Risk of Parkinson’s disease after human papillomavirus infection: a nationwide cohort study
Tien-Wei Hsu, Chih-Wei Hsu, Yu-Chen Kao, Shih-Jen Tsai, Ya-Mei Bai, Tung-Ping Su, Tzeng-Ji Chen, Mu-Hong Chen, Chih-Sung Liang

TL;DR
This study finds that people infected with human papillomavirus may have a higher risk of developing Parkinson’s disease, particularly in males.
Contribution
The novel contribution is identifying a potential link between HPV infection and increased Parkinson’s disease risk in a large-scale cohort study.
Findings
HPV-infected patients had a 1.25-fold higher risk of Parkinson’s disease compared to controls.
Male patients with HPV had a 1.48-fold higher risk of Parkinson’s disease than controls.
No significant association was found in female HPV-infected patients.
Abstract
Little is known about the association between human papillomavirus (HPV) infection and Parkinson’s disease (PD). This study aimed to explore the risk of incident PD following HPV infection. Patients 40 years or older with HPV infection diagnosed between 1996 and 2013 were included in the case group and were 1:4 matched with controls from the Taiwan National Health Insurance Research Database. A second matched control group of patients with acute respiratory infection (ARI) was also included. The outcome was incident PD, as determined using Cox proportional hazards. The study population included 80,318 patients with HPV infection, 322,952 non-HPV infection matched controls, and 80,318 ARI infection matched controls. There were 456 incident PD cases in the HPV group (0.84 per 1000 person-year), 2499 in the control group (0.43 per 1000 person-year), and 655 in the ARI control group (0.45…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
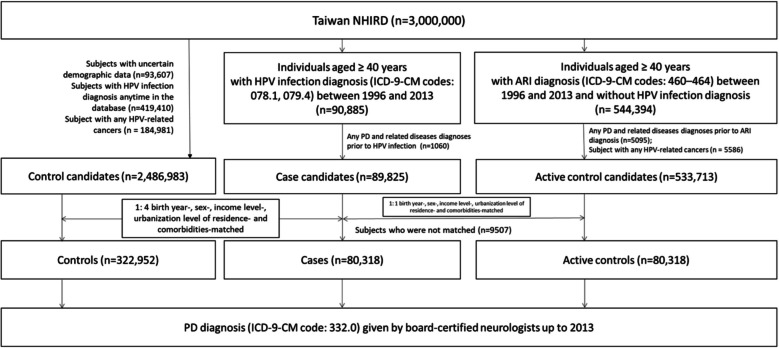 Figure 1
Figure 1- —https://doi.org/10.13039/100020595National Science and Technology Council
- —https://doi.org/10.13039/501100004606Chang Gung Medical Foundation
- —Taipei, Taichung, Kaohsiung Veterans General Hospital, Tri-Service General Hospital, Academia Sinica Joint Research Program
- —Veterans General Hospitals and University System of Taiwan Joint Research Program
- —http://dx.doi.org/10.13039/501100011912Taipei Veterans General Hospital
- —http://dx.doi.org/10.13039/501100007354Yen Tjing Ling Medical Foundation
- —Ministry of Science and Technology, Taiwan
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCervical Cancer and HPV Research · Multiple Sclerosis Research Studies · Parkinson's Disease Mechanisms and Treatments
Background
Parkinson’s disease (PD) is a neurodegenerative disorder affecting over 8.5 million people globally [1]. It is characterized by motor symptoms, including tremors, rigidity, and bradykinesia, and non-motor symptoms, including olfactory dysfunction, cognitive impairment, psychiatric symptoms, sleep disorders, and autonomic dysfunction [2]. Importantly, PD is associated with increased economic and caregiver burden, decreased overall quality of life, and a higher mortality [3]. The crucial pathophysiology of PD includes loss of dopaminergic neurons within the substantia nigra and aggregated α-synuclein (Lewy pathology), possibly due to genetic (e.g., SNCA,* LRRK2*,* GBA*) and environmental factors (e.g., pesticide exposure, prior head injury, beta-blocker use) [2].
