Paraneoplastic Remitting Seronegative Symmetrical Synovitis With Pitting Edema: A Systematic Review of Case Reports and Observational Studies on Clinical Features, Treatment Response, and Outcomes
Ryuichi Ohta, Yoshinori Ryu, Kaoru Tanaka, Chiaki Sano, Kunihiro Ichinose, Hidetoshi Hayashi

TL;DR
This study reviews cases of a rare inflammatory condition called RS3PE that is linked to cancer, highlighting its symptoms, cancer associations, and treatment outcomes.
Contribution
The paper systematically reviews clinical features and outcomes of paraneoplastic RS3PE, emphasizing its role as a cancer marker.
Findings
RS3PE is strongly associated with malignancies like prostate, lung, and gastrointestinal cancers.
Corticosteroid response rates vary by region, with higher remission rates in Japanese and U.S. cohorts.
RS3PE often coincides with cancer diagnosis, suggesting it is a sentinel marker for malignancy.
Abstract
Remitting seronegative symmetrical synovitis with pitting edema (RS3PE) is an uncommon inflammatory disorder that may occur as a paraneoplastic manifestation. To clarify its clinical profile, we reviewed published cases and observational studies reporting paraneoplastic RS3PE. A total of 120 patients were identified, including 40 individual case reports and four observational cohorts. The mean age was 69 years, and men accounted for approximately 70-80% of patients. Associated malignancies were diverse, with prostate (22%), lung (18%), and gastrointestinal cancers (16%) being the most frequent among solid tumors, alongside hematologic malignancies such as lymphoma and leukemia (12%). The hallmark clinical presentation was symmetrical synovitis of the hands and feet with pitting edema. Systemic features were common, including fever (36%), weight loss (28%), and fatigue (21%).…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
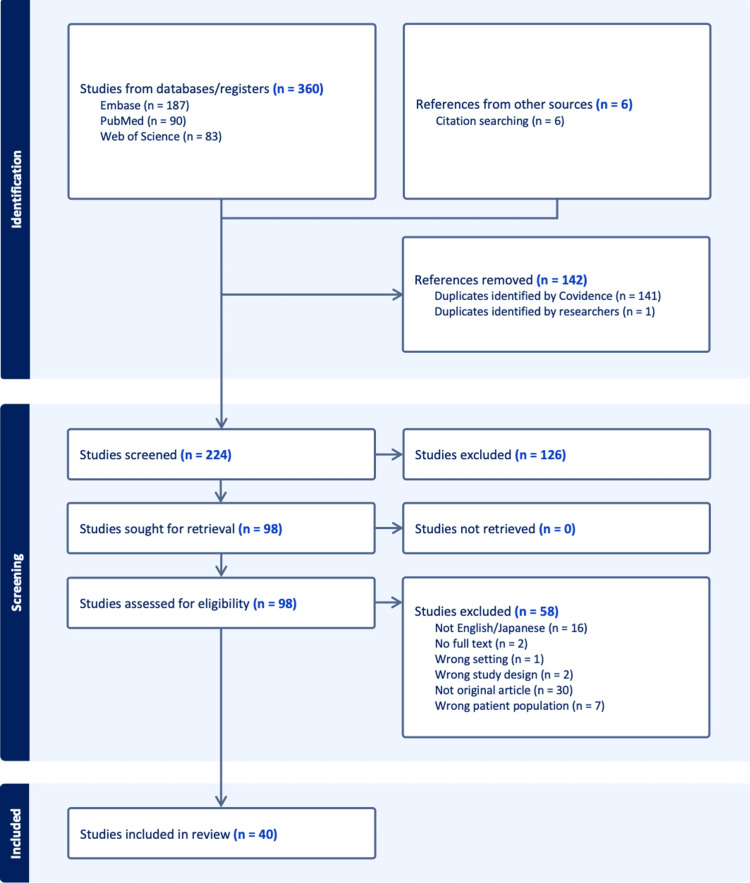 Figure 1
Figure 1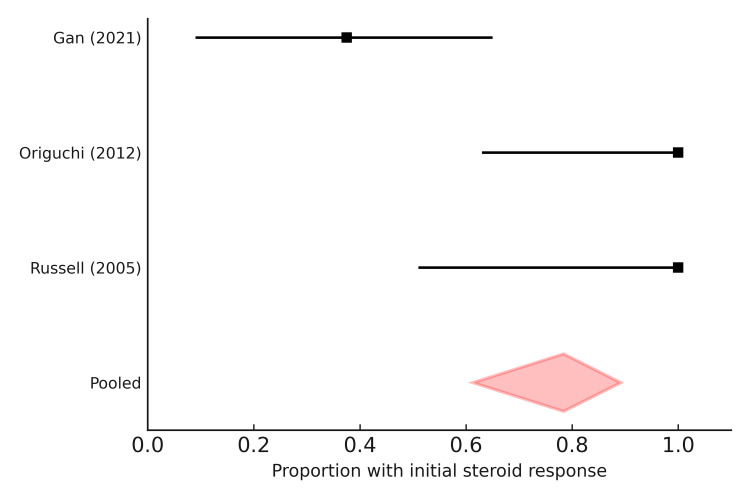 Figure 2
Figure 2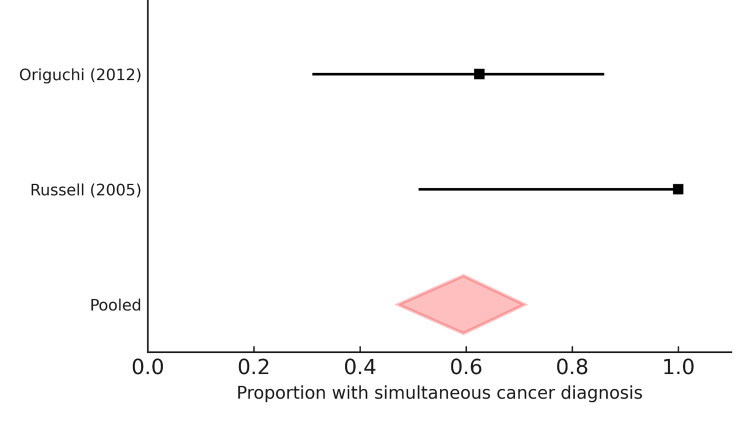 Figure 3
Figure 3| Published Year | First Author | Country | Age | Sex | Tumor type (solid tumor vs hematologic malignancy) |
| 1997 | Domenico Olivo [ | Italy | 76 | Female | Solid tumor – Endometrial adenocarcinoma (moderately differentiated, infiltrating) |
| 2002 | S. Paira [ | Argentina | 68 | Male | Rectal adenocarcinoma |
| 2002 | S. Paira [ | Argentina | 62 | Male | Malignant fibrohistiocytoma (iliac bone) |
| 2002 | S. Paira [ | Argentina | 75 | Male | Myelodysplastic syndrome (hematologic) |
| 2002 | S. Paira [ | Argentina | 60 | Male | Non-Hodgkin’s lymphoma |
| 2002 | Tadakuni Yamasaki [ | Japan | 67 | Male | Hematologic malignancy – Peripheral T-cell lymphoma |
| 2004 | Olivier Gisserot [ | France | 65 | Female | Hematologic malignancy – peripheral T-cell non-Hodgkin’s lymphoma (recurrence) |
| 2004 | S.E. Tunc [ | Turkey | 74 | Male | Solid tumor – Prostate adenocarcinoma |
| 2004 | S.E. Tunc [ | Turkey | 70 | Male | Solid tumor – Prostate adenocarcinoma |
| 2004 | Masayuki Suga [ | Japan | 83 | Male | Solid tumor – Lung squamous cell carcinoma |
| 2005 | Nicole Chiappetta [ | USA | 82 | Male | Hematologic malignancy – Acute Myeloid Leukemia (AML) |
| 2005 | Tohru Ishikawa [ | Japan | 64 | Male | Solid tumor – Metastatic squamous cell carcinoma (cervical lymph node, lung metastases; primary uncertain, likely oral origin) |
| 2007 | Francesco U. S. Mattace-Raso [ | Netherlands | 78 | Female | Solid tumor – Lung malignancy (not otherwise specified, large right lung mass) |
| 2008 | Mustafa Özdemir [ | Turkey | 70 | Female | Solid tumor – Kaposi sarcoma (cutaneous) |
| 2010 | Gonçalo Marto [ | Portugal | 74 | Male | Solid tumor – prostate adenocarcinoma |
