Safety and Efficacy of Stereotactic Magnetic Resonance-Guided Adaptive Radiation Therapy (SMART) for Ultracentral Metastases in Non-Small Cell Lung Cancer
Elena Moreno-Olmedo, Ben George, Kasia Owczarczyk, David Woolf, John Conibear, Andy Gaya, Joss Adams, Luis Aznar-García, Timothy Sevitt, Peter Dickinson, Kevin Franks, Alex Martin, Veni Ezhil, Philip Camilleri, James Good, Crispin Hiley

TL;DR
SMART radiation therapy safely and effectively treats hard-to-reach lung cancer metastases near critical organs.
Contribution
Demonstrates the safety and efficacy of SMART for ultracentral NSCLC lesions with daily plan adaptation.
Findings
No grade ≥ 3 toxicities were observed in 11 patients treated with SMART.
One-year freedom from local progression was 93% with a median overall survival of 20 months.
Daily online plan adaptation improved safety and local control compared to conventional SABR.
Abstract
Stereotactic ablative radiation therapy (SABR) is a standard of care for early-stage lung cancer and thoracic oligometastatic or oligoprogressive disease. However, ultracentral lesions remain challenging because of their proximity to critical mediastinal structures and the associated risk of severe toxicity. Stereotactic magnetic resonance-guided adaptive radiation therapy (SMART) allows for daily plan adaptation and real-time tracking in breath-hold, enhancing target coverage while improving sparing of adjacent organs compared to conventional SABR. This retrospective study analyzed outcomes of SMART-based SABR for ultracentral metastatic lesions in patients with histologically confirmed non-small cell lung cancer (NSCLC). Ultracentral lesions were defined by planning target volume overlapping with the proximal bronchial tree, esophagus, or pulmonary vessels. Endpoints included grade ≥…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