Viral infection is one of the etiologies of PD [4]. Epidemiological studies have reported an increased risk of subsequent PD in patients infected with the hepatitis C virus [5], herpes virus [6], and Dengue virus infection [7]. Parkinsonism can emerge during other viral infections, such as Coxsackievirus and Flaviviruses (e.g., Japanese encephalitis and West Nile virus), showing a preference for basal ganglia involvement. Possible mechanisms include direct infection of the central nervous system, promotion of chronic inflammation, and the production of high levels of cytokines that can breach the blood–brain barrier. This process induces cellular oxidative stress, alters neurotransmitter systems, and leads to the misfolding and aggregation of pathological proteins [4, 8].
The human papillomavirus (HPV) is one of the most prevalent sexually transmitted deoxyribonucleic acid (DNA) viruses worldwide. Approximately 120 subtypes of HPV have been identified in various studies, approximately 40 of which result in infectious cycles in the host [9]. Most research has focused on the impact of HPV infection on mucosal and epithelial tissues, but not on the central nervous system (CNS). Low-risk types, such as HPV types 6 and 11, are associated with anogenital warts or low-grade changes in cervical cells [10, 11]. High-risk groups, especially types 16 and 18, are associated with cervical cancer, squamous cell carcinoma, and head and neck cancers [10, 12]. Importantly, preliminary research suggests that HPV infection is associated with Alzheimer's Disease through interactions with other pathogens and cytokines [13]. However, to date, no studies have examined the association between HPV infection and PD, a major neurodegenerative disease.
The objective of the current study was to examine the risk of incident PD after an HPV infection diagnosis using data from a nationwide cohort study. We hypothesized that patients with HPV infection would have an increased risk of subsequent PD compared with those without HPV infection.
Methods
Data source
The Taiwan National Health Insurance (NHI) program, established in 1995, is a universal single-payer system that provides compulsory health insurance to almost all residents of Taiwan; its coverage rate was approximately 99.7% at the end of 2013. The Taiwan National Health Insurance Research Database (NHIRD) is audited and released by the National Health Research Institutes for scientific study purposes. Individual medical records included in the NHIRD are anonymously maintained to protect patient privacy. The International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes are used for disease diagnosis. The NHIRD has been used extensively in many epidemiologic studies in Taiwan [14–17]. Taipei Veterans General Hospital’s institutional review board approved the study protocol and waived the requirement for informed consent since this investigation used de-identified data and no human subjects’ contact was required.
Inclusion criteria for individuals with HPV infection and the control group
Individuals aged ≥ 40 years who had a diagnosis of HPV infection (ICD-9-CM codes: 078.1, 079.4) given by board-certified internal medicine physicians, infectious disease physicians, urologists, colorectal physicians, otolaryngologists, obstetricians and gynecologists, and dermatologists between January 1, 1996, and December 31, 2013, at least twice and had no history of PD and related diseases (ICD-9-CM code: 332.x) before enrollment were included as the HPV infection cohort. We randomly selected two control groups from the NHIRD based on the same time point as the index date of HPV infection diagnosis for their corresponding cases using the following procedures. In the first control group, exact matching was performed to match this cohort in a 1:4 fashion to candidate controls who had no diagnosis of HPV infection anytime in the database based on birth year, sex, medical and mental comorbidities, income level, and urbanization level of residence (levels 1–3, most to least urbanized), a proxy for healthcare availability in Taiwan [18]. We also performed exact matching in a second control group to match this cohort in a 1:1 fashion to candidate controls who had no HPV infection diagnosis in the database, were not in the first control group, and had acute respiratory infections (ARI) (ICD-9-CM codes: 460–464) based on birth year, sex, medical and mental comorbidities, income level, and urbanization level of residence. Figure 1 