42 ± 4.54Unemployed23.09 ± 3.9719.77 ± 4.4117.16 ± 4.59 t −1.626−1.5690.980 P 0.1050.1170.168Educational levelPrimary school or less22.29 ± 3.6718.42 ± 4.4315.55 ± 4.30Secondary school22.37 ± 4.1419.20 ± 4.0717.21 ± 4.30Tertiary school or above22.93 ± 3.9120.02 ± 4.4417.29 ± 4.90 F 1.0674.7556.846 P 0.3450.0090.001Monthly income (CNY)< 250022.75 ± 4.8018.96 ± 4.3415.79 ± 4.852500–500022.45 ± 3.8618.66 ± 4.6416.11 ± 4.445000–10,00022.72 ± 3.6919.41 ± 4.0317.27 ± 4.25≥ 10,00022.18 ± 3.7419.15 ± 4.3716.94 ± 4.77 F 0.4341.0182.193 P 0.7290.3840.088Smoking historySmoking21.69 ± 3.7418.45 ± 4.3015.75 ± 4.48Ex-smoker23.05 ± 4.1718.97 ± 4.5616.79 ± 3.84No22.70 ± 3.8719.41 ± 4.3616.83 ± 4.66 F 2.7441.6461.935 P 0.0650.1940.146Drinking historyRegular drinking20.48 ± 3.7217.82 ± 4.1215.86 ± 3.61Ex-drinker23.57 ± 3.6419.33 ± 3.8917.71 ± 4.33Occasional drinking22.77 ± 3.5019.47 ± 4.3316.95 ± 4.48No22.65 ± 4.2519.12 ± 4.5216.21 ± 4.89 F 5.0041.7191.544 P 0.0020.1620.202Age r 0.1710.0420.054 P < 0.0010.4000.284Knowledge r 0.1950.1670.126 P < 0.001< 0.0010.012Social support r 0.1810.2200.084 P < 0.001< 0.0010.093Depression r −0.246−0.316−0.202 P < 0.001< 0.001< 0.001Anxiety r −0.117−0.144−0.032 P 0.0190.0040.528Self-efficacy r 0.3450.5060.502 P < 0.001< 0.011< 0.001t Independent t-tests, F one-way analysis of variance, HPLP II Health-Promoting Lifestyle Profile II, N nutrition, S Stress management, PA Physical activity
Hierarchical linear regression analysis
No multicollinearity was detected in the present study, as tolerance values were above 0.1 and VIF values were below 10. After controlling the significant characteristics of participants, the results showed that knowledge (β = 0.176, P < 0.001) and self-efficacy (β = 0.299, P < 0.001) had significant effects on the nutritional domain of health-promoting lifestyles. We also observed significant predictive roles of social support (β = 0.099, P = 0.027), depression (β=−0.181, P < 0.001), and self-efficacy (β = 0.434, P < 0.001) on stress management. In addition, self-efficacy (β = 0.485, P < 0.001) significantly predicted physical activity (Table 3).
Table 3. Hierarchical linear regressions of factors affecting health-promoting lifestylesVariableStep 1Collinearity statisticsStep 2Collinearity statisticsβ P ToleranceVIFβ P ToleranceVIFHPLP II_NGender0.1140.0410.7481.3370.0950.0650.7321.367Marital status0.0210.7040.7711.2980.0120.8160.6871.456Ex-drinker0.1670.0040.7111.4060.1690.0010.7051.419Occasional drinking0.288< 0.0010.3532.8360.250< 0.0010.3482.872No drinking0.1880.0300.3123.2080.2050.0090.3113.215Age0.1500.0070.7671.3040.227< 0.0010.6591.518Knowledge0.176< 0.0010.7721.295Social support0.0390.4350.7791.283Depression−0.0810.1320.6691.494Anxiety−0.0110.8360.6991.431Self-efficacy0.299< 0.0010.7951.257 R2 (ΔR2) 0.075 (0.075)0.249 (0.174) F 5.33411.732HPLP II_SSecondary school0.0820.1390.8081.238−0.0290.5500.7341.363Tertiary school or above0.1700.0020.8081.2380.0200.3580.5761.736Knowledge0.0160.7450.7501.334Social support0.0990.0270.8901.124Depression−0.181< 0.0010.6971.434Anxiety−0.0080.8750.6991.431Self-efficacy0.434< 0.0010.7521.3290.023 (0.023)0.305 (0.282)4.75524.676HPLP II_PASecondary school0.1660.0030.8081.2380.0560.2620.7421.347Tertiary school or above0.1770.0010.8081.2380.0180.7490.6031.660Knowledge−0.0400.4140.7641.308Depression−0.0810.0740.9171.091Self-efficacy0.485< 0.0010.7721.2950.033 (0.033)0.262 (0.229)6.84628.048 ***p < 0.001, **p < 0.01, VIF Variance Inflation Factor, HPLP II Health-Promoting Lifestyle Profile II, N Nutrition, *S * Stress management, *PA * Physical activity
Network analysis