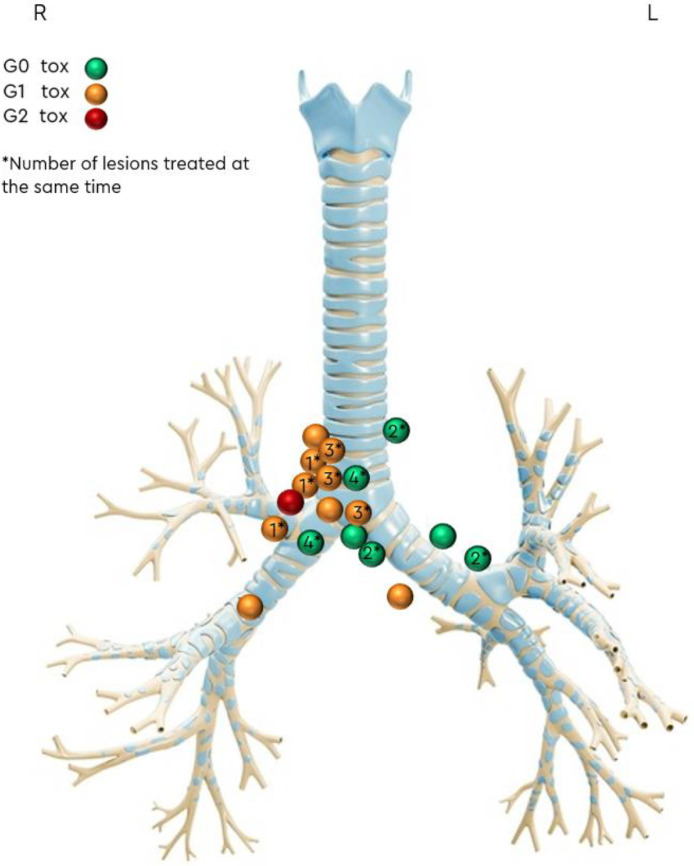 Figure 1
Figure 1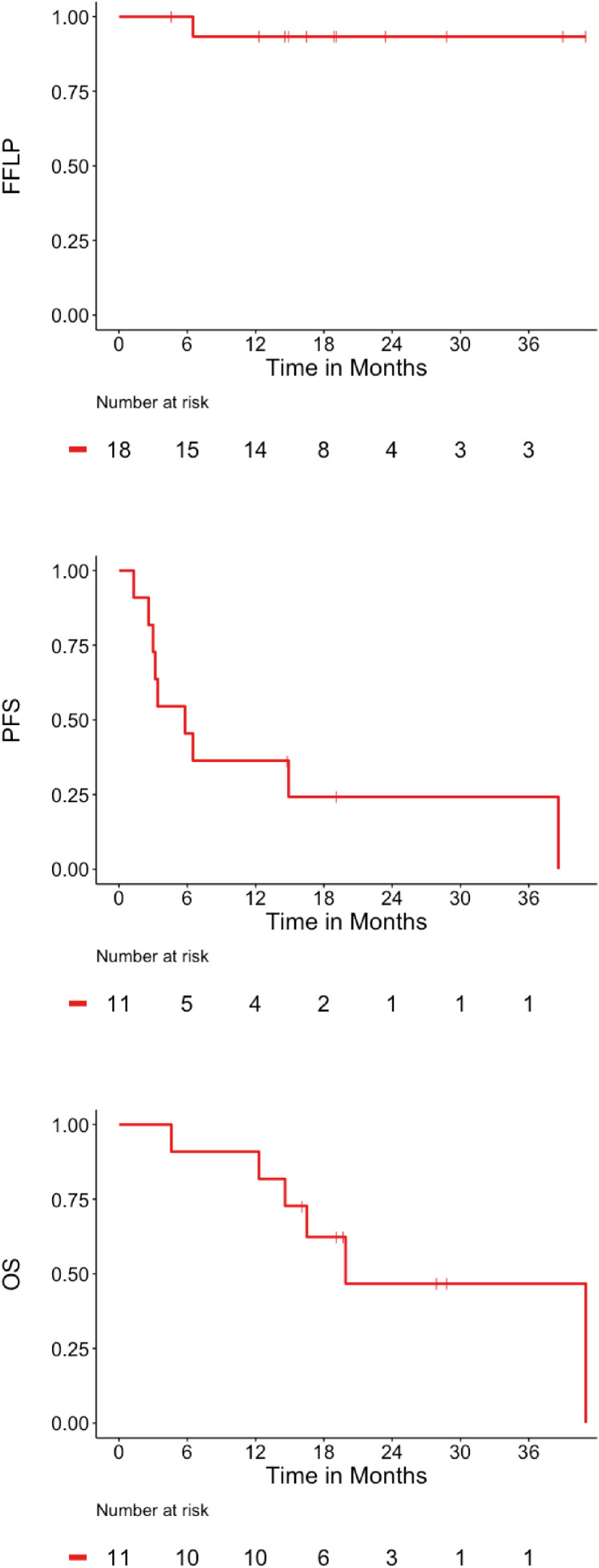 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdvanced Radiotherapy Techniques · Lung Cancer Diagnosis and Treatment · Medical Imaging Techniques and Applications
Introduction
For patients with non-small-cell lung cancer (NSCLC), stereotactic ablative body radiation therapy (SABR) is a standard of care for patients with early-stage cancer and for oligometastatic (OMD) or oligoprogressive disease (OPD).1, 2, 3
Although conventional SABR achieves excellent local control (LC), ultracentral tumor location makes the delivery of a safe effective treatment challenging. Contemporary series of nonadaptive conventional SABR for ultracentral tumors report LC rates of 83% to 90% at 2 to 3 years but at the expense of 7% to 34% of ≥G3 toxicity.4, 5, 6, 7 Stereotactic magnetic resonance-guided adaptive radiation therapy (SMART) enhances treatment precision. Daily online volume adaptation and plan reoptimization accounts for changes in tumor size and position relative to organs at risk (OARs). Real-time imaging permits treatment in breath-hold with automated gated beam delivery which eliminates the need for an internal target volume (ITV).
Current evidence for the benefit of SMART for ultracentral tumors is encouraging but is determined from cohorts of patients with heterogeneous primary cancer diagnoses.8, 9, 10, 11, 12, 13, 14, 15 Differences in tumor biology and systemic therapy regimes, in a heterogeneous cohort, may confound assessment of safety. We present our institution's experience of daily-SMART for ultracentral tumors, from a homogeneous cohort of patients with a primary diagnosis of NSCLC.