| 2011 | Rurika Hamanaka [ | Japan | 79 | Male | Solid tumor – Combined large cell neuroendocrine carcinoma + squamous cell carcinoma + adenocarcinoma |
| 2012 | R.N. Sarkar [ | India | 40 | Female | Solid tumor – Phyllodes tumor of breast (recurrent) |
| 2013 | Cláudia Ferrao [ | Portugal | 60 | Male | Solid tumor – non-small cell lung carcinoma (adenosquamous type) |
| 2014 | Ilknur Aktas [ | Turkey | 72 | Male | Solid tumor – Prostate adenocarcinoma |
| 2016 | Amir Emamifar [ | Denmark | 83 | Male | Solid tumor – Prostate adenocarcinoma |
| 2017 | Takahiko Sakamoto [ | Japan | 69 | Male | Solid tumor – Lung adenocarcinoma (EGFR exon21 L858R mutation) |
| 2017 | Hiroyasu Matsuoka [ | Japan | 77 | Male | Solid tumor – Primary lung adenocarcinoma (acinar predominant) |
| 2017 | Tomoya Sagawa [ | Japan | 69 | Male | Solid tumor – Pulmonary pleomorphic carcinoma (hCG-producing) |
| 2018 | Edgar Pratas [ | Portugal | 80 | Male | Solid tumor – adenocarcinoma of caecum |
| 2018 | Shuta Ohara [ | Japan | 67 | Male | Solid tumor – Lung adenocarcinoma (papillary type) |
| 2018 | Katsuyuki Suzuki [ | Japan | 67 | Male | Solid tumor – Minimally invasive lung adenocarcinoma |
| 2019 | Yoichiro Aoshima [ | Japan | 69 | Male | Solid tumor – lung adenocarcinoma |
| 2020 | Shugo Yajima [ | Japan | 77 | Male | Solid tumor – prostate adenocarcinoma |
| 2022 | Sae Ohwada [ | Japan | 76 | Male | Solid tumor – Hepatocellular carcinoma |
| 2022 | L. Merkle Moore [ | USA | 47 | Male | Hematologic malignancy – CLL (with suspected NET) |
| 2023 | Kain Kim [ | USA | 62 | Male | History of solid tumor – prostate cancer (inactive) |
| 2023 | Taketsugu Kawano [ | Japan | 46 | Female | Solid tumor – ovarian clear cell carcinoma |
| 2023 | Gen Ohara [ | Japan | 86 | Male | Solid tumor – Lung squamous cell carcinoma |
| 2023 | Misa Itamura [ | Japan | 65 | Female | Solid tumor – High-grade serous ovarian carcinoma |
| 2023 | Narumi Ishihara [ | Japan | 75 | Male | Hematologic malignancy – Angioimmunoblastic T-cell lymphoma (AITL), diagnosed as OI-LPD (methotrexate/tacrolimus-associated) |
| 2024 | Rishi Raman [ | India | 60 | Female | Solid tumor – Gastroesophageal junction squamous cell carcinoma (poorly differentiated) |
| 2024 | Maria Inês Matos [ | Portugal | 72 | Male | Solid tumor – Clear cell renal cell carcinoma |
| 2024 | Shuta Kimura [ | Japan | 63 | Male | Solid tumor – Lung adenocarcinoma (poorly differentiated) |
| 2025 | Shoji Mochizuki [ | Japan | 70 | Male | Solid tumor – Squamous cell carcinoma, cancer of unknown primary origin (CUP) |
| 2025 | Samar Alharbi [ | Saudi Arabia | 58 | Female | Solid tumors – Papillary thyroid carcinoma + Adenocarcinoma of unknown primary origin (inguinal lymph node metastasis, suspected breast/gynecologic/lung/pancreatobiliary origin) |
| Published Year | First Author | Country | Study design | Sample size | Mean/median age | Sex distribution |
| 2005 | Elizabeth B. Russell [ | USA | Retrospective cohort follow-up (10 patients with RS3PE, mean follow-up up to 19 years) | 4 paraneoplastic RS3PE patients (out of 10 total with follow-up) | Not separately reported (overall mean = 68 years, range 45–81) | 100% male (4/4) |
| 2012 | Tomoki Origuchi [ | Japan | Retrospective multicenter cohort study | 33 patients with RS3PE (8 paraneoplastic, 24 non-neoplastic, 1 excluded from analysis) | Median 79 years (range 73–87) | 7 male, 1 female (87.5% male) |
| 2021 | Misako Higashida-Konishi [ | Japan | Retrospective medical record study | 24 RS3PE patients (of whom 6 had malignancies = paraneoplastic RS3PE) | 78–87 | 5 male, 1 female |
| 2021 | Yuzhou Gan [ | China | Ambispective single-center cohort study | 51 RS3PE patients (48 with follow-up; 8 with malignancy = paraneoplastic RS3PE) | Mean 75.0 ± 11.1 years (range 53–85) | 5 male, 3 female |
