Vascular complications related to Le Fort I osteotomy: a scoping review
Luiza Clertiani Alves, Joana Maria Alves, Ariana Maria Soares, Delane Gondim

TL;DR
This review summarizes the vascular complications that can occur during Le Fort I osteotomy, a facial surgery, and highlights the need for careful surgical technique and multidisciplinary care.
Contribution
The study provides a comprehensive overview of vascular complications associated with Le Fort I osteotomy through a scoping review.
Findings
Pseudoaneurysm was the most common vascular complication observed.
Surgical trauma primarily affects the internal maxillary artery and its branches.
Complications often arise from incisions involving the pterygomaxillary junction and nasal cavity.
Abstract
Le Fort I (LFI) osteotomy represents a secure procedure employed for correcting facial deformities and may be coupled with other facial osteotomies. However, notwithstanding professional proficiency, this technique is not exempt from issues or morbidities. Therefore, the objective of this study was to relate the types of vascular complications associated with LFI. A scoping review was conducted with published articles up to April 2024 sourced from PubMed, LILACS, EMBASE, Scopus, Web of Science, Cochrane Library and Google Scholar. The analyzed data comprised: i) comprehensive details pertaining to each vascular lesion associated with LFI; and ii) pertinent anatomical characteristics along with their implications. A total of 2,415 papers were identified. After removing duplicates and applying the inclusion and exclusion criteria, 33 studies were selected. All included patients had…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
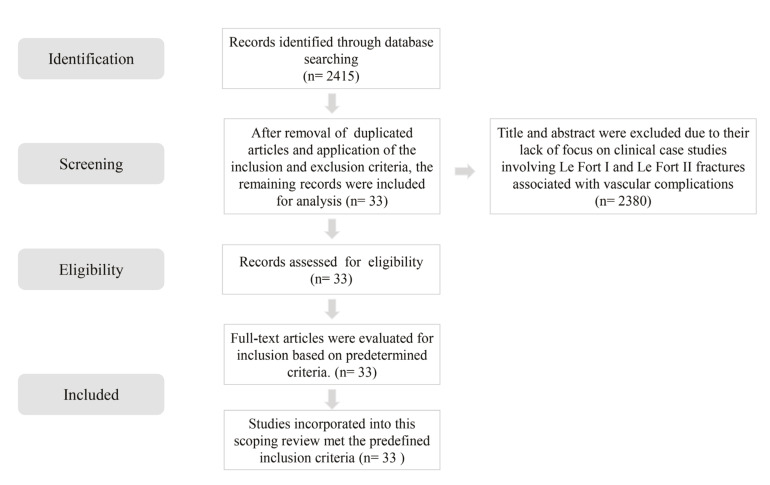 Figure 1
Figure 1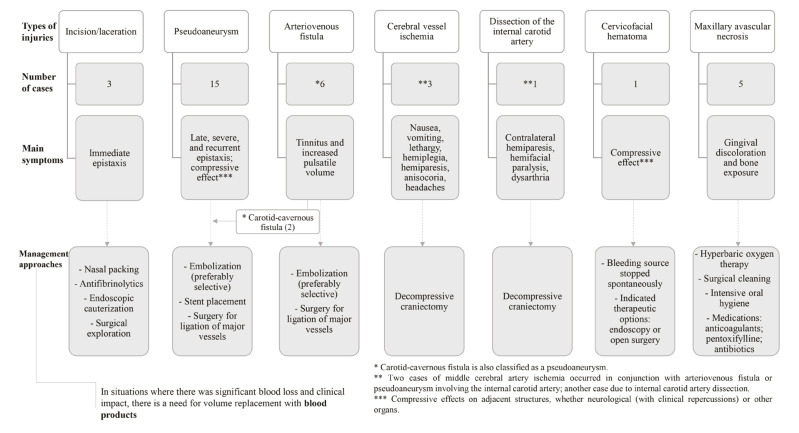 Figure 2
Figure 2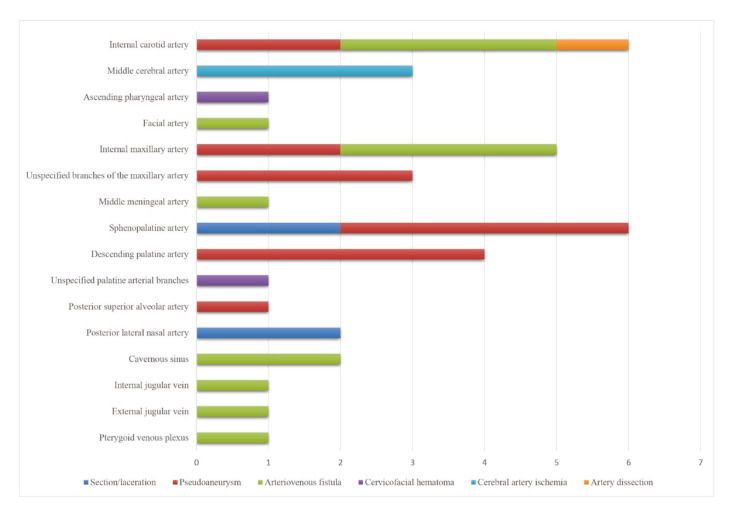 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone Tumor Diagnosis and Treatments · Hypertrophic osteoarthropathy and related conditions · Cerebrovascular and Carotid Artery Diseases
Introduction
The Le Fort I (LFI) fracture pattern, first described by Rene LeFort in 1901 and initially indicated for accessing skull base tumors, was first used in the context of facial orthopedics by Wasmund in 1921. The current LFI osteotomy standard consists of cutting the maxillary bone from the lateral wall of the nasal cavity, breaking the nasal bone septum, to the pterygomaxillary junction (PTJ), allowing the maxilla to move in all three planes, as well as correcting hypoplasia of the middle third of the face, vertical excess of the maxilla and dentofacial asymmetry (1,2).