Methods and Materials
Study design and population
This single institution retrospective analysis assessed the safety and efficacy of SMART in ultracentral metastatic lesions from patients with histologically proven NSCLC. All patients provided written consent and were assessed by a tumor board. Ultracentral tumors were defined as any parenchymal lesion or lymph node whose PTV overlapped the proximal bronchial tree (PBT), esophagus or pulmonary vessels. OMD included ≤5 disease sites and OPD ≤ 3 progressing disease sites. Systemic therapy (ST) was held before SABR to avoid interactions with concurrent treatment.
The primary objective of this study was to assess the incidence of SABR related acute (<3 months) and late (>3 months) toxicity, graded according to the Common Terminology Criteria for Adverse Events version 5.0. A secondary objective was to evaluate time-to-event outcomes, measured from the first day of SMART. Freedom from locoregional progression (FFLP) was defined as the absence of progressive lung cancer within or adjacent to the radiation therapy field. Patients were censored at the time of death from distant metastases or at the last follow-up if alive without evidence of locoregional failure. Progression-free survival (PFS) was defined as the time from SMART initiation to the first occurrence of disease progression (locoregional or distant) or death from any cause. Patients lost to follow-up were censored at the date of last contact. Overall survival (OS) was defined as the time from SMART initiation to death from any cause, with patients lost to follow-up censored at the date of last known survival.
SMART planning and delivery
Simulation consisted of a 0.35T magnetic resonance imaging (MRI) true fast imaging with steady-state free precession sequence and a computed tomography (CT) image. Simulations were performed in breath-hold at the same respiratory phase. The CT was deformably registered to the magnetic resonance (MR) to provide electron density information for dose calculation. A suitable tracking structure was identified through cine MR imaging to permit gated treatment. Contouring of gross target volume (GTV) and OARs was in concordance with national and international guidelines with mandatory peer review.16 The PTV margin was a 3-mm axial expansion and a 3- to 6-mm superior/inferior margin from the GTV.
A 6-MV photon fixed field SABR plan was generated with inverse planning with the following dosimetric aims: PTV V100% ≥ 95%, PTV V95 ≥ 98%, Dmax(0.1cc) ≥ 110% and ≤ 140%, with hotspots inside the GTV. PTV coverage was compromised, when necessary to meet OAR constraints with a minimum PTV V100% ≥ 70% required. SABR was delivered on a 6 MV 0.35T MRIdian (ViewRay Systems, MRIdian). A daily onset breath-hold MRI true fast imaging with steady-state free precession sequence scan was acquired for consideration of online adaptation. The contours (GTV and OARs within a 3-cm distance from PTV) were adapted daily. Plan optimization was performed to meet planning objectives and mandatory OAR constraints for each individual fraction.16 SABR was delivered with gated delivery during repeated breath-holds under continuous MR-guidance.
To estimate the reduction in PTV volume and overlap with OARs from SMART in breath-hold compared to conventional SABR with 4-dimensional CT, motion was simulated on the adaptive MR-Linac planning scan for each tumor. The mean range of motion in the superior-inferior, anterior-posterior, and left-right axis was applied as reported by the management of respiratory motion in radiation oncology report of American Association of Physicists in Medicine Task Group.17 A standard GTV-PTV margin expansion of 5 mm was then applied.
Institutional follow-up assessment was conducted 7 to 10 days after treatment. Further follow-up at our institution was not mandated but safety and efficacy outcomes were obtained from the referring oncologist.
Statistical analysis
The Kaplan–Meier method was used to estimate FFLP, PFS, and OS, with a log-rank test for subgroup comparisons. The reverse Kaplan–Meier method was used to estimate the median follow-up duration, accounting for censoring. Paired t tests were used to assess the difference in PTV overlap with OARs between the conventional and adaptive approaches. Kruskal–Wallis test with post hoc pairwise comparisons using the Dunn's test was used for any other analyses.