| Feature | N | % |
| Hands involvement | 26 | 65 |
| Wrists involvement | 20 | 50 |
| Feet/ankle involvement | 20 | 50 |
| Knee involvement | 16 | 40 |
| Shoulder involvement | 14 | 35 |
| Hip involvement | 5 | 12.5 |
| Weight loss | 10 | 25 |
| Anorexia | 5 | 12.5 |
| Fatigue / malaise / asthenia | 10 | 25 |
| Anemia | 6 | 15 |
| Skin manifestations | 2 | 5 |
| Fever (Yes) | 10 | 25 |
| Fever (No) | 11 | 27.5 |
| Fever (Not reported) | 19 | 47.5 |
| CRP elevated (reported) | 31 | 77.5 |
| CRP very high (>100 mg/L) | 5 | 12.5 |
| ESR elevated (reported) | 27 | 67.5 |
| ESR very high (>50 mm/h) | 15 | 37.5 |
| First Author (Year) | Cases (n) | Joint involvement | Systemic symptoms | Inflammatory markers | Biomarkers / Tumor markers |
| Elizabeth B. Russell (2005) [ | 4 | 100% bilateral hands (MCP, small joints) | Not systematically reported | ESR elevated; CRP not reported | Not reported |
| Tomoki Origuchi (2012) [ | 8 | Shoulders 37.5%, elbows 37.5%, wrists majority, MCP 62.5% | Fever 50% | Median ESR 89 mm/h (55–108), CRP 6.1 mg/dL (2.1–13.2) | Not reported |
| Misako Higashida-Konishi (2021) [ | 6 | Not separately reported; overall RS3PE: multiple joints | Overall RS3PE: fever 12.5% (not subgroup-specific) | Median ESR 48 mm/h (30–70), CRP 5.3 mg/dL (3.4–9.8) | Not reported |
| Yuzhou Gan (2021) [ | 8 | Hands bilateral 62.5%, wrists/ankles also affected | Weight loss 62.5% | ESR 19–86 mm/h, CRP elevated; bFGF high | bFGF elevated; AFP 14.3%, CYFRA21-1 14.3% |
| Outcome | N / Value |
| Steroid use (reported) | 30 / 40 cases (75%) |
| Median initial steroid dose (mg/day) | 10 mg/day |
| Dose range (mg/day) | 5-30 mg/day (up to 80 mg/day in rare cases) |
| Representative steroid doses and responses | 10 mg/day: transient improvement, relapse (Olivo 1997) [ |
| Complete remission | 15 cases (37.5%) |
| Partial remission | 2 cases (5%) |
| No remission / refractory | 3 cases (7.5%) |
| Relapse during course | 8 cases (20%) |
| Deaths during follow-up | 9 cases (22.5%) |
| First Author (Year) | Initial steroid response | Relapse | Remission rate | Mortality | Notes / Biomarkers |
| Elizabeth B. Russell (2005) [ | 4/4 (100%) complete response | 0/4 (0%) | 100% initial remission | 3/4 (75%) died of malignancy | Outcomes dominated by underlying malignancy |
| Tomoki Origuchi (2012) [ | 8/8 (100%) good response | 1/8 (12.5%) | 100% | Not reported | Uniform steroid response, single relapse |
| Misako Higashida-Konishi (2021) [ | Not separately reported (overall good response) | Not specified; tendency for higher relapse in cancer patients | Not available | Not separately reported; worse in paraneoplastic subgroup | Median follow-up 31.5 months; subgroup not detailed |
| Yuzhou Gan (2021) [ | 3/8 (37.5%) good response; 5/8 (62.5%) poor response | Several relapses reported, often with cancer progression (~20%) | 42.8% vs. 97.4% in idiopathic RS3PE | Not specified; poorer long-term outcomes compared with idiopathic | bFGF elevated; poor steroid responsiveness linked to malignancy |
| Timing category | N (cases) | % of total (N=40) | Representative examples |
| Simultaneous (RS3PE and cancer diagnosed in parallel) | 20 | 50 | Lung cancer, prostate cancer, lymphoma detected during RS3PE evaluation |
| RS3PE preceding cancer diagnosis | 10 | 25 | Acute myeloid leukemia, hepatocellular carcinoma, prostate cancer, lymphoma diagnosed weeks to years later |
| Cancer preceding RS3PE | 5 | 12.5 | RS3PE onset 6 weeks post-prostatectomy; RS3PE during chemotherapy for gastrointestinal cancer |
| RS3PE associated with cancer recurrence | 5 | 12.5 | RS3PE relapse coinciding with recurrence of lymphoma or Kaposi sarcoma |