illustrate the steps in participant selection and follow-up. In order to avoid the immortal time bias and the competing effect of death, all subjects survived at the end of the study (December 31, 2013). To minimized the risk of immortal time bias, we carefully aligning the starting time (time zero) for both cases and controls. Specifically, for each individual diagnosed with HPV infection (case), we selected a matched control on the same calendar day of the HPV diagnosis. This ensured that both groups began follow-up at the same time point, eliminating any potential for a period during which individuals in the case group would need to “survive” to qualify for inclusion. A diagnosis of PD (ICD-9-CM code: 332.0) made by board-certified neurologists at least twice was recorded during the follow-up period (from January 01, 1996, to December 31, 2013). Medical comorbidities included cerebrovascular diseases and traumatic brain injury. Mental comorbidities included depressive disorder, alcohol use disorder, and substance use disorder. Charlson comorbidity index (CCI) consisting of 22 physical conditions was also assessed to determine the systemic health conditions of all enrolled subjects [19].Fig. 1. Flowchart of population selection. ARI, acute respiratory infection; HPV, human papillomavirus; ICD-9-CM, International Classification of Diseases, 9th Revision, Clinical Modification; NHIRD, The Taiwan National Health Insurance Research Database; PD, Parkinson’s disease
Statistical analysis
For between-group comparisons, the F-test was used for continuous variables and Pearson’s X^2^ test for nominal variables. We applied stratified time-dependent Cox-regression analysis with adjustment for CCI scores to investigate the PD risk between groups. The HPV infection state was treated as a time-dependent variable. Sub-analyses stratified by sex were also performed. Given the insidious onset of PD, two types of sensitivity analyses were performed to validate the results by minimizing under-diagnosis of occult PD at the time of HPV infection diagnosis. In the “exclusion of observation period” model, the first year of observation after the diagnosis of HPV infection was excluded, eliminating all cases of PD diagnosed within the year following HPV infection diagnosis. In the “exclusion of enrollment period” model, only patients diagnosed with HPV before the date December 31, 2008, were included in the analysis; patients with HPV diagnosed after these time points were selectively excluded. Additional sensitivity analysis excluding patients with HPV and HPV-related cancers (cervical, oral, anal, vaginal, penile, vulvar cancers) was also performed. Statistical significance was set at two-tailed P ≤ 0.05. Data processing and statistical analyses were performed with SAS (version 9.1, SAS Institute, Cary, NC, USA).
Data availability
The NHIRD was released and audited by the Department of Health and Bureau of the NHI Program for the purpose of scientific research (https://www.apre.mohw.gov.tw/).
Results
We identified 80,318 patients previously infected with HPV, 322,952 patients without HPV infection as the first control group, and 80,318 patients who had ARI as the second control group, matched for age, sex, physical comorbidities, mental comorbidities, income, and residence (Table 1). The HPV group had a higher CCI score (mean = 2.11, standard deviation, SD = 1.84) compared with the control group (mean = 1.92, SD = 1.87, z-score > 3.89) and the ARI control group (mean = 1.93, SD = 1.85, z-score > 3.89). Table 1. Demographic characteristics between patients with HPV infection and controlsAnalysis 2^b^Analysis 1^a^(C) Control group(n = 322,952)(P) Patients with HPV infection (n = 80,318)(A) ARI control group(n = 80,318)P vs. C^a^p-valueP vs. A^b^p-valueBirth year (n, %) > 0.999 > 0.999 < 194054,704 (17.0)13,676 (17.0)13,676 (17.0) 1940–194955,756 (17.4)13,939 (17.4)13,939 (17.4) 1950–1959112,604 (35.0)28,151 (35.0)28,151 (35.0) ≧196098,208 (30.6)24,552 (30.6)24,552 (30.6)HPV diagnosis age (years, SD)54.69 (11.33)HPV-related cancers (n, %)1068 (0.1)Sex (n, %) > 0.999 > 0.999 Male36,606 (45.6)36,606 (45.6)36,606 (45.6) Female43,712 (54.4)43,712 (54.4)43,712 (54.4)Medical comorbidities (n, %) Cerebrovascular diseases33,616 (10.5)8404 (10.5)8404 (10.5) > 0.999 > 0.999 Traumatic brain injury7320 (2.3)1830 (2.3)1830 (2.3) > 0.999 > 0.999 Depressive disorder18,012 (5.6)4503 (5.6)4503 (5.6) > 0.999 > 0.999 Alcohol use disorder7816 (2.4)1954 (2.4)1954 (2.4) > 0.999 > 0.999 