Results
Between September 2020 and August 2023, 11 patients with a histologically confirmed NSCLC received daily-SMART to treat a total of 18 thoracic lesions (Table 1). All patients had metastatic disease. Prior to SMART 4 patients had received a tyrosine kinase inhibitor for an actionable genomic alteration, 1 patient had received a tyrosine kinase inhibitor and chemotherapy, 2 patients had received immunotherapy, 1 patient had received chemotherapy, and 3 patients had not received any prior therapy in the metastatic setting (Table S1). During the peri-SMART period, the median time off-ST was 0.6 months prior SMART and 0.75 months following the last fraction.Table 1. Demographics and clinic characteristicsTable 1 Patients (lesions)11 (18) Age, median (range) y67 (46-82)Gender, n (%) Male2 (18) Female9 (82)Lesion Type, n (%) Lung parenchyma2 (11) Lymph node16 (89)History of metastatic disease before SMART, n (%) No3 (27) Yes8 (73) Thoracic metastasis2 (18) Extra-thoracic metastasis6 (55)Histology subgroup, n (%) Adenocarcinoma8 (73) Large cell neuroendocrine3 (27)**Ultracentral overlap, n (%)**per lesions PBT7 (39) PBT + pulmonary vessels6 (33) PBT + esophagus1 (6) Pulmonary vessels2 (11) PBT + pulmonary vessels+ esophagus2 (11)Abbreviation: PBT = proximal bronchial tree; SMART = stereotactic magnetic resonance-guided adaptive radiation therapy.
A summary of the dose prescriptions, targets volumes and dose coverage is presented in Table 2. The median SMART PTV volume overlapping the ultracentral OARs was 0.85 cm^3^ (8.4% of the PTV; range, 0.09-3.30 cm^3^). To meet OAR constraints 74% of tumors had prescriptions with BED_10_ < 100 Gy with a median PTV V100(%) of 92.5%.Table 2. Treatment and dosimetric parametersTable 2Treatment prescriptions, median (range) Dose prescribed, Gy40 (30 - 60) Dose prescribed BED_10_, Gy60 (48 – 105) Fractions prescribed8 (5-8)Fractions delivered and adapted73 (100%)SMART fractionation schedules, n per lesion (%) 30 Gy/5#4 (22.2) 40 Gy/5#4 (11.1) 40 Gy/8#5 (38.9) 50 Gy/8#1 (5.6) 60 Gy/8#4 (22.2)Baseline SMART plan dosimetry, median (IQR) GTV volume, cc2.7 (11.2) PTV volume, cc10.1 (23.7) PTV V100(%), cc9.7 (23.8) PTV V100(%), %92.5 (17.7)Gy****BED10 Gy PTV D(99%)34.3 (9.2)49.1 (11.5) PTV D(98%)35.4 (9.7)51.7 (11.8) PTV D(95%)38.5 (10.0)57.2 (12.8) PTV Dmax, %141.7 (2.4) PTV D(50%), Gy47.7 (13.4) Prescription Dose Spill1.2 (0.1) Modified gradient index6.6 (3.9)Target volume and ultracentral organ at risk overlap, median (IQR) SMART PTV volume, cc10.1 (23.7) Conventional-SABR PTV volume, cc30.4 (23.7) SMART PTV overlap, cc0.85 (0.9) Conventional-SABR PTV overlap, cc4.7 (3.2)Organ at risk doses, median (IRQ)GyEQD2 α/β = 3 Esophagus D(0.1 cc)27.1 (15.3)34.6 (33.6) Esophagus Dmax30.6 (16.6)41.8 (38.9) Proximal bronchial tree D(0.1 cc)33.5 (11.4)62.7 (37.3) Proximal bronchial tree Dmax37.1 (12.3)68.4 (38.9) Lungs minus GTV V(20 Gy), %1.8 (7.3) Lungs minus GTV V(5 Gy), %22.1 (17.4) Lungs minus GTV D(mean), Gy3.2 (3.7)Abbreviations: α/β = alpha/beta ratio; BED = biological effective dose; CTV = clinical target volume; EQD2 = equivalent dose in 2 Gy fraction; GTV = gross target volume; IQR = interquartile range; LR = left-right; PA = posterior-anterior; PTV = planning target volume; SABR = stereotactic ablative radiation therapy; SI = superior-inferior; SMART = stereotactic magnetic resonance-guided adaptive radiation therapy.Conventional-SABR PTV = created as [gross target volume + (0.8 cm SI + 0.4 cm PA + 0.4 cm LR) = CTV] + 0.5 cm isotropic expansion.