| First Author (Year) | Simultaneous diagnosis | RS3PE preceding cancer | Cancer preceding RS3PE | RS3PE at cancer recurrence |
| Elizabeth B. Russell (2005) [ | 4/4 (100%) | 0/4 (0%) | 0/4 (0%) | Not reported |
| Tomoki Origuchi (2012) [ | 5/8 (62.5%) | 2/8 (25%) | 1/8 (12.5%) | Not reported |
| Misako Higashida-Konishi (2021) [ | Most cases (exact number not reported) | Some cases, within 1 year (not specified) | Occasional, not quantified | Not reported |
| Yuzhou Gan (2021) [ | 5/8 (62.5%) | 2/8 (25%) | 1/8 (12.5%) | Observed in some patients (number not specified) |
| Study (year, country) | Selection (0–4) | Comparability (0–2) | Outcome (0–3) | NOS total (0–9) | Risk category | Key limitations noted |
| Elizabeth B. Russell 2005 (USA) [ | 3 | 1 | 2 | 6 | Some concerns | Small N; retrospective; limited confounder control; cancer outcomes dominate long-term results |
| Tomoki Origuchi 2012 (Japan) [ | 3 | 1 | 3 | 7 | Low risk | Multicenter but limited adjustment; elderly cohort; incomplete detail on some confounders |
| Misako Higashida-Konishi 2021 (Japan) [ | 3 | 1 | 2 | 6 | Some concerns | Single center; small N; subgroup outcomes for paraneoplastic cases not fully detailed |
| Yuzhou Gan 2021 (China) [ | 3 | 1 | 3 | 7 | Low risk | Ambispective design; biomarker substudies; limited multivariable adjustment |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEosinophilic Disorders and Syndromes · Musculoskeletal synovial abnormalities and treatments · Inflammatory Myopathies and Dermatomyositis
Introduction and background
Remitting seronegative symmetrical synovitis with pitting edema (RS3PE) syndrome is a rare inflammatory rheumatic disorder first described by McCarty and colleagues in 1985 [1,2]. The true prevalence or incidence of RS3PE remains unknown, as large-scale epidemiologic studies are lacking. Several reviews note that it is highly uncommon [1,2]. RS3PE primarily affects elderly individuals, with a mean onset age of around 70 years, and is characterized by acute symmetrical synovitis, prominent pitting edema of the dorsum of the hands or feet, negativity for rheumatoid factor (RF), and a rapid response to low- to moderate-dose glucocorticoids [1-3]. Laboratory findings frequently include elevated C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) [3]. Diagnosis is made clinically and serologically, after excluding other inflammatory conditions such as polymyalgia rheumatica, rheumatoid arthritis, or crystal-induced arthritis [4].
Over the past decades, increasing attention has focused on the relationship between RS3PE and malignancy. Previous studies have reported that approximately 16-30% of RS3PE cases are associated with cancer, usually within one year before or after the diagnosis of RS3PE [5,6]. Both solid tumors (prostate, gastric, colorectal, and lung cancers) and hematologic malignancies (lymphomas, leukemias) have been described [5-7]. When RS3PE occurs in association with malignancy, it is regarded as a paraneoplastic syndrome, showing distinctive clinical features compared with non-paraneoplastic RS3PE [8]. These include incomplete or transient responses to corticosteroid therapy, complete remission of symptoms following definitive cancer treatment, and higher risks of recurrence and mortality [5-8].
Although the pathophysiological mechanisms remain unclear, several biomarkers have been implicated. Elevated vascular endothelial growth factor (VEGF) and basic fibroblast growth factor (bFGF) have been reported in paraneoplastic cases, suggesting a role in synovial inflammation and subcutaneous edema formation [8]. Matrix metalloproteinase-3 (MMP-3) has also been proposed as a biomarker for disease activity and association with malignancy [8].