The LFI osteotomy is considered a safe, efficient and predicTable procedure, and most of the complications are reversible and without permanent sequelae. However, it is not free of serious complications with risk of death (1,3). In this case, vascular complications have been reported during and after this type of osteotomy, appearing as excessive bleeding, compressive effects and blood flow changes (4).
Due to the severity of some of these complications and ethical issues, research and reports may be underestimated and there are no studies showing the compilation of information. For this, the data about the types of possible vascular complications involved, and their prevalence and management must be assessed, as well as the most affected blood vessels and the most likely causal factors. In addition, maxillofacial surgeons must recognize the potential complications associated with the procedure, and the initial symptomatology and course of the lesion, aiming at the early management of these alterations and thus avoiding severe and irreversible outcomes.
Material and Methods
-Protocol and registration
This scoping review was based on the five-step methodology proposed by Arksey and O’Malley and followed the PRISMA Extension for Scoping Reviews (PRISMA-ScR) (5,6).
- Research question
The starting question was: "What types of vascular complications are associated with LFI osteotomy?" and it was registered under https://osf.io/s5mu6.
- Identification of relevant studies
The literature search was performed in PubMed, LILACS, EMBASE, Scopus, Web of Science, Cochrane Library, and Google Scholar databases for articles published up to April 2024, using medical term descriptors (MeSH) matched by the Boolean operators "OR" and "AND": “Osteotomy, Le Fort” OR “Le Fort Osteotomy” OR “LeFort Osteotomy” OR “Le Fort I Osteotomy” OR “Maxillary expansion” OR “Rapid maxillary expansion” OR “Maxillary surgery” OR “Maxillary osteotomy” OR “Maxillary advancement” AND “ischemia” OR “osteonecrosis” OR “Bone necrosis” OR “Bone aseptic necrosis” OR “Bone avascular necrosis” OR “Carotid-Cavernous Sinus Fistula” OR “Carotid Artery Diseases” OR “Cavernous Sinus Fistula” OR “Epistaxis” OR “Nosebleed” OR “Nasal bleeding” OR “Nose bleeding” OR “Hemorrhage” OR “Bleeding” OR “Aneurysm, False” OR “Vascular injury” OR “False aneurysm” OR “Vascular complication” OR "Maxillary Artery" OR "Ophthalmic Artery" OR "Arteries" OR "Veins".