The cumulative incidence of acute and late grade 1 to 2 toxicity was 54% and 18%, respectively. No grade 3 to 5 acute or late toxicities were reported (Table 3). Figure 1 represents the location of each lesion in relation to the PBT, graded by maximum reported toxicity and indicating those treated synchronously.Table 3. Toxicity according to CTCAE v5Table 3**Acute, n (%)**6 (54.5)G15 (45) Fatigue4 (36) Cough1 (9) Dysphagia1 (9) Breathlessness on exertion1 (9)G21 (9) Nausea/Vomiting1 (9)G3-50 (0)**Late, n (%)**2 (18)G1 Breathlessness on exertion2 (18)G3-50 (0)Abbreviation: CTCAE = Common Terminology Criteria for Adverse Events.Figure 1. Distribution of each lesion location in relation to the PBT, graded by maximum reported toxicity and indicating those treated synchronously.Abbreviation: PBT = proximal bronchial tree.Figure 1
With a median follow-up of 28 months (range, 5 - 41 months), 1 lesion recurred within the SMART field. In this case the volume of overlap of the PTV with the left PBT and pulmonary vessels was 7.6 cm^3^. Consequently, the PTV coverage was compromised to meet OAR constraints, resulting in a PTV V100(%) of 71%. The 12-month FFLP rate was 93%. Intrathoracic but out of field recurrence was the primary pattern of failure in this cohort (42%), whereas 25% of the cohort had a distant relapse. Median PFS was 6 months (range, 1-39 months). Median and 1-year OS was 20 months (range, 5-41 months) and 91%, respectively (Fig. 2). These data are presented in the context of recently published studies on ultracentral lesions (Table 4).4, 5, 6, 7^,^10^,^12, 13, 14, 15Figure 2. Kaplan–Meier function for freedom from local progression (FFLP), progression-free survival (PFS), and overall survival (OS). P values indicate a log-rank analysis between groups.Figure 2. Table 4Key outcomes compared to the most relevant reports of ultracentral tumoursTable 4Platform/ RMMAdaptive approach, MRI-Linac (MRIdian®) Tracking, GatingNon- Adaptive approach, CT-based 4D-CT/ITVCurrent cohortSMART Phase I (10)Sandoval (12)Regnery (14)Dana-Farber (13)La Rosa (15)HILUS (6)SUNSET (4)Sunnybrook (5)LUSTRE Phase 3** (7)UC definitionPTV overlaps/touch PBT and/or oesophagus and/or pulm vesselsGTV abutting mainstem bronchi, carina, or mediastinumPer the HILUS trial definitionPTV overlapsPBT or oesophagusGTV abutting PBT, oesophagus and/or great vesselsPTV overlapsTrachea, mainstem bronchi or oesophagus1cm from PBT (GroupA)≤1cm from lobar bronchi (GroupB)PTV overlaps/touch PBT and/or oesophagus and/or pulm vesselsPTV overlap/touch PBT and/or oesophagusCentral 1 cm of mediastinum or 2 cm of PBT (No provide UC definition)**Patients† (lesions)*12 (19)526 (A)12 (B)1618 (19)1329 (group A)30154 (162)45(*central +SABR)HistologyNSCLC(primary/mets)NSCLC (OMD/inoperable)MixMix(OMD/primary NCLCMix(OMD/OPD)Mix(primary/mets)Mix(78% NSCLC)Primary NSCLCMixPrimary NSCLC (inoperable)**Dose regimens, Gy/#**40/8 (30-60/5-8)(BED_10_ 48-105)50/5(BED_10_ 100)60/8 (50-60/5-15)(BED_10_ 75-105)50-60/10(BED_10_ 75-90)50/5 (35-60/5)60/1556/8(BED_10_ 95.2)60/8(BED_10_ 105)30-55 Gy/5(BED_10_ 48-115)60/8(BED_10_ 105)**Survival Parameters *(calculate from SABR)*****OS, Median, %15m1y: 80%1y:60%1&2yGroupA: 89GroupB:81 & 762y 63%1y-75 %, 2y-66 (no distinction central vs UC)NR1y 81; 2y 583y 72.544m1y 78%; 2y 67%1y 95; 2y 78LC, %**94.7%1y: 802y:84;3y:78groupA:2y:91; 3y:812y 931y 94; 2y 86%6m: 92.3%85 (1y); 83 (2 and 3y)89.6 at 3y95.2(2y 89%; 3y 86%87.6% 3y(no distinction central vs UC)**G3-5 toxicity, %**0%20(1 patient G3)4.3% (G3)(no distinction by groups)19%no death-related0%0%33.8 (15.4% death-related)6.7 (3y)1y 6.7%, 2y 8.4%; 3y 9.4%13 (1 G5 in UC lesion)Abbreviations: BED: Biological Equivalent Dose (alpha/beta of 10);ITV: Interval Target Volume; LC: Local Control; Linac: linear accelerator; LPFS: Local Progression Free Survival; MRIdian®=6 MV 0.35T MRI-Linac ViewRay Systems^;,^NR: no reported, OS: NSCLC: Non-Small Cell Lung Cancer; Overall Survival; PBT: Proximal Bronchial Tree; PFS: Progression Free Survival; PTV: Planning Target Volume; RMM: respiratory motion management; SABR: Stereotactic Ablative Radiation Therapy; UC: Ultracentral.