Streamlining care through patient navigation: a retrospective cohort study of timely anti-HER2 therapy in early breast cancer in a low-middle income country
Emad Shash, Fatema Alaa, Engy Maher, Julia F. Rostom, Alaa Ibrahim, Rania Said, Nada Abou El-Kheir, Mona Elhosary, Reem Eid

TL;DR
A patient navigation program in Egypt helped speed up anti-HER2 cancer treatment for patients, reducing delays in a low-middle income country.
Contribution
Demonstrates that patient navigation can effectively reduce treatment delays in LMICs for early HER2-positive breast cancer patients.
Findings
Navigation significantly reduced the time from MOH approval to treatment start (T4) in primary and sensitivity analyses.
Overall time from registration to treatment initiation decreased across the full year with navigation, despite rising patient volumes.
Pathological complete response rates remained comparable between groups with and without navigation.
Abstract
Timely initiation of therapy is critical for patients with HER2-positive early breast cancer, especially in low- and middle-income countries (LMICs) where health-system constraints delay care. We evaluated whether a Patient Navigation Program could reduce time from registration to initiation of dual anti-HER2 therapy in Egypt. Retrospective cohort study at the Breast Cancer Comprehensive Center (BCCC). Trained navigators tracked diagnostics, scheduled multidisciplinary tumor board (MDT), prepared/submitted Ministry of Health (MOH) approval files, monitored approval, and booked the earliest infusion slot. The primary endpoint was time from registration to therapy start; secondary endpoints were prespecified intervals—T1 (registration→MDT), T2 (MDT→MOH submission), T3 (MOH submission→MOH approval), and T4 (MOH approval→therapy start), time to surgery, and pathological complete response…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
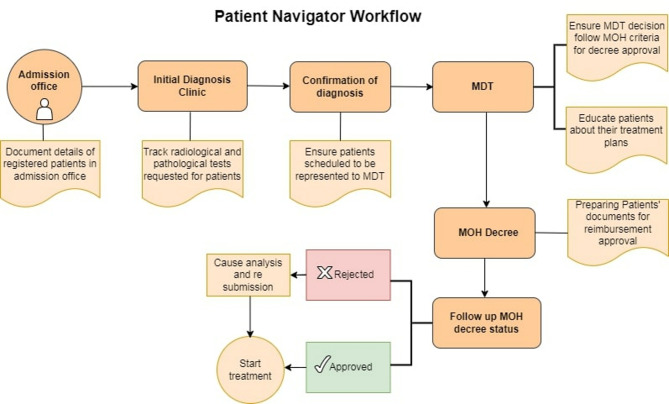 Figure 1
Figure 1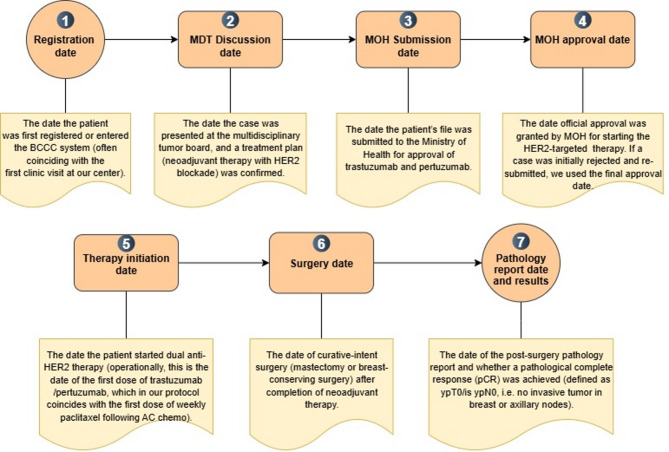 Figure 2
Figure 2- —Cairo University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Cancer Incidence and Screening · Advances in Oncology and Radiotherapy · Economic and Financial Impacts of Cancer
Background
Breast cancer is the most diagnosed cancer and the leading cause of cancer death among women globally [1]. In 2020, an estimated 2.3 million new cases and 685,000 deaths were reported, with a disproportionate burden in low- and middle-income countries (LMICs) where constrained systems drive later diagnosis and treatment delays [1, 2]. Timely therapy is critical: longer intervals to treatment are consistently associated with more advanced disease at presentation and poorer survival [3–5].