In 2016, Karmacharya et al. performed a systematic review of 331 RS3PE cases and found a malignancy association in 16.3%, as well as a higher risk of recurrence among cancer-associated cases [9]. However, their analysis did not focus specifically on paraneoplastic RS3PE, nor did it explore biomarker differences, treatment response, or survival outcomes in detail. Since then, additional case reports and cohort studies have been published, but no updated systematic review has specifically addressed the clinical characteristics and prognosis of paraneoplastic RS3PE.
Therefore, we conducted a systematic review of case reports, case series, and observational studies of paraneoplastic RS3PE. This study aimed to comprehensively evaluate the clinical features, diagnostic timing, treatment responses, and outcomes of paraneoplastic RS3PE. Our objectives were to clarify: (1) the demographic and clinical characteristics of paraneoplastic RS3PE, (2) the timing of cancer diagnosis relative to RS3PE onset, (3) treatment responses to corticosteroid therapy and cancer therapy, and (4) outcomes including recurrence and mortality. By synthesizing evidence from both descriptive and observational studies, this review aims to provide a comprehensive understanding of paraneoplastic RS3PE and inform strategies for cancer screening and individualized management in patients presenting with this syndrome.
Review
Study design
This study was conducted as a systematic review according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines for reporting systematic reviews and was prospectively registered with the International Prospective Register of Systematic Reviews (PROSPERO; registration ID: CRD420251128476) [10].
Data sources and search strategy
We systematically searched PubMed, Embase, and Web of Science from January 1, 1995, to August 31, 2025. Additional sources, including the Cochrane Library and Scopus, were screened for potential relevance. The search strategy combined Medical Subject Headings (MeSH) and free-text terms: ("RS3PE" OR "remitting seronegative symmetrical synovitis with pitting edema") AND ("paraneoplastic" OR "malignancy" OR "cancer" OR "neoplasm" OR "tumor"). Searches were restricted to English/Japanese-language publications. Case reports, case series, and observational studies were included. Unpublished studies, conference abstracts, and non-peer-reviewed reports were excluded to ensure data quality. The search process and results were thoroughly documented to ensure reproducibility.
Eligibility criteria
Studies were eligible if they met the following criteria: adults (≥18 years) with RS3PE diagnosed according to established clinical criteria (acute onset, bilateral pitting edema, symmetrical synovitis, RF negativity), documented diagnosis of malignancy with RS3PE onset or remission of RS3PE following cancer treatment, consistent with paraneoplastic RS3PE, reported clinical features, biomarkers, treatment response, or outcomes (e.g., remission, recurrence, mortality) and study design such as case reports, case series, or observational studies (retrospective/prospective cohorts or cross-sectional studies). Exclusion criteria were drug-induced RS3PE (e.g., immune checkpoint inhibitor-related), pediatric cases (<18 years), reports lacking information on malignancy status, and non-English/Japanese publications without sufficient data for extraction. We also excluded duplicate publications, conference abstracts without full-text data, review articles without extractable patient-level information, and studies where RS3PE diagnosis did not fulfill established clinical criteria.
Study selection
Two reviewers (RO and YR) independently screened titles and abstracts. Full texts of potentially eligible studies were retrieved and assessed against the inclusion criteria. Disagreements were resolved by consensus or consultation with a third reviewer. The selection process was recorded in a PRISMA flow diagram.
Data extraction
Data were independently extracted by two reviewers using a standardized form. Extracted information included study characteristics (year, first author, country, study design and sample size), patient demographics (age, sex, and comorbidities), cancer-related variables (tumor type (solid vs hematologic), stage, and timing relative to RS3PE onset (preceding, synchronous, subsequent)), clinical features of RS3PE (joint distribution, systemic symptoms (fever, weight loss, fatigue), and laboratory findings (CRP, ESR, VEGF, MMP-3, bFGF, tumor markers)), treatment (initial steroid dose, response (complete, partial, refractory), and oncological therapies) and outcomes (remission, recurrence, time to recurrence, mortality, and follow-up duration). When data were incomplete, efforts were made to extract the maximum available information; missing data were reported as “not available.”
Data synthesis
Descriptive statistics were used to summarize patient demographics, cancer characteristics, and RS3PE features. Continuous variables were expressed as mean with standard deviation or median with interquartile range (IQR), as appropriate. Categorical variables were summarized as frequencies and percentages.
In addition to descriptive synthesis, a meta-analysis was performed when data from at least three observational cohorts were available. Pooled estimates were calculated for initial corticosteroid responsiveness and the timing of cancer diagnosis relative to RS3PE onset (preceding, synchronous, subsequent), using a random-effects model (DerSimonian-Laird method) with 95% confidence intervals. Heterogeneity was quantified with the I² statistic, with values >50% considered indicative of substantial heterogeneity. Forest plots were constructed to summarize pooled effect sizes visually. Subgroup analyses were planned for tumor type (solid vs. hematologic) and biomarker levels (e.g., VEGF, MMP-3, bFGF), where data allowed, and by geographical region. Assessment of publication bias (e.g., funnel plots and Egger’s test) was planned for outcomes with ≥10 studies; however, the number of eligible studies for meta-analysis was limited, precluding a formal assessment.
The methodological quality of the included observational studies was assessed independently by two reviewers using the Newcastle-Ottawa Scale (NOS) for cohort studies, which evaluates three domains: (1) selection of study groups, (2) comparability of cohorts, and (3) ascertainment of outcomes. Each study was awarded up to nine stars, with higher scores indicating lower risk of bias [11]. Case reports were not formally appraised, given their descriptive design, but they were considered inherently at high risk of bias. Discrepancies were resolved by consensus.