As shown in Fig. 1, self-efficacy in nutrition (weight = 0.13) had a strong connection with the nutritional domain of health-promoting lifestyles. Self-efficacy for psychological well-being (weight = 0.23) and depression (weight=−0.11) were strongly related to stress management. In addition, self-efficacy in exercise (weight = 0.33) had a strong correlation with physical activity. The centrality analysis revealed that self-efficacy for psychological well-being had the largest values for strength (z-score = 1.58) and closeness (z-score = 1.81), meaning that it is the core node (Fig. 2). It also had the largest value for bridge strength (z-score = 1.16), highlighting its vital role in connecting various factors that affect health-promoting lifestyles (Fig. 3). The bootstrapped CIs were small, which suggested that the network was accurate (Fig. 4). The correlation stability coefficient was 0.751 for strength, 0.438 for closeness, and 0.517 for bridge strength, indicating that the network was stable (Fig. 5). The results of bootstrapped difference tests are presented in Figs. 6 and 7. Figure 6 shows that most node strengths significantly differ from each other. The self-efficacy for psychological well-being node has the greatest strength, which is significantly larger than that of most other nodes. Moreover, as shown in Fig. 7, most edges significantly differ from one another.
Fig. 1. Network structure of health-promoting lifestyles and its influencing factors
Fig. 2. Standardized centrality indices of network (z-scores) Note: SSU Support utilization, SSS Subjective support, SSO Objective support, SER Self-efficacy_Responsible health practice, *SEP * Self-efficacy_Psychological well-being, SEN Self-efficacy_Nutrition, SEE Self-efficacy_Exercise, MSP MS_prophylaxis, MSD MS_definition, MSC MS_complication, HPS Health-promoting lifestyles_Stress management, HPPA Health-promoting lifestyles_Physical activity, HPN Health-promoting lifestyles_Nutrition, D Depression, A Anxiety
Fig. 3. Standardized bridge centrality indices of network (z-scores). Note: SEP Self-efficacy_Psychological well-being, MSC MS_complication, SEN Self-efficacy_Nutrition HPPA Health-promoting lifestyles_Physical activity, HPS Health-promoting lifestyles_Stress management, D Depression, SEE Self-efficacy_Exercise, HPN Health-promoting lifestyles_Nutrition, SSU Support utilization, SSS Subjective support, MSP MS_prophylaxis, A Anxiety, SSO Objective support, SER Self-efficacy_Responsible health practice, *MSD * MS_definition
Fig. 4. Bootstrap 95% confidence intervals of the edge weight
Fig. 5. Correlation stability coefficient for strength, closeness, and bridge strength
Fig. 6. Estimation of node strength difference by bootstrapped difference test Note: Gray boxes indicate no significant differences between nodes, while black boxes represent nodes that exhibit significant differences (α = 0.05); White boxes display the values of node strength
Fig. 7. Estimation of edge weight difference by bootstrapped difference test Note: Gray boxes indicate no significant differences between nodes, while black boxes represent nodes that exhibit significant differences (α = 0.05); Blue boxes indicate positive correlations
Discussion
This study explored the factors influencing health-promoting lifestyles among young and middle-aged adults with metabolic risk factors. The results showed that age, drinking history, knowledge, and self-efficacy significantly affect dietary behaviors. Social support, depression, and self-efficacy can predict stress management, while self-efficacy also contributes to physical activity. The network analysis demonstrated the crucial role of self-efficacy for psychological well-being in the network of factors affecting health-promoting lifestyles. These findings provide a reference for developing targeted interventions to promote healthy lifestyles in this patient group.