Human epidermal growth factor receptor 2 (HER2)–positive breast cancer is biologically aggressive but highly curable when modern therapy is delivered without delay. In the neoadjuvant setting, dual HER2 blockade (trastuzumab plus pertuzumab) with chemotherapy significantly increases pathological complete response (pCR) versus chemotherapy alone or single-agent HER2 targeting [6]. Because pCR correlates with lower recurrence and improved survival, delays in initiating HER2-targeted treatment may compromise the probability of cure.
At the Breast Cancer Comprehensive Center (BCCC), National Cancer Institute, Cairo University (Cairo, Egypt), the standard pathway for HER2-positive early breast cancer includes neoadjuvant chemotherapy plus dual anti-HER2 therapy (trastuzumab + pertuzumab), definitive surgery, and adjuvant systemic therapy and/or radiotherapy as indicated. Within the public sector, starting dual anti-HER2 therapy requires Ministry of Health (MOH) approval based on a complete dossier (histopathology/receptor status and baseline assessments). This administrative step, alongside communication gaps and patient-level barriers (navigating appointments, document acquisition, health literacy), can introduce clinically meaningful delays—challenges echoed in other Egyptian public cancer centers. Egypt’s Presidential Initiative for Women’s Health (launched 2019) has expanded screening and access; by March 2022, >16.5 million women had been screened, and the government committed to providing innovative cancer therapies free of charge to eligible patients [7]. Realizing these gains, however, depends on parallel improvements in care coordination after diagnosis.
Patient navigation is an established strategy to reduce delays and inequities. Originating in 1990 at Harlem Hospital, navigation for underserved patients substantially improved breast cancer outcomes (five-year survival ~ 70% with-navigation versus 39% without) [8]. Across diverse settings, navigators—nurses, social workers, or trained laypersons—coordinate appointments, facilitate communication, and resolve logistical barriers, shortening time from abnormality to diagnosis and from diagnosis to treatment, particularly for vulnerable groups [9–15]. International bodies, including the Breast Health Global Initiative (BHGI) and WHO, endorse navigation as part of comprehensive cancer control in LMICs [15].
Aligned with these directives, the Breast Cancer Comprehensive Center (BCCC) established a dedicated Patient Navigation Program in 2022, the first of its kind in our region [16]. The program proactively guides patients from first visit through treatment completion, targeting expedited multidisciplinary team review, MOH approval, and therapy scheduling, while reinforcing patient education. This study evaluates the program’s impact on timeliness of dual anti-HER2 therapy initiation and downstream outcomes (including pCR), with the hypothesis that navigation meaningfully shortens the interval from registration to treatment start and advances alignment with international benchmarks.
Methods
Intervention: patient navigation program
Pre-implementation (without navigation). There was no standardized, centralized process to coordinate diagnostics, multidisciplinary tumor board (MDT) scheduling, Ministry of Health (MOH) reimbursement submission/approval, and infusion booking. Steps were fragmented, largely clinician-initiated, and patients frequently transported documents between services.
Post-implementation (with navigation). The Patient Navigation Program (Fig. 1) deployed trained navigators who: (1) tracked completion of required diagnostics and ensured reports were available; (2) scheduled the earliest feasible MDT discussion; (3) assembled, prepared, and submitted complete MOH reimbursement files; (4) monitored MOH approval status and resolved deficiencies; and (5) booked the first available infusion appointment immediately upon approval.
Fig. 1. Patient Navigation Program workflow. Navigator-coordinated steps from admission through MDT, MOH approval, and treatment start. Activities include verifying MOH criteria at MDT, preparing/submitting reimbursement documents, tracking approval status, educating patients, and booking the earliest infusion slot upon approval. Abbreviations: MDT, multidisciplinary tumor board; MOH, Ministry of Health
Study design
We conducted a retrospective cohort study at the Breast Cancer Comprehensive Center (BCCC) to evaluate the impact of the Patient Navigation Program on treatment timeliness for HER2-positive early breast cancer.
Patients were grouped as without navigation (before implementation) and with navigation (after implementation, with active navigator involvement). The program launched in mid-2022 and was fully operational from January 2023.
- Primary analysis: consecutive patients in the six months immediately before full implementation (July–December 2022; without navigation) versus the first six months after (January–June 2023; with navigation).