Results
Study Selection
A total of 360 records were identified through electronic database searches: 187 from Embase, 90 from PubMed, and 83 from Web of Science. An additional six records were retrieved through citation searching, giving a total of 366 references for screening. After removing 142 duplicates, 224 unique records remained for title and abstract screening. Of these, 126 were excluded, and 98 full-text articles were sought for retrieval. All full texts were successfully obtained. Following full-text review, 58 articles were excluded for the following reasons: not in English or Japanese (n = 16), no full text available (n = 2), wrong setting (n = 1), wrong study design (n = 2), not original research (n = 30), and wrong patient population (n = 7). Ultimately, 40 studies met the eligibility criteria and were included in the systematic review (Figure 1).
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 flow diagram for study selection.A total of 366 records were identified (360 through database searches and six through citation searching). After the removal of 142 duplicates, 224 records were screened. Of these, 126 were excluded, leaving 98 full-text articles assessed for eligibility. Fifty-eight full-text articles were excluded (not English/Japanese, n = 16; no full text, n = 2; wrong setting, n = 1; wrong study design, n = 2; not original research, n = 30; wrong patient population, n = 7). Finally, 40 studies met the inclusion criteria and were included in the systematic review.
Study Characteristics
Case reports:* *A total of 40 paraneoplastic RS3PE cases were identified from published case reports included in this review. The majority of patients were older adults, with a mean age of 68.9 years, a median of 69.5 years, and an overall age range of 40 to 86 years. Most cases occurred in men (31/40, 77.5%), while women accounted for 9/40 (22.5%).
Cancer types associated with RS3PE were heterogeneous. Among solid tumors, the most frequently reported were prostate adenocarcinoma (n = 6), followed by lung cancers, including adenocarcinoma (n = 4), squamous cell carcinoma (n = 2), and other histologies such as large-cell neuroendocrine carcinoma and pulmonary pleomorphic carcinoma. Additional solid tumors included gastroesophageal junction carcinoma, colorectal adenocarcinoma, renal cell carcinoma, ovarian carcinoma, endometrial adenocarcinoma, hepatocellular carcinoma, papillary thyroid carcinoma, breast phyllodes tumor, malignant fibrohistiocytoma, and Kaposi sarcoma.
In contrast, hematologic malignancies were also represented, including non-Hodgkin lymphomas (n = 3), acute myeloid leukemia (n = 1), chronic lymphocytic leukemia (n = 1), angioimmunoblastic T-cell lymphoma (n = 1), peripheral T-cell lymphomas (n = 2), and myelodysplastic syndrome (n = 1) (Table 1).
Observational study:* *Four observational studies were included, comprising a total of 120 patients diagnosed with RS3PE, of whom between 15.7% and 40% were classified as paraneoplastic, depending on the study population and methodology. The earliest study, conducted in the United States (Russell et al., 2005), analyzed a retrospective cohort of 10 patients, including four paraneoplastic cases (40%), all male and with hematologic malignancies. Although all initially responded to low-dose corticosteroids, three subsequently died of underlying cancer, yielding a 75% mortality rate among paraneoplastic cases [47].
A Japanese multicenter cohort (Origuchi et al., 2012) included 33 patients, with eight (24.2%) identified as paraneoplastic. The median age was 79 years (range 73-87), with a clear male predominance (87.5%). All paraneoplastic patients responded to corticosteroids initially, but one relapsed during follow-up. Mortality data were not systematically reported [48].
A subsequent single-center retrospective review from Japan (Higashida-Konishi et al., 2021) evaluated 24 patients, of whom six (25%) were paraneoplastic, aged 78-87 years, again predominantly men (83%). The median follow-up was 31.5 months; however, treatment response and outcomes were not separately analyzed for the paraneoplastic subgroup [49].
The most recent ambispective cohort from China (Gan et al., 2021) analyzed 51 patients, including eight (15.7%) with paraneoplastic RS3PE (mean age 75 years, range 53-85; 62.5% male) [5]. In contrast to earlier cohorts, paraneoplastic patients demonstrated poorer steroid responsiveness, with 62.5% showing inadequate response compared to idiopathic RS3PE. Moreover, remission rates were substantially lower in the paraneoplastic group (42.8% vs. 97.4%). Biomarker analyses revealed that elevated bFGF may serve as a potential marker for malignancy-associated RS3PE.
Overall, across these cohorts, paraneoplastic RS3PE was consistently observed in older adults (median age 75-79 years) with a marked male predominance. The frequency of paraneoplastic cases varied widely, ranging from 15.7% to 40%. While initial steroid responsiveness was generally favorable in the Japanese cohorts, outcomes were poorer in the Chinese study, highlighting heterogeneity in clinical trajectories. Mortality was primarily driven by underlying cancer, with the highest rate reported in the earliest U.S. cohort (Table 2).
Clinical Features of Paraneoplastic RS3PE
Case reports:* *Among the 40 paraneoplastic RS3PE cases, the hallmark presentation was symmetrical synovitis with pitting edema, particularly affecting distal joints. Regarding joint involvement, hands were the most frequently affected (26/40, 65%), often with swelling of the dorsum. Wrists were involved in 20/40 (50%) cases. Feet/ankles were also commonly affected (20/40, 50%). Knees were affected in 16/40 (40%), and shoulders in 14/40 (35%). Hips were less commonly reported (5/40, 12.5%). Overall, most cases showed bilateral and symmetrical involvement, sometimes extending from distal to proximal joints.