#fractions, y: year(s).†Only UCs number expressed.**LUSTRE trial no specified number neither definition nor stratified outcomes per UC lesions.
The median simulated conventional-SABR PTV was significantly larger than the SMART PTV (30.4 cm^3^ vs 10.1 cm^3^, P < .001), with a significant increase in the median volume of overlap with ultracentral OARs (4.7 cm^3^ vs 0.85 cm^3^, P < .001) (Table 2). Furthermore, when applying the simulated conventional-SABR PTV, 6 lesions overlapped with an additional ultracentral OAR compared to the SMART PTV.
Discussion
Our study sought to highlight the promising outcomes and safety profile of SMART in the treatment of a cohort of patients all with a histologic diagnosis of NSCLC and ultracentral thoracic metastases. With a median follow-up of 28 months, SMART demonstrated both excellent LC and a low toxicity profile. This compares favorably with nonadaptive SABR series, which have reported severe toxicity rates, including treatment-related deaths, ranging from 7% to 34% for ultracentral tumors.4, 5, 6, 7^,^18 The absence of grade 3 to 5 acute or late toxicities and the low incidence of acute grade 1 to 2 toxicity (54% and 18%, respectively) underscores the safety of SMART in breath-hold with gated beam delivery in this high-risk cohort. Additionally, mandatory peer review of target and OAR volumes, and acceptance of PTV coverage compromise to respect OAR constraints, likely contributed to these favorable safety outcomes. Despite individualized prescription doses to meet nationally agreed OAR constraints for mediastinal structures, our analysis demonstrated LC rates comparable to conventional nonadaptive SABR studies.4, 5, 6, 7 The observed median OS of 20 months is encouraging, particularly given that 73% of patients had a history of metastatic disease prior to SMART and underscores the importance of careful patient selection for metastasis directed therapy in multidisciplinary tumor board discussions.
Previous dose–response modeling has shown a significant correlation between PTV overlap with the mainstem bronchus or trachea and grade ≥ 3 toxicity.18 By employing breath-hold delivery with automated beam gating, SMART obviates the need for an ITV and permits smaller PTV margins. Real-time MR imaging enables continuous monitoring during breath-hold and allows for immediate detection of intrafractional tumor drift, ensuring that beam delivery is automatically paused if the target moves outside the defined gating boundary.19
Our data showing reduced PTV overlap with ultracentral OARs compared to simulated conventional-SABR PTVs are consistent with prior findings.20 These results suggest that daily adaptive radiation therapy with breath-hold, using SMART, may broaden the therapeutic window for patients with lung tumors, enabling an isotoxic treatment approach while maintaining or improving target coverage. Both daily adaptive planning and breath-hold delivery with real-time gated beam control are integral components of SMART, each contributing to motion management and dose optimization, and likely playing complementary roles in achieving the favorable toxicity profile observed in this study.
