Vaccines as antimicrobial resistance control tools: evidence from pneumococcal conjugate vaccines in South Africa
Chinwe Iwu-Jaja, Akhona Victress Mazingisa, Anelisa Jaca, Chidozie Declan Iwu, Charles Shey Wiysonge

TL;DR
Vaccines, like pneumococcal conjugate vaccines in South Africa, can help reduce antimicrobial resistance by lowering drug-resistant infections.
Contribution
Demonstrates that pneumococcal vaccines significantly reduce resistant strains, offering a novel AMR control strategy in Africa.
Findings
Pneumococcal conjugate vaccines reduced drug-resistant pneumococcal infections by 67-96% in South Africa.
Vaccines offer a cost-effective way to combat antimicrobial resistance while reducing disease burden in Africa.
Abstract
The Expanded Programme on Immunisation demonstrated remarkable success for 50 years, accounting for 52% reduction in infant mortality in Africa. As antimicrobial resistance (AMR) continues to be a threat in Africa, responsible for 250,000 deaths in WHO African region in 2019, vaccines offer proven solutions. Studies from South Africa demonstrate that pneumococcal conjugate vaccines significantly reduced drug-resistant pneumococcal infections, with 67-96% reductions in resistant strains. Increasing immunisation coverage in Africa, reduces disease burden while providing a cost-effective strategy to combat antimicrobial resistance.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
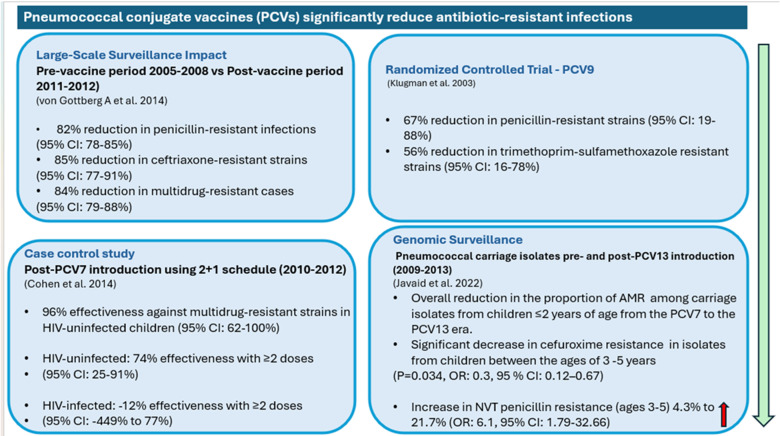 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPneumonia and Respiratory Infections · Immune responses and vaccinations · Influenza Virus Research Studies
Brief
The Expanded Programme on Immunisation (EPI), launched 50 years ago, has demonstrated unprecedented success in reducing mortality, averting 154 million deaths globally and accounting for 52% of the decline in infant mortality in the African region [1]. This remarkable achievement underscores the proven track record of vaccines as one of the most effective public health interventions in history. Antimicrobial resistance threatens to undermine decades of progress in fighting infectious diseases in Africa. Bacterial AMR directly caused 250,000 deaths in 2019 [2]. By 2050, bacterial AMR could result in up to 1.91 million annual deaths globally, disproportionately affecting the WHO African region [2]. Healthcare systems face mounting costs treating resistant infections, with longer hospital stays and higher mortality rates [3], particularly concerning in resource-limited settings where alternative antibiotics may be unavailable.
Building on EPI’s proven success, vaccines offer a complementary approach to addressing AMR, by preventing infections and reducing antibiotic use, thereby decreasing selection pressure for resistant organisms [4,5]. While various vaccines have demonstrated potential in addressing antimicrobial resistance (AMR), pneumococcal conjugate vaccines (PCVs) represent the most extensively studied intervention with the most robust available empirical evidence in Africa [6,7].
Streptococcus pneumoniae is a leading cause of pneumonia, meningitis, and bloodstream infections and deaths globally, with Africa bearing a disproportionate burden. PCVs have led to significant reduction of these diseases, particularly among children under five years [8]. More recently, their role in reducing antibiotic-resistant strains has gained attention. Given the pressing need to highlight the role of vaccines in curbing AMR for policy makers and stakeholders in immunisation and AMR space, this paper summarises the available evidence on the impact of PCV on AMR in Africa.