- Study selection
The standard descriptors used in the search strategy were selected to identify descriptive studies of complications associated with LFI osteotomy. The elements of the study question included: Participants (P) = patients with dentofacial deformity or skull base lesions who underwent LFI osteotomy; Exposure (E) = vascular complications related to LFI; and Outcomes (O) = prevalence of vessel injuries, clinical and surgical management, sequelae, and prevention methods.
Inclusion criteria: Case reports and case series involving vascular complications in the middle third of the face following LFI osteotomy, with or without other procedures on the gnathic bones. The selected publication period was the last 21 years up to April 2024, with no language restrictions.
Exclusion criteria: Studies unrelated to the subject; unavailability of the full text; and patients with blood dyscrasias or those using medication that directly affects the blood coagulation system.
The selection process was conducted in two phases: Phase 1 - two researchers (LCVA and JMSA) independently reviewed the titles and abstracts of all identified references, applying the inclusion criteria in a blinded process; Phase 2 - the same reviewers independently applied the exclusion criteria to the remaining studies based on full-text reading, also blinded. Inter-rater reliability during the study selection was determined by the Cohen kappa test, with a satisfactory value of 0.85. Any disagreements at any stage were resolved through discussion with a third reviewer (DVG). The final decision was always based on the full text of the published studies.
- Data collection
The full texts were carefully evaluated. Data from the eligibility forms were stored in Tables using an independent method by LCVA, JMSA, and AMSS. The validation process was conducted by a fourth reviewer (DVG).
- Compilation, summarization, and reporting of results
After data extraction, the findings were presented using a narrative report divided into two main sections: individualized information about the course of vascular injuries associated with LFI osteotomy as described in each report; and the relevance of surgical anatomy and its implications. The following data related to the characteristics and course of the injuries were extracted and detailed in a Table (Table 1): authors and year of publication, type of study, affected blood vessels, signs and symptoms, time between the procedure and onset of symptoms, type of vascular injury, probable cause, and management.
Results
The initial search retrieved 2,415 articles. After removing duplicates and applying the inclusion and exclusion criteria, a total of 33 articles were selected for analysis (Fig. 1).
The final sample included 41 patients who underwent LFI osteotomy. The female-to-male ratio was 18:22, and the mean age was 26 years, ranging from 14 to 52 years. Most patients had no significant past medical history.
All patients presented with dentofacial deformities requiring correction of the midfacial third. Reported conditions included Angle Class II or III malocclusion, maxillary atresia, facial asymmetry, vertical maxillary excess, and hypoplasia secondary to cleft lip and palate. Maxillary movements were performed to address these deformities, including segmentation, expansion, intrusion, extrusion, advancement, and setback.
The vascular complications reported in the selected articles were as follows: pseudoaneurysm (3,4,7,8,9-19); arteriovenous fistula (20-25) laceration (26,27); partial vascular necrosis (28-32); and total vascular necrosis (33). Additionally, one case of cervicofacial hematoma (34) and one case of internal carotid artery dissection (35) were reported.
The vessels most frequently associated with these complications were the sphenopalatine artery (4,7,10,16,18,27,28), followed by the internal carotid artery (8,17,20,21,35).
Detailed information regarding the characteristics and clinical course of these injuries is presented in Table 1, and a graphical summary was generated for quantitative visualization (Fig. 2, Fig. 3).
Figure 1. Flowchart of the electronic search.