- Sensitivity analysis: the originally reported window of May–December 2022 (without navigation) versus January–December 2023 (with navigation) to assess robustness.
Objectives
Primary objective
determine whether the Patient Navigation Program reduced the time from registration at BCCC to initiation of dual anti-HER2 therapy (start of trastuzumab/pertuzumab during neoadjuvant chemotherapy).
Secondary objectives
(1) decompose the total interval into component steps—registration→MDT decision, MDT decision→MOH submission, MOH submission→MOH approval, and MOH approval→therapy start—to localize improvements; (2) compare time from therapy initiation to surgery between cohorts; and (3) compare pathological complete response (pCR) rates between cohorts.
Patient population
We included consecutive adults (≥ 18 years) with stage I–III HER2-positive invasive breast carcinoma (Immunohistochemistry (IHC)3 + or In situ hybridization (ISH)-amplified) planned for neoadjuvant chemotherapy plus dual anti-HER2 therapy during the study windows, who initiated neoadjuvant treatment at BCCC in 2022 or 2023.
The standard neoadjuvant protocol comprised an anthracycline–taxane backbone with dual HER2 blockade: four cycles of doxorubicin/cyclophosphamide (AC) followed by 12 weeks of weekly paclitaxel with concurrent trastuzumab and pertuzumab. Surgery is part of the standard pathway; however, surgery was not required for inclusion in time-interval analyses. Patients missing any key timestamp needed for interval computation were excluded from interval endpoints.
Exclusion criteria
de novo metastatic (stage IV) disease; no neoadjuvant dual HER2 blockade (e.g., contraindication to targeted therapy or upfront surgery/adjuvant approach).
Data collection
Data were abstracted retrospectively from the institutional electronic medical record (EMR) and patient files. Operational definitions and their positions along the pathway are mapped in Fig. 2, defining four prespecified intervals (T1–T4) and downstream dates (therapy initiation, surgery, pathology/pCR). All entries (expanded definition in supplementary Table 1 A & 1B) were double-checked; discrepancies or extreme outliers were adjudicated by chart review. We report observed intervals without inferring causality; occasional clinical reasons for delay (e.g., intercurrent illness, additional clearances, patient scheduling constraints) were documented during review.
Fig. 2. Timeline capture points. T1 (registration→MDT), T2 (MDT→MOH submission), T3 (submission→approval), T4 (approval→therapy start); plus, downstream dates (surgery; pathology/pCR). Abbreviations: MDT, multidisciplinary tumor board; MOH, Ministry of Health; pCR, pathological complete response; HER2, human epidermal growth factor 2; BCCC, breast comprehensive cancer center; AC, doxorubicin (Adriamycin) and cyclophosphamide
Endpoints
Primary endpoints
system time intervals—T1 (registration→MDT), T2 (MDT→MOH submission), T3 (MOH submission→MOH approval), T4 (MOH approval→therapy start), and their sum (total time).
Secondary endpoint
pCR among patients who underwent definitive surgery with evaluable pathology. Surgical procedures and outcomes were not prespecified primary endpoints.
Statistical analysis
Baseline characteristics were summarized descriptively. For each interval (T1–T4, total), we compared without-navigation (July–December 2022) versus with-navigation (January–June 2023) using non-parametric mann-whitney u test; as normality wasn’t met. Where variances were unequal, Welch’s correction was used. Results are reported as mean (SD) or median (IQR) as appropriate, with mean differences and 95% confidence intervals. pCR rates were compared using chi-square tests. Statistical significance was set at p < 0.05 (two-sided). Sensitivity analyses repeated interval comparisons for May–December 2022 versus January–December 2023. Analyses were conducted in IBM SPSS Statistics v26. Given the programmatic, retrospective design and similar year-to-year case mix, no multivariable adjustment was prespecified.
Results
Cohorts and analytic windows
The 2023 cohort (with navigation) represents the first full operational year of the Patient Navigation Program, coinciding with increasing referrals driven by national early-detection efforts. The 2022 cohort (without navigation) covered a partial year beginning in May. To improve comparability, our primary analysis was conducted using symmetric six-month windows: July–December 2022 (without navigation) versus January–June 2023 (with navigation). A sensitivity analysis was also performed comparing the entire available periods: May–December 2022 versus January–December 2023.