Substance use disorder8288 (2.6)2072 (2.6)2072 (2.6) > 0.999 > 0.999CCI scores (SD)1.92 (1.87)2.11 (1.84)1.93 (1.85) < 0.001^c^ < 0.001^c^Level of urbanization (n, %) > 0.999 > 0.999 1 (most urbanized)43,904 (13.7)10,976 (13.7)10,976 (13.7) 2131,396 (40.9)32,849 (40.9)32,849 (40.9) 3 (most rural)145,972 (45.4)36,493 (45.4)36,493 (45.4)Income-related insured amount (n, %) > 0.999 > 0.999 ≤ 19,100 NTD/month129,224 (40.6)32,767 (40.6)32,767 (40.6) 19,001 ~ 42,000 NTD/month145,316 (45.1)36,424 (45.1)36,424 (45.1) > 42,000 NTD/month46,732 (14.3)11,547 (14.3)11,547 (14.3)*HPV *human papillomavirus, *SD *standard deviation, *CCI *Charlson Comorbidity Index, *NTD *new Taiwan dollars, *ARI *acute respiratory infection^a^A comparison between the control group (C) and patients with HPV (P)^b^A comparison between the patients with HPV (P) and the patients with ARI (A)^c^z-score > 3.89, two-tailed p-value < 0.001
After adjustment for CCI scores (Table 2), patients with HPV infection were associated with a higher subsequent risk of PD (Hazard ratio, HR = 1.25, 95% confidence interval, CI = 1.13 to 1.39) compared with the control group. When comparing with the ARI control group, patients with HPV infection were still associated with a higher risk of PD (HR = 1.20, 95% CI = 1.04 to 1.38). Stratified by sex, male patients with HPV were still associated with an increased risk of PD, no matter when comparing with the control group (HR = 1.48, 95% CI = 1.28 to 1.71) or the ARI control group (HR = 1.31, 95% CI = 1.09 to 1.59). However, the risk of subsequent PD in female patients with HPV infection did not show a significant difference from the control group (HR = 1.04, 95% CI = 0.89 to 1.22) nor the ARI control group (HR = 1.08, 95% CI = 0.88 to 1.33). Table 2. Risk of Parkinson’s disease between groupsParkinson’s disease^a^Events (n, 1000 person-year)HR95% CIAnalysis 1All sample Control group2499 (0.43)1 (ref)- Patients with HPV infection456 (0.84)1.25****1.13–1.39Male sample Control group1227 (0.47)1 (ref)- Patients with HPV infection258 (1.04)1.48****1.28–1.71Female sample Control group1272 (0.41)1 (ref)- Patients with HPV infection198 (0.67)1.040.89–1.22Analysis 2All sample ARI control group655 (0.45)1 (ref) Patients with HPV infection456 (0.84)1.20****1.04–1.38Male sample ARI control group355 (0.54)1 (ref) Patients with HPV infection258 (1.04)1.31****1.09–1.59Female sample ARI control group300 (0.38)1 (ref) Patients with HPV infection198 (0.67)1.080.88–1.33*HPV *human papillomavirus, *CCI *Charlson Comorbidity Index, *HR *hazard ratio, *CI *confidence interval, *ARI *acute respiratory infection^a^Stratified time-dependent Cox regression analyses with adjustment of CCI scores
In the sensitivity analyses (Table 3), when comparing with the control group, after the exclusion of the first year observation (HR = 1.25, 95% CI = 1.13 to 1.39). After the exclusion of the first 3-year and 5-year observation, we still had consistent findings. After the exclusion of enrollment after 2009 (HR = 1.26, 95% CI = 1.13 to 1.41) and after the exclusion of patients with HPV-related cancers (HR = 1.27, 95% CI = 1.14 to 1.41), the HPV group still showed an increased risk of subsequent PD. When comparing with the ARI control group, the HPV group had higher risks of PD in all sensitivity test. Table 3. Sensitivity analyses for PD riskHR (95% CI)All sampleExcluding the first year observationExcluding the first 3-year observationExcluding the first 5-year observationExcluding those enrolled after 2009Excluding patients with HPV-related cancersAnalysis 1Control group1 (ref)1 (ref)1 (ref)1 (ref)1 (ref)1 (ref)Patients with HPV infection**1.25 (1.13–1.39)****1.25 (1.13–1.39)****1.25 (1.13–1.39)****1.26 (1.13–1.40)****1.26 (1.13–1.41)****1.27 (1.14–1.41)Analysis 2ARI control group1 (ref)1 (ref)1 (ref)1 (ref)1 (ref)1 (ref)Patients with HPV infection1.20 (1.40–1.38)****1.20 (1.04–1.38)****1.20 (1.04–1.38)****1.23 (1.07–1.41)****1.21 (1.04–1.40)****1.20 (1.05–1.38)***HPV *human papillomavirus, *CCI *Charlson Comorbidity Index, *HR *hazard ratio, *CI *confidence interval, *ARI *acute respiratory infectionNote: stratified time-dependent Cox regression models with adjustment of CCI scores
Discussion