Regarding systemic manifestations, weight loss was reported in 10/40 (25%) cases. Anorexia was present in 5/40 (12.5%). Fatigue, asthenia, or general malaise were described in 10/40 (25%). Anemia was documented in 6/40 (15%). Skin manifestations (rash, panniculitis, dermatomyositis-like) were rare, noted in two cases (5%). About one-third of reports explicitly mentioned no systemic symptoms, while in other cases, no data were reported.
Regarding fever, fever was documented in 10/40 (25%), typically low- to moderate-grade (37-39 °C), sometimes recurrent. In contrast, 11/40 (27.5%) were explicitly reported as afebrile. In 14/40 (35%), fever status was not recorded.
Regarding inflammatory markers, elevated CRP and ESR were nearly universal. Several reports documented CRP >100-200 mg/L and ESR >50 mm/h, confirming high inflammatory activity. Isolated cases noted extreme CRP elevation (≥250 mg/L) and leukocytosis. A minority of cases included biomarker data such as VEGF, MMP-3, or bFGF, though these were not consistently available (Table 3).
Observational study:* *Across the four observational cohorts, paraneoplastic RS3PE was consistently characterized by distal symmetrical synovitis with pitting edema, most often involving the hands and wrists and sometimes extending to shoulders, elbows, knees, and ankles. In the paraneoplastic subsets, the frequency of hand involvement reached 60-100%, confirming its role as the hallmark feature.
Systemic manifestations were variably present but noteworthy. Fever was observed in up to 50% of paraneoplastic patients in Japanese cohorts, whereas weight loss was prominent in the Chinese cohort, affecting 62.5%. Fatigue, anorexia, and anemia were less consistently described but were recognized in smaller proportions. These features suggest that paraneoplastic RS3PE is more likely than idiopathic RS3PE to be accompanied by constitutional symptoms, reflecting the influence of underlying malignancy.
Inflammatory markers were uniformly elevated. Reported median CRP levels ranged between 5 and 6 mg/dL, with values often exceeding 10 mg/dL, while ESR commonly exceeded 50 mm/h (median 48-89 mm/h across cohorts). Although rheumatoid factor was consistently negative, as per the diagnostic criteria, selected biomarker studies revealed potential signals related to malignancy. In particular, the Chinese cohort identified bFGF as significantly elevated in paraneoplastic cases. At the same time, other tumor markers such as AFP and CYFRA21-1 were occasionally abnormal in individual patients (Table 4).
Treatment Response and Outcomes
Case report:* *Regarding steroid therapy, initial corticosteroid therapy was reported in 30 of 40 cases (75%). The median starting dose was 10 mg/day (prednisolone equivalent), with a range from 0 to 80 mg/day. Despite therapy, steroid efficacy was inconsistent. Complete remission after steroids alone was achieved in 15 cases (37.5%). Partial remission was described in two cases (5%), often requiring dose escalation or additional immunomodulators. No remission or refractory disease despite steroids was reported in three cases (7.5%). Several cases noted relapse upon tapering (<12.5 mg/day), highlighting dose sensitivity.
Regarding tumor-directed therapy, in multiple cases, RS3PE symptoms resolved only after tumor treatment (surgery, chemotherapy, or radiotherapy), even when steroids had been ineffective. Reports emphasized that edema and synovitis improved in parallel with tumor regression, supporting the paraneoplastic mechanism.
Relapse occurred in eight of 40 cases (20%), most often during steroid tapering. In several reports, relapse coincided with tumor recurrence or progression, reinforcing the tight association between cancer activity and RS3PE.
Regarding mortality, at least nine of 40 patients (22.5%) died during follow-up, primarily due to underlying malignancy or treatment complications. Conversely, more than half of patients (>20/40, ~50%) were alive and symptom-free or stable at last follow-up. Reported follow-up durations ranged from three months to over eight years (Table 5).
Table 5: Treatment response, steroid dosing, and outcomes of paraneoplastic remitting seronegative symmetrical synovitis with pitting edema (RS3PE)Steroid dose is expressed as prednisolone equivalent. Median and range were calculated from 30 cases with reported doses. Representative examples are derived from individual case reports (e.g., Olivo 1997 [12], Paira 2002 [13], Marto 2010 [22], Ferrao 2013 [25], Aktas 2014 [26]). “Complete remission” indicates full resolution of RS3PE symptoms, whereas “partial remission” reflects persistent or relapsing disease despite steroids. “Relapse” generally occurred during steroid tapering (<12.5 mg/day) or with cancer recurrence. Mortality data primarily reflect deaths due to underlying malignancy or treatment complications. Percentages are calculated from a total of 40 included cases.
Observational study:* *Treatment outcomes of paraneoplastic RS3PE varied across cohorts but showed typical patterns of initial steroid responsiveness, risk of relapse, and mortality strongly linked to the underlying malignancy.
In the earliest U.S. cohort by Russell et al. (2005), all four paraneoplastic patients (100%) achieved initial remission with low-dose corticosteroids. Yet, three of the four (75%) died from their malignancies during follow-up, underscoring that long-term prognosis was dominated by cancer rather than RS3PE itself [47].
The Japanese multicenter cohort by Origuchi et al. (2012) similarly reported uniform initial responses (8/8, 100%) to corticosteroids, with one relapse (12.5%) documented during follow-up. Mortality outcomes were not systematically reported, but the relatively high age of this group (median 79 years) suggests considerable comorbidity and frailty [48].