Primary analysis: July–December 2022 vs. January–June 2023
Patient demographics and baseline
The two cohorts were demographically well balanced (Table 1). Mean age was 45.6 ± 10.3 years in 2022 and 46.4 ± 9.9 years in 2023. Referral patterns were similar, with most patients from Greater Cairo (78.3% vs. 70.0%), followed by Delta (10.0% vs. 16.7%), Upper Egypt (10.0% vs. 11.7%), and Suez/Ismailia/Red Sea (1.7% each).
Table 1. Baseline characteristics and pathological complete response (pCR) in the primary analysis cohorts (HER2-positive EBC treated with neoadjuvant chemotherapy + Dual anti her 2 therapy at BCCC)Characteristic2022 (Without navigation: Jul–Dec) n = 1202023 (With navigation: Jan–Jun) n = 120p-valueAge,** years** (mean ± SD)45.6 ± 10.346.4 ± 9.9—Geographic referral region, n (column %)Greater Cairo94 (78.3)84 (70.0)—Delta12 (10.0)20 (16.7)—Upper Egypt12 (10.0)14 (11.7)—Suez/Ismailia/Red Sea2 (1.7)2 (1.7)—Evaluable for pCR, n 115
117 —pCR (per pathology)**, n (row %)Yes78 (67.8)81 (69.2) 0.818 No37 (32.2)36 (30.8)Abbreviations: BCCC, Breast Cancer Comprehensive Center; EBC, early breast cancer; pCR, pathological complete response pCR assessed among patients who underwent definitive surgery with evaluable pathology; percentages shown within the evaluable denominator for each cohortNotes:• Geographic rows sum to the cohort totals (n = 120 per column)• pCR rows sum to the number evaluable for pCR (115 in 2022; 117 in 2023)• “—” indicates not tested/not applicable for baseline descriptors
System intervals to therapy
The navigation program significantly shortened the MOH approval → therapy initiation interval (T4) (p = 0.008) (Table 2). Other intervals were not statistically different: registration → MDT (T1, p = 0.764), MDT → MOH submission (T2, p = 0.762), and submission → approval (T3, p = 0.678). The total time (registration → therapy) was modestly reduced but not statistically significant (p = 0.127).
Table 2. Between-cohort comparison of system time intervals (primary analysis: July–Dec 2022 vs. Jan–Jun 2023)IntervalMedian (Days)(Minimum – Maximum)Test statistics (U)p-valueT1: Registration → MDT24 (0–360)7.360.764T2: MDT → MOH submission54 (1–198)6.340.762T3: MOH submission → MOH approval6 (0–15)7.170.678T4: MOH approval → therapy start19 (0–168)5.210.008Total: Registration → therapy124 (28–448)6.380.127Abbreviations: MDT, multidisciplinary tumor board; MOH, Ministry of HealthNotes: Comparisons are between without-navigation (July–December 2022) and with-navigation (January–June 2023) cohorts. U denotes the Mann–Whitney U test statistic as reported; p-values are two-sided. Lower interval values indicate faster progression to therapy
Pathological complete response (pCR)
pCR outcomes were similar: 78 patients in the 2022 cohort vs. 81 in 2023 achieved pCR (Table 1). The difference was not statistically significant (p = 0.818).
Sensitivity analysis: May–December 2022 vs. January–December 2023
In a sensitivity analysis including 441 patients (162 in 2022; 279 in 2023), results were directionally consistent with the primary analysis and more robust: the total time from registration to initiation of dual anti-HER2 therapy decreased from 146.2 ± 76.6 days in 2022 to 121.6 ± 50.4 days in 2023 (difference − 24.6 days, p < 0.001). By interval, T1 (registration→MDT) improved from 44.4 to 36.6 days (p = 0.174), T2 (MDT→MOH submission) from 63.3 to 56.9 days (p = 0.108), T3 (submission→approval) increased slightly from 6.2 to 7.4 days (+ 1.2 days; p < 0.001), and T4 (approval→therapy start) shortened substantially from 32.4 to 20.8 days (–11.6 days; p < 0.001). pCR rates were similar (64.1% in 2022 vs. 69.9% in 2023; p = 0.76). Collectively, these data underscore that the program’s major effect was acceleration of T4, yielding a statistically significant reduction in overall time to therapy despite higher 2023 volumes (Table 3).