This nationwide cohort study followed participants for 18 years and showed a clear and robust association between HPV infection and incident PD. After adjustment, we found that patients with HPV infection had a 1.25-fold increased risk of incident PD compared to controls without HPV infection. This finding remains consistent when comparing to the second control group who had ARI and when possible cases of insidious onset of PD are excluded. Stratified by sex, only male patients with HPV infection had a higher risk of subsequent risk of PD, but not female patients. HPV papillomavirus infections are associated with the development of various cancers and other health issues [4, 10]. Our findings suggest that HPV infection may be a risk factor for PD. Therefore, healthcare professionals must emphasize the importance of prevention through education of the general public. Educating individuals about the risks associated with HPV infection and promoting preventive measures can significantly contribute to reducing the incidence of serious HPV-related complications.
Viral infections induce PD through various cellular mechanisms. These infections affect host cell responses, diminishing neuronal function by (i) increasing reactive oxygen species (ROS) through interference with the electron transport system and hindering antioxidant production and (ii) promoting neuroinflammation by enhancing the secretion of proinflammatory cytokines [8]. HPV infections follow a similar pathophysiological process. Expression of the E6 protein increases ROS levels in both HPV-positive and HPV-negative cells [20]. E6 expression also decreases the expression of superoxide dismutase isoform 2 and glutathione peroxidase [20]. During the inflammatory process, pro-inflammatory cytokines act on the endothelium of blood–brain barrier cells, triggering the upregulation of adhesion molecules and recruiting circulating T cells and monocytes [21]. HPV is an immunological modulator, which actively induces Th2 and Th17 pathways, with resultant increased production of interleukin-17 (IL-17), IL-13, and subsequently tumor necrosis factor-α (TNF-α) [22, 23]. Furthermore, elevated serum IL-6, IL-8, IL-1β, and macrophage inflammatory protein-1α (MIP-1α) were also observed in patients with HPV infection [24, 25]. Animal studies have shown that neurotoxin 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP)-treated mice have increased numbers of Th17 cells in the substantia nigra [26, 27]. Clinical studies have shown increased Th17 frequency in the peripheral blood of patients with PD compared to healthy controls [28]. Th17 cells actively participate in nigral neurodegeneration by infiltrating the nigral region, which results in excessive activation of microglial cells [29]. Prolonged TNF-α expression leads to continued microglial activation and recruitment of monocytes/macrophages, ultimately resulting in the death of dopaminergic neurons [30]. In the pathogenesis of PD, elevated expression of interferon-gamma (IFN-γ), IL-6, and IL-1β also indicates the crucial role of the inflammatory response in the brain [31]. The severity of PD is correlated with elevated levels of TNF-α and IL-1β [25].
The HPV E6 oncoprotein, commonly generated by HPV 16 and 18, binds to a cellular protein of 100 kDa, termed E6-associated protein (E6-AP) [32, 33]. Subsequently, the E6/E6AP complex recruits and degrades p53, a tumor suppressor protein, which is a major carcinogenic mechanism employed by HPV [32]. E6-AP, homologous to the E6-AP C-terminus domain family E3 ubiquitin ligase, is a component of Lewy bodies in the post-mortem PD brain [34]. In the absence of E6, E6-AP demonstrates ubiquitin ligase activity and promotes the degradation of α-synuclein [33, 34]. Previous studies have demonstrated that the expression of E6 reduces co-expressed E6AP, both in the high-risk type, HPV 16, and the low-risk type, HPV 11 [35, 36]. Long-term infection by HPV with downregulation of E6AP expression, leading to cumulative α-synuclein, may be another mechanism associated with viral PD. However, HPV is an epitheliotropic pathogen. It may be possible for HPV to affect nerve cells or infect the brain. A clinical observational study screened 50 HPV 16-associated samples (15 cervical, 35 head, and neck cancers) and found that the HPV 16 genome exists in a non-replicating form in neurons and constitutively produces high levels of E6 and E7 proteins. [37] In a non-cancer study, HPV antigen expression was elevated in patients with Rasmussen encephalitis, whereas there were no detectable HPV antigens in control patients. [38] Evidence suggests that HPV infects nerve cells in the brain. Nevertheless, further in vivo studies are required to confirm the hypothesis that E6-AP expression is altered by CNS HPV infection.