Figure 2. Main vascular injuries associated with Le Fort I osteotomy procedure and their management.
Figure 3. Primary blood vessels affected during the Le Fort I osteotomy procedure.
Discussion
Deformities of the maxillofacial skeleton are usually corrected through orthognathic surgery, involving the mobilization of the gnathic bones. LFI osteotomy is is a widely performed and generally safe procedure for correcting midfacial discrepancies and may be combined with other surgical techniques. Despite the expertise of the surgical team, the procedure is not without risks. Although complications are rare and, in most cases, reversible, they must be carefully considered (4,7,33).
Complications from orthognathic surgery may present in the short or long term—occurring hours, days, or even weeks postoperatively—depending on the nature of the injury. The most severe complications involve vascular structures and may be life-threatening, regardless of whether they are of arterial or venous origin. In our review, pseudoaneurysm was the most frequently reported vascular complication (3,4,7-19). We believe this frequency in the literature reflects both their clinical relevance and rarity, which prompts publication for educational purposes and to discuss diagnostic and therapeutic strategies.
Epistaxis may occur immediately or at a delayed stage, manifesting as isolated or recurrent episodes, with bleeding ranging from mild to severe (3-5, 7,9-11,13-16,18,26-28,36). Recognizing these patterns helps guide diagnostic suspicion. Direct vascular injuries, such as lacerations, typically cause immediate bleeding, while pseudoaneurysms often develop later, days to months postoperatively, and are frequently associated with recurrent nasal bleeding. Pseudoaneurysms of small branches in deep facial regions, such as terminal branches of the maxillary artery, are rare. Moreover, partial injuries involving only one or two layers of the vessel wall (excluding simultaneous involvement of the intima, media, and adventitia) are also uncommon (7,34,37).
Lesions such as pseudoaneurysms, arteriovenous fistulas, and hematomas can be clinically significant and costly to manage. Even when located in deep anatomical planes and not externally visible, they may compress surrounding structures. Depending on their location, this compression can result in serious symptoms including cranial nerve deficits, ocular disturbances, airway obstruction, central nervous system involvement, or altered cerebral perfusion, leading to signs such as lethargy, dysarthria, hemiparesis, facial paralysis, nausea, and headache (8,9,15,20,21,34,35).
One particularly relevant complication is cervicofacial hematoma, as described by Bertossi et al. (2012) (34). It was observed on the first postoperative day after a Le Fort I osteotomy and led to upper and lower airway compression, requiring urgent medical intervention. This highlights the critical importance of continuous postoperative monitoring for the early detection and management of potential
Among diagnostic tools, arteriography was the most frequently employed and effective for identifying pseudoaneurysms and arteriovenous fistulas. When clinical signs suggest vascular lesions, early arteriographic evaluation is recommended due to the unpredicTable course and rupture risk of such injuries. Selective arterial embolization is considered the first-line treatment, as it is minimally invasive, effective, and preserves the vascular architecture more effectively than surgical interventions like vessel ligation (7,10,11,37).
Arteriovenous fistula was the second most frequently reported vascular complication in our review (20-25). Its potentially progressive nature and risk of hemodynamic instability necessitate early detection. Most reported cases responded well to endovascular embolization.
The LFI osteotomy involves an ascending bone cut from the PTJ to the pyriform aperture, along the lateral nasal wall, and includes fracturing the nasal septum. Special attention must be paid to avoid injuring adjacent soft tissues, especially the small and large blood vessels in the posterior nasal cavity and pterygopalatine fossa—regions approximately 2.5 cm from the PTJ (37). These areas are difficult to access and highly vascularized by the internal maxillary artery and its branches, making them particularly vulnerable to surgical trauma (12).
In several cases, the specific arterial branch involved in a complication could not be identified, as many studies did not clearly report which vessel was affected. Nonetheless, among identifiable cases, the sphenopalatine artery was the most commonly involved branch of the maxillary artery (4,7,10,16,18,27,28).