It should be noted that our cohort consisted predominantly of patients with OMD or OPD, whereas many published nonadaptive conventional SABR series primarily included patients with early-stage primary lung cancer. The competing risk of death from systemic progression in our population may confound LC outcomes, and comparisons to early-stage cohorts should therefore be interpreted with caution. We acknowledge several limitations in our study, including its retrospective design, small cohort size, and relatively limited median follow-up. Although the median follow-up was 28 months, late toxicities related to stereotactic radiation therapy may emerge beyond 2 years, and longer observation periods may be necessary to fully capture such events. Additionally, the inclusion of a large proportion of patients referred from external centers introduces heterogeneity in ST timing, follow-up imaging, and toxicity reporting, representing a potential source of bias.
Conclusions
Our analysis demonstrates that hypofractionated SMART with daily online adaptation for ultracentral NSCLC achieved comparable LC to conventional nonadaptive SABR, with a safer toxicity profile. These findings support the consideration of SMART as a safer and effective treatment option for this challenging subgroup of thoracic tumors.
Disclosures
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ball D.Mai G.T.Vinod S.Babington S.Ruben J.Kron T.Stereotactic ablative radiotherapy versus standard radiotherapy in stage 1 non-small-cell lung cancer (TROG 09.02 CHISEL): a phase 3, open-label, randomised controlled trial Lancet Oncol 2020194945033077029110.1016/S 1470-2045(18)30896-9 · doi ↗ · pubmed ↗
- 2Gomez D.R.Tang C.Zhang J.Local Consolidative therapy vs. maintenance therapy or observation for patients with oligometastatic non-small-cell lung cancer: Long-term results of a multi-institutional, phase II, randomized study J Clin Oncol 372019155815653106713810.1200/JCO.19.00201 PMC 6599408 · doi ↗ · pubmed ↗
- 3Tsai C.J.Yang J.T.Shaverdian N.Standard-of-care systemic therapy with or without stereotactic body radiotherapy in patients with oligoprogressive breast cancer or non-small-cell lung cancer (Consolidative Use of Radiotherapy to Block [CURB] oligoprogression): an open-label, randomised, controlled, phase 2 study Lancet 40320241711823810457710.1016/S 0140-6736(23)01857-3PMC 10880046 · doi ↗ · pubmed ↗
- 4Giuliani M.E.Filion E.J.Faria S.Stereotactic radiation for ultra-central non-small cell lung cancer: A safety and efficacy trial (SUNSET)Int J Radiat Oncol Biol Phys 1182024 e 210.1016/j.ijrobp.2024.03.05038614279 · doi ↗ · pubmed ↗
- 5Li G.J.Tan H.Nusrat H.Safety and efficacy of stereotactic body radiation therapy for ultra-central thoracic tumors: A single center retrospective review Int J Radiat Oncol Biol Phys 12020243593693862160710.1016/j.ijrobp.2024.04.009 · doi ↗ · pubmed ↗
- 6Lindberg K.Grozman V.Karlsson K.The HILUS-trial—a prospective Nordic multicenter phase 2 study of ultracentral lung tumors treated with stereotactic body radiotherapy J Thorac Oncol 162021120012103382328610.1016/j.jtho.2021.03.019 · doi ↗ · pubmed ↗
- 7Wu C.H.D.Wierzbicki M.Parpia S.Toxicity in patients receiving radiotherapy for ultracentral stage I non-small cell lung cancer: A secondary analysis of the LUSTRE randomized trial Radiother Oncol 202202511060510.1016/j.radonc.2024.11060539481606 · doi ↗ · pubmed ↗
- 8Finazzi T.Palacios M.A.Spoelstra F.O.B.Role of on-table plan adaptation in MR-guided ablative radiation therapy for central lung tumors Int J Radiat Oncol Biol Phys 10420199339413092836010.1016/j.ijrobp.2019.03.035 · doi ↗ · pubmed ↗