The prevalence of Parkinson's Disease (PD) is higher in males than in females, with a male-to-female ratio of approximately 1.2:1 to 1.5:1 [39, 40]. This is also reflected in our results, showing that male HPV patients have a higher risk of PD. In past studies on other viral infections and incident PD, it was also found that males had a significantly higher risk while females did not. For instance, after Dengue infection, males had a 3.51-fold higher incidence of PD (HR: 3.51, 95% CI: 1.76 to 7.00), whereas females showed no significant increase (HR: 1.75, 95% CI: 0.73 to 4.19) [7]. Estrogen might play an important role in neuroprotection from development of PD [41]. Several possible mechanisms between estrogen and anti-PD have been studied, including anti-aggregation and fibril destabilization properties in α-synuclein, decreased inflammatory cytokines, decreased microglia activation, decreased leukocyte CNS entry, decreased apoptosis of neurons, increased dopamine synthesis, and increased expression of neurotrophic factors, such as glial cell line-derived neurotrophic factor (GDNF) and brain-derived neurotrophic factor (BDNF) [41–45]. Nevertheless, we still need further studies to investigate the exact mechanisms underlying the sex difference in risk of PD after HPV infection.
Limitation
Our study has some limitations. First, HPV infections were identified using ICD-9-CM codes in the administrative claims data. Specific HPV types could not be identified from the database. Second, the cumulative incidence of PD was relatively low in our cohort. There were several possible reasons. Although our follow-up period can extend up to 18 years, this duration may be relatively short for the development of PD in some cases. In addition, we used a relatively strict definition of PD, using only one ICD-9 code (332.0), and excluded other related codes. Third, the NHIRD database lacks genetic data; however, it is important to note that inherited genetic mutations linked to PD are widely acknowledged. These mutations are associated with approximately 3–5% of sporadic cases and 30% of familial cases [2]. Fourth, the HPV vaccine would be an important confounding factor. However, in Taiwan, HPV vaccination was self-funded and not covered by the National Health Insurance before 2018. The data period for this study is from 1996 to 2013; therefore, vaccination data would not be recorded in this dataset. Hormonal contraceptives in the NHIRD are also self-funded, meaning they are not covered by the NHIRD, either. Fifth, lifestyle, pollution exposure, or other viral infections might also influence the development of PD, but such data are unavailable in our database or are too complex to calculate. In addition, while we adjusted our results for the CCI score, which includes various clinical conditions, it remains challenging to assess the individual impact of each disease within the CCI index on PD development. Identical CCI scores may reflect different clinical conditions, potentially resulting in unequal effects on the development of PD.
Conclusions
Our nationwide longitudinal study showed a clear and clinically significant association between HPV infection and the incidence of PD. The increased risk of incidence of PD further consolidates the need for enhanced vigilance and consideration of populations vulnerable to HPV infection. Public education initiatives are needed to inform people that HPV infection may be a risk factor for incident PD. However, further studies are required to validate the mechanisms underlying this association, especially for the sex difference. These studies could even be extended to explore whether there are common or unique mechanisms among different viruses in relation to viral infections and neurodegenerative diseases. In addition to its role in preventing cancer and genital warts, the HPV vaccine may have a preventive effect on PD. This study provides supplementary support for advocating HPV vaccination in clinical practice.
Supplementary Information
Additional file 1. STROBE Statement—Checklist of items that should be included in reports of cohort studies.