Table 3. Comparative time intervals from registration to dual HER2 therapy (Without- vs. With-Navigation)Interval2022 (Without-navigation) Mean ± SD (days)2023 (With-navigation) Mean ± SD (days)Mean Differencep-valueT1: Registration → MDT44.4 ± 69.036.6 ± 31.2–7.80.174T2: MDT → MOH Submission63.3 ± 41.556.9 ± 34.3–6.40.108T3: Submission → Approval6.2 ± 3.17.4 ± 2.90+ 1.2< 0.001T4: Approval → Therapy32.4 ± 28.120.8 ± 22.2–11.6< 0.001Total: Registration → Therapy146.2 ± 76.6121.6 ± 50.4–24.6< 0.001 pCR Rates
2022 (Without navigation)
2023 (With navigation) 64.1%69.9%0.76SD: standard deviation. Negative differences indicate faster times in 2023. Bolded intervals (T3, T4 and Total) had statistically significant reductions
Discussion
Introducing a Patient Navigation Program at a high-volume public cancer center in an LMIC context was associated—on our primary, symmetric six-month analysis—with a targeted, statistically significant reduction in the MOH approval → therapy start interval (T4; p = 0.008) for patients with early HER2-positive breast cancer starting dual anti-HER2 therapy. Upstream intervals (registration→MDT, MDT→MOH submission, submission→approval) and the total registration→therapy time showed non-significant trends (p = 0.764, 0.762, 0.678, and 0.127, respectively), indicating that navigation most effectively addressed the operational bottleneck between approval and infusion scheduling—the segment most under institutional control. This pattern accords with global evidence that navigation mitigates system barriers and accelerates treatment initiation [9].
Our findings mirror experiences from multiple settings where navigation was adapted to local constraints yet consistently accelerated care. In the United States, navigation began as an equity-focused intervention in Harlem and targeted practical barriers such as insurance authorizations, transportation, appointment coordination, and communication, improving outcomes for underserved women [10]. Subsequent efforts—including the NCI-sponsored Patient Navigation Research Program—embedded navigators within clinic workflows to track each step from abnormal screening through diagnostic resolution to treatment initiation, with studies demonstrating faster resolution and higher odds of on-time treatment start [9, 10]. Taken together, the U.S. experience underscores that barrier-specific problem solving and proactive tracking—both core to our program—are key mechanisms of effect.
In Brazil, the national “60-day Law” requires public hospitals to start treatment within 60 days of diagnosis. Navigation teams in Sistema Único de Saúde (SUS) operationalized this mandate by monitoring the legal “clock,” assembling required documentation in advance, securing appointments across siloed services, and escalating delays to hospital leadership. Programs in Rio de Janeiro reported markedly shorter timelines and high compliance with the 60-day target when navigators were engaged [12]. As in Egypt, centralized coverage alone did not ensure timeliness; navigation provided the coordination layer that translated funding into punctual care.
In Rwanda, where workforce and geographic constraints are pronounced, a digitally enabled multi-hospital navigation model linked peripheral and referral centers, standardized referral forms, flagged missing diagnostics, and used dashboards to shorten handoffs across pathology, imaging, and oncology clinics. Reported time from diagnosis to treatment start fell substantially after implementation [14]. This experience highlights the additive value of digital tracking alongside human navigators—a direction that could further compress intervals within Egypt’s largely paper-based approval environment.
Across these contexts, navigation is flexible and transferable: it targets the dominant barriers in each system—socioeconomic/insurance (U.S.), legal timeframes and service fragmentation (Brazil), workforce and geography (Rwanda), or administrative bottlenecks and rising volumes (Egypt)—yet converges on the same outcome: faster movement to definitive therapy [9, 10, 12, 14].
Our sensitivity analysis reinforced these conclusions: when all available months were included (May–December 2022 vs. January–December 2023), the total time from registration to dual anti-HER2 therapy decreased by 24.5 days (p < 0.001), driven largely by a substantial improvement in T4 (–11.6 days; p < 0.001), with a small increase in T3 likely reflecting external payer processing dynamics under higher 2023 volumes. Together, the primary analysis pinpoints where navigation works (post-approval operations), and the sensitivity analysis shows that, over a full operational year with increasing referrals, these gains translate into a clinically meaningful reduction in overall time to therapy.
