Indirect cognitive mapping in glioma surgery in patients not eligible for awake craniotomy – how I do it
Patrick Vigren, Hans Lindehammar

TL;DR
This paper presents a surgical technique to map cognitive brain pathways in patients who cannot undergo awake brain surgery.
Contribution
A novel indirect method for cognitive mapping in glioma surgery when awake craniotomy is not possible.
Findings
Preoperative mapping of motor and subcortical structures helps identify cognitive pathways.
Subcortical motor mapping serves as a landmark for cognitive structures.
The method is demonstrated through three clinical cases.
Abstract
This paper illustrates a method to map cognitive subcortical white matter pathways in brain tumour surgery, in patients not eligible for awake intraoperative mapping. The latter being the gold standard, it is not feasible in all patients. Illustrated by three cases, the presented method includes a preoperative mapping of both motor and subcortical eloquent structures – such as arcuate fasciculus and basal ganglia – subsequentially using subcortical motor mapping as a landmark to indirectly identify the cognitive structures. The online version contains supplementary material available at 10.1007/s00701-025-06706-1.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
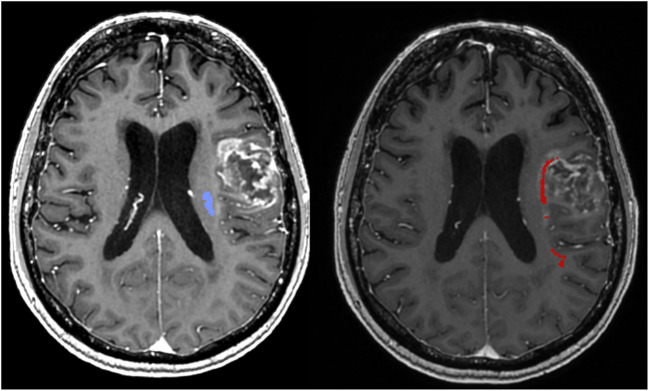 Figure 1
Figure 1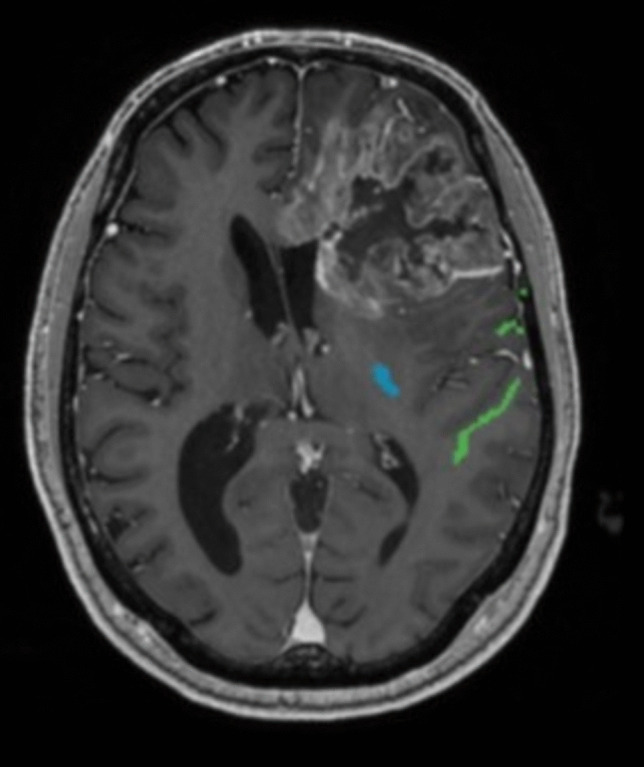 Figure 2
Figure 2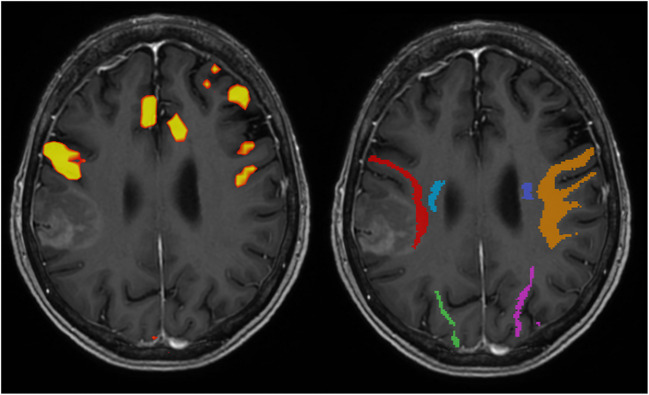 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdvanced Neuroimaging Techniques and Applications · Intraoperative Neuromonitoring and Anesthetic Effects · Glioma Diagnosis and Treatment