In line with a previous study, this study confirmed the pivotal role of self-efficacy in shaping health-promoting lifestyles among young and middle-aged adults with metabolic risk factors [19]. Notably, whereas this prior work identified the effect of self-efficacy on healthy eating and exercise behaviors, our findings extended this understanding by demonstrating that enhancing self-efficacy is of paramount importance for improving stress management practices in this population. In addition, the network analysis showed that self-efficacy for psychological well-being serves as a core and bridge factor affecting health-promoting lifestyles. Therefore, when designing effective and targeted lifestyle interventions for young and middle-aged adults with metabolic risk factors, it is recommended to prioritize this crucial element, with particular emphasis on bolstering patients’ confidence in promoting psychological well-being.
The present study only revealed that knowledge about metabolic syndrome had significant effects on dietary behaviors among young and middle-aged adults with metabolic risk factors. A better understanding of the condition and the importance of its management contributes to healthier eating patterns such as choosing low-fat and low-sugar foods, increasing intake of vegetables and fruits, and regularly eating breakfast. Healthcare providers can employ suitable strategies to deliver the cardiometabolic information, thereby promoting a balanced diet in this patient group. Considering the non-significant effect observed on exercise and stress management, future investigations are needed to provide additional evidence.
In contrast to prior research suggesting a vital role of social support for dietary behaviors among adults with metabolic syndrome [18], our study found that social support significantly affects participants’ practices in managing stress. Strengthening support networks can help individuals cope with stressful events more effectively [36], and thus, this component should be addressed with appropriate strategies when developing lifestyle interventions for these patients. We also recommend further studies to explore the role of social support for exercise and dietary behaviors in this younger group of patients.
Our findings revealed that depression leads to poor stress management in young and middle-aged adults with metabolic risk factors, aligned with a previous study [22]. Patients with depression often experience feelings of hopelessness, loss of interest, insomnia, and lack of energy, which may prevent them from executing stress management strategies [22, 37]. Addressing depression via medications and psychological interventions may promote stress-coping abilities. More evidence on the effects of depression on other health-promoting lifestyles is warranted.
Additionally, we found that younger patients and those who were regular drinkers exhibited worse dietary behaviors. Special attention should be paid to these subgroups of patients when providing lifestyle modifications, and their needs should be addressed via tailored interventions.
Several limitations should be acknowledged in this study. Firstly, as this study employed a cross-sectional design, the findings warrant further examination through longitudinal and experimental studies. Secondly, the participants were recruited from a highly developed city in China using convenience sampling, which may limit the generalizability of the results. Thirdly, the Cronbach’s alpha values for the Social Support Rating Scale and the Hospital Anxiety and Depression Scale-Depression subscale are relatively low. Lastly, the use of self-reported tools for data collection might have introduced social desirability and recall biases. However, social desirability bias may be mitigated, as participants are more likely to respond truthfully when anonymity and confidentiality are ensured.
Conclusions
Self-efficacy, knowledge, social support, and depression are indispensable modifiable factors affecting health-promoting lifestyles among young and middle-aged adults with metabolic risk factors. In particular, self-efficacy for psychological well-being represents a key target for developing effective lifestyle interventions.
Supplementary Information
Supplementary Material 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wang W, Hu M, Liu H, Zhang X, Li H, Zhou F et al. Global Burden of Disease Study 2019 suggests that metabolic risk factors are the leading drivers of the burden of ischemic heart disease. Cell Metabolism. 2021;33(10):1943-56.e 2.10.1016/j.cmet.2021.08.00534478633 · doi ↗ · pubmed ↗
- 2Rus M, Crisan S, Andronie-Cioara FL, Indries M, Marian P, Pobirci OL et al. Prevalence and risk factors of metabolic syndrome: A prospective study on cardiovascular health. Med (Kaunas). 2023;59(10):1711.10.3390/medicina 59101711 PMC 1060864337893429 · doi ↗ · pubmed ↗
- 3Wang Q, Chair SY, Wong EM, Taylor-Piliae RE, Qiu XCH, Li XM. Metabolic syndrome knowledge among adults with cardiometabolic risk factors: A Cross-Sectional study. Int J Environ Res Public Health. 2019;16(1):159.10.3390/ijerph 16010159 PMC 633897030626137 · doi ↗ · pubmed ↗