Although pCR rates were similar across cohorts, the slight favorable direction is clinically relevant given the strong association between pCR and improved long-term outcomes in HER2-positive disease [8, 18]. By reducing delays, navigation may lessen pre-treatment tumor growth and enhance chemosensitivity—mechanisms consistent with international evidence linking prompt care to better outcomes [9]. Navigation’s additional benefits—improved knowledge, communication, and adherence—are well documented and were reflected in our early implementation experience [9, 16].
These results align with the WHO Global Breast Cancer Initiative (GBCI) emphasis on timely diagnosis, streamlined referral pathways, and coordinated treatment in resource-constrained settings [15]. Embedding navigation within national cancer control plans, while digitizing tracking and inter-facility referrals, could further compress upstream intervals (T1–T2) and stabilize payer-facing timelines (T3) [13, 14, 17]. In publicly funded systems, navigation provides the operational glue that turns policy and coverage into timely, equitable access to evidence-based therapy.
In summary, the BCCC Patient Navigation Program produced a precise, measurable improvement in the most actionable segment of the pathway (T4) in the primary analysis and a significant reduction in total time to therapy over the full operational year. Consistent with international experience, navigation is a scalable, equity-promoting strategy for LMIC cancer centers progressing toward GBCI targets [9, 10, 12–15, 17].
Limitations
Our study has several limitations consistent with a before–after, retrospective design in health services research. First, without randomization or a concurrent control group, causal attribution to the Patient Navigation Program cannot be assured. Although we prespecified symmetric six-month windows for the primary analysis (July–December 2022 vs. January–June 2023) to improve comparability and used a full-year sensitivity analysis, secular trends and unmeasured confounding may persist (e.g., rising referrals from national early-detection activities, informal workflow refinements, or learning-curve effects).
Second, this is a single-center study from a large tertiary public cancer hospital in Egypt; the organizational context (e.g., staffing, MOH approval pathways, infusion capacity) may limit generalizability to smaller facilities or different provinces. Third, interval measurement relied on EMR timestamps and paper approvals. Despite double-checking and adjudication, residual measurement error is possible; exclusions for missing key dates may introduce selection bias.
Fourth, the study was not powered to detect modest differences in pCR and did not include time-to-event outcomes (recurrence, survival), patient-reported outcomes, or cost-effectiveness. pCR was assessed only among surgical cases with evaluable pathology, which may introduce attrition bias. Finally, we did not apply multivariable adjustment or quasi-experimental methods (e.g., interrupted time series, difference-in-differences) that could further address confounding by time-varying factors, detailed navigator metrics (staff numbers, caseloads, training hours, costs) were not prospectively collected.
Future work should include multi-center prospective designs, equity-focused subgroup analyses, Patient -Reported Outcomes (PROs), survival endpoints, cost-effectiveness, and implementation outcomes (acceptability, fidelity, reach).
Conclusion
In conclusion, the implementation of a Patient Navigation Program at our tertiary cancer center in Egypt significantly reduced treatment delays for HER2-positive early breast cancer, particularly by shortening the critical interval between MOH approval and initiation of dual anti-HER2 therapy. When examined across the full operational year, navigation achieved a meaningful reduction in overall time to treatment despite rising referral volumes, underscoring its capacity to deliver system-level efficiency gains in resource-constrained settings. While pCR rates were comparable, the timeliness gains are clinically important given the established association between prompt therapy and improved outcomes. These findings demonstrate that navigation is a practical, adaptable, and equity-promoting intervention aligned with global initiatives to strengthen cancer care in LMICs, and they provide a compelling rationale for continued implementation, scale-up, and prospective evaluation across similar health systems.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cortazar P, Zhang L, Untch M, Mehta K, Costantino JP, Wolmark N, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CT Neo BC pooled analysis. Lancet. 2014;384(9938):164–172. 10.1016/S 0140-6736(13)62422-810.1016/S 0140-6736(13)62422-824529560 · doi ↗ · pubmed ↗
- 2Broglio KR, Quintana M, Foster M, Olinger M, Mc Glothlin A, Berry SM, et al. Association of pathologic complete response to neoadjuvant therapy in HER 2-positive breast cancer with long-term outcomes: a meta-analysis. JAMA Oncol. 2016;2(6):751–60. 10.1001/jamaoncol.2015.611310.1001/jamaoncol.2015.611326914222 · doi ↗ · pubmed ↗