It is important to note that improper execution of the PTJ separation and subsequent down-fracture may generate excessive force on the skull base, potentially resulting in fractures and damage to adjacent structures. Inappropriate angulation of osteotomes, incomplete osteotomy cuts, and improper activation of expansion devices are reported contributors to such complications (6,8,10,13,14,20,22).
After down-fracture, the maxilla's blood supply mainly depends on the ascending pharyngeal, ascending palatine, descending palatine, and small mucosal terminal arteries. There is ongoing debate about whether sacrificing the descending palatine arteries is justified to prevent hemorrhage, especially in complex cases like clefts or syndromic patients. However, refined surgical techniques can often prevent complications while preserving vascular integrity (25,33).
Avascular necrosis of the maxilla (24,29-31,33) is an important complication associated with LFI osteotomy. In most reported cases, it led to partial bone loss, including the loss of teeth and alveolar bone segments, and occasionally resulted in oronasal fistulas. In more severe instances, total maxillary necrosis occurred, causing devastating functional and aesthetics consequences. To reduce the risk of this outcome, it is essential to ensure adequate vascular supply through meticulous surgical planning and techniques such as hypotensive anesthesia.
In conclusion, LFI osteotomy requires precise surgical technique and a thorough understanding of the anatomical landscape, particularly the vascular structures in high-risk regions such as the pterygoid and posterior nasal fossae. Early recognition and diagnosis of vascular complications, along with timely and appropriate interventions coordinated through multidisciplinary collaboration, are essential to minimizing morbidity and optimizing patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Buchanan EP Hyman CH Le Fort I osteotomy Semin Plast Surg 201327149542487276110.1055/s-0033-1357112 PMC 3805729 · doi ↗ · pubmed ↗
- 2Jeong HI Lee HS Jung YS Park HS Jung HD Nasal soft tissue change following bimaxillary orthognathic surgery Journal of Craniofacial Surgery 201728 e 605e 82857041010.1097/SCS.0000000000003736 · doi ↗ · pubmed ↗
- 3Chepla KJ Totonchi A Hsu DP Gosain AK Maxillary artery pseudoaneurysm after Le Fort I osteotomy: treatment using transcatheter arterial embolization. J. Craniofac Surg 2010211079812061356710.1097/SCS.0b 013e 3181 e 20693 · doi ↗ · pubmed ↗
- 4Procopio O Fusetti S Liessi G Ferronato G False aneurysm of the sphenopalatine artery after a Le Fort I osteotomy: report of 2 cases J Oral Maxillofac Surg 20036152041268497410.1053/joms.2003.50100 · doi ↗ · pubmed ↗
- 5Politis C Life-threatening hemorrhage after 750 Le Fort I osteotomies and 376 SARPE procedures Int J Oral Maxillofac Surg 20124170282248087710.1016/j.ijom.2012.02.015 · doi ↗ · pubmed ↗
- 6Moher D Liberati A Tetzlaff J Altman DG The PRISMA Group Preferred reporting items for systematic reviews and meta-analyses:the PRISMA statement P Lo S Med 20096 e 10000971962107210.1371/journal.pmed.1000097 PMC 2707599 · doi ↗ · pubmed ↗
- 7Avelar RL Goelzer JG Becker O Ede Oliveira RB Raupp E Fde Magalhães PSC Embolization of pseudoaneurysm of the internal maxillary artery after orthognathic surgery J Craniofac Surg 201021176482111941710.1097/SCS.0b 013e 3181 f 40393 · doi ↗ · pubmed ↗
- 8Hacein-Bey L Blazun JM Jackson RF Carotid artery pseudoaneurysm after orthognathic surgery causing lower cranial nerve palsies: endovascular repair J Oral Maxillofac Surg 2013711948552399277910.1016/j.joms.2013.07.001 · doi ↗ · pubmed ↗