Evidence from South Africa demonstrates PCV’s impact on AMR through four key studies. These include a randomised controlled trial (RCT) [9], a case-control study [10], a clinical surveillance study [11], and a genomic surveillance study [12]. The RCT which was a study which assessed the efficacy of PCV9, demonstrated a 67% reduction in penicillin-resistant strains (95% CI: 19-88%) and 56% reduction in trimethoprim-sulfamethoxazole resistant strains (95% CI: 16-78%) [9]. The case-control study following PCV7 introduction (2010-2012) showed 96% effectiveness against multidrug-resistant strains in HIV-uninfected children (95% CI: 62-100%) [10]. The clinical surveillance study which compared pre-vaccine (2005-2008) and post-vaccine periods (2011-2012) showed significant reductions in resistant infections: 82% decrease in penicillin-resistant infections (95% CI: 78-85%), 85% reduction in ceftriaxone-resistant strains (95% CI: 77-91%), and 84% decline in multidrug-resistant cases of pneumococcal disease (95% CI: 79-88%) [11]. Lastly, the genomic surveillance revealed significant changes in resistance patterns between PCV7 and PCV13 eras [12]. Among children ≤2 years, substantial reductions were observed for several important antibiotic classes. Most notably, resistance to penicillin decreased from 55.5% to 41.8%, while cephalosporin resistance showed similar declines (cefuroxime: 9.9% to 3.2%; ceftriaxone: 6.4% to 1.5%). Significant reduction in cefuroxime resistance was also observed in children aged 3-5 years (OR: 0.3, 95% CI: 0.12-0.67, P=0.034). Furthermore, vaccine-type strains (those targeted by the vaccine formulation) showed stronger association with reduced resistance compared to non-vaccine types (strains that aren’t targeted by the vaccine formulation). However, among non-vaccine types, penicillin resistance significantly increased in children aged 3-5 years (4.3% to 21.7%, OR: 6.1, 95% CI: 1.79-32.66, P=0.02) [12]. These findings are summarised in Figure 1.
impact of pneumococcal conjugate vaccines on antibiotic resistance
The robust evidence from South Africa demonstrates that PCV significantly reduce antibiotic-resistant infections, providing the real-world evidence of vaccines’ potential in combating AMR. While emerging data from other vaccines, such as respiratory syncytial virus (RSV) and typhoid conjugate vaccines, show promise in reducing antibiotic use in Africa, the compelling evidence from PCV serves as a compelling example of the expanded value of vaccines. This evidence supports a paradigm shift in how we value vaccination programmes: not just as disease prevention tools, but as crucial and cost-effective interventions in addressing the global challenge of AMR.
For policy makers, these findings provide additional rationale for strengthening existing immunisation programmes and justify investment in vaccination as one of the core strategies for AMR control. Beyond preventing deaths, reduced AMR infections decrease healthcare costs through shorter hospital stays and reduced need for expensive second-line antibiotics. Investing in initiatives to improve vaccine uptake and coverage therefore offers a dual benefit: preventing infectious diseases while simultaneously tackling AMR. Priority actions should include integrating AMR impact assessment into immunisation programme evaluations alongside existing coverage improvement strategies. As novel vaccines enter the pipeline, their potential impact on AMR should be considered in policy decisions. In an era of dwindling global health financing, this dual-impact approach maximises the value of every health dollar spent on vaccination programmes.
In conclusion, as Africa celebrates 50 years of the Expanded Programme on Immunisation [13,14], the demonstrated success of PCV in reducing antibiotic-resistant infections exemplifies how immunisation programmes can address critical public health challenges like AMR while providing compelling evidence for strengthening vaccination programmes as a key strategy. Further research from other African countries and on additional vaccines is needed to build a more comprehensive evidence base.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Shattock AJ Johnson HC Sim SY Carter A Lambach P Hutubessy RC Wet al Contribution of vaccination to improved survival and health: modelling 50 years of the Expanded Programme on Immunization Lancet 20244032307163870515910.1016/S 0140-6736(24)00850-XPMC 11140691 · doi ↗ · pubmed ↗
- 2GBD 2021 Antimicrobial Resistance Collaborators Global burden of bacterial antimicrobial resistance 1990-2021: a systematic analysis with forecasts to 2050 Lancet 2024 Sep 2840410459119912263929926110.1016/S 0140-6736(24)01867-1PMC 11718157 · doi ↗ · pubmed ↗
- 3Global leaders Group on Antimcrobial Resistance Building the investment case for action against antimicrobial resistance 2024 March, Accessed 31 May 2025
- 4Bloom DE Black S Salisbury D Rappuoli R Antimicrobial resistance and the role of vaccines PNAS 201811512868713055920410.1073/pnas.1717157115 PMC 6305009 · doi ↗ · pubmed ↗
- 5World Health Organization Estimating the impact of vaccines in reducing antimicrobial resistance and antibiotic use:technical report Geneva 2024
- 6Doherty TM Hausdorff WP Kristinsson KG Effect of vaccination on the use of antimicrobial agents: a systematic literature review Ann Med 202052283993259723610.1080/07853890.2020.1782460 PMC 7880080 · doi ↗ · pubmed ↗
- 7Brink AJ Richards GA Use of vaccines as a key antimicrobial stewardship strategy South African Med J 20151054313
- 8Franklin K Kwambana-Adams B Lessa FC Soeters HM Cooper L Coldiron M Eet al Pneumococcal Meningitis Outbreaks in Africa, 2000-2018: Systematic Literature Review and Meningitis Surveillance Database Analyses J Infect Dis 2021224 S 174833446956110.1093/infdis/jiab 105PMC 8414910 · doi ↗ · pubmed ↗