In the single-center study by Higashida-Konishi et al. (2021), six paraneoplastic cases were identified within 24 patients overall [49]. While subgroup outcomes were not detailed numerically, the cohort as a whole demonstrated a median follow-up of 31.5 months, with indications that patients with cancer had more frequent relapse and worse survival, even if precise percentages were unavailable.
By contrast, the Chinese ambispective study by Gan et al. (2021) demonstrated poorer steroid outcomes [5]. Among eight paraneoplastic cases, five (62.5%) showed inadequate steroid responses, and the overall remission rate was markedly lower than idiopathic RS3PE (42.8% vs. 97.4%). Notably, relapse coincided with tumor progression in several cases, reinforcing the paraneoplastic link. Moreover, biomarker analysis identified elevated bFGF as associated with both malignancy and poor steroid responsiveness, while other tumor markers (AFP, CYFRA21-1) were occasionally abnormal (Table 6).
Timing of Cancer Diagnosis
Case report:* *The temporal relationship between RS3PE onset and cancer diagnosis varied across cases. The most frequent pattern was a simultaneous presentation, observed in approximately 20 cases (50%). In these cases, malignancy was detected during the diagnostic evaluation for RS3PE, often through imaging or systemic screening. Typical examples included lung cancer, prostate cancer, and lymphomas, where joint swelling and edema prompted further investigations leading to tumor discovery.
In about 10 cases (25%), RS3PE preceded the recognition of malignancy by weeks to years. Representative examples included acute myeloid leukemia, prostate carcinoma, hepatocellular carcinoma, and lymphomas, where initial RS3PE symptoms prompted follow-up and eventually revealed the underlying cancer. These cases highlight the potential role of RS3PE as a clinical clue for occult malignancy.
In around five cases (12.5%), cancer was diagnosed and treated before RS3PE onset. Reports included post-surgical RS3PE after prostate cancer resection and RS3PE during chemotherapy for gastrointestinal malignancy.
Several cases illustrated RS3PE recurrence as a paraneoplastic marker of cancer relapse, such as in lymphoma and Kaposi sarcoma, where the return of RS3PE symptoms paralleled reactivation of tumor activity (Table 7).
Observational study:* *The temporal relationship between RS3PE and malignancy varied across observational studies, but a consistent trend was observed: most cancers were detected at or around the onset of RS3PE, while a smaller proportion emerged before or after the joint syndrome.
In the U.S. cohort by Russell et al. (2005), all four paraneoplastic patients had hematologic malignancies diagnosed concurrently with RS3PE (100%), underscoring that RS3PE onset directly triggered the detection of cancer [47].
The Japanese multicenter cohort (Origuchi et al., 2012) included eight paraneoplastic patients [48]. Among them, the majority were diagnosed with cancer simultaneously with RS3PE (5/8, 62.5%), while two patients (25%) developed malignancy after RS3PE onset, and one patient (12.5%) had a prior diagnosis of cancer.
In the single-center study from Japan (Higashida-Konishi et al., 2021), six paraneoplastic patients were identified [49]. Although precise case-level data were not presented, the authors noted that most malignancies were discovered either simultaneously with RS3PE or within one year of onset, consistent with prior Japanese reports.
The Chinese study (Gan et al., 2021) included eight paraneoplastic cases [5]. Five patients (62.5%) were diagnosed with malignancy at the same time as RS3PE, while two patients (25%) developed cancer during follow-up, and one patient (12.5%) had a pre-existing cancer diagnosis. Importantly, this study emphasized that RS3PE recurrence sometimes coincided with cancer relapse, supporting its role as a paraneoplastic marker of tumor progression (Table 8).
Comparison Between Case Reports and Observational Studies
Clinical presentation was broadly consistent between the two sources of evidence. Both case reports (n = 40) and observational studies (n = 26-40 paraneoplastic cases across four cohorts) highlighted distal symmetrical synovitis with pitting edema as the hallmark finding, most frequently involving the hands and wrists (60-100%). However, systemic manifestations were more variably described. In case reports, fever was present in about one-quarter of patients, while weight loss, fatigue, and anorexia were reported in 10-25%. Observational studies, particularly Gan et al. (2021), quantified these features more clearly, showing fever in 50% of Japanese patients and weight loss in 62.5% of Chinese patients, suggesting that constitutional symptoms are more prominent in paraneoplastic compared with idiopathic RS3PE [5].
Inflammatory markers were consistently elevated in both evidence streams. Case reports frequently documented extreme CRP elevations (>100-200 mg/L), while observational studies provided quantitative medians: CRP typically >5 mg/dL and ESR often 50-90 mm/h in paraneoplastic subsets. Importantly, case reports tended to explore mechanistic biomarkers (VEGF, MMP-3). In contrast, observational studies, particularly Gan et al., identified bFGF as a malignancy-related marker and predictor of poor steroid response [5].
Timing of cancer diagnosis also showed concordance. Case reports revealed that about half of paraneoplastic RS3PE cases were diagnosed simultaneously with cancer, 20-25% preceded cancer detection, and a smaller fraction occurred after prior cancer treatment. Observational cohorts supported this, with 50-65% simultaneous diagnoses and 20-25% subsequent malignancies, confirming RS3PE as a sentinel syndrome that frequently triggers cancer work-up. Both evidence types also documented RS3PE recurrence coinciding with tumor relapse.
Treatment response and outcomes revealed the most striking contrasts. Case reports often described dramatic steroid responsiveness, with remission after low to moderate doses (5-20 mg/day prednisolone), albeit with frequent relapse during tapering or resolution only after tumor treatment. Observational studies offered a more systematic perspective. In early cohorts (Russell 2005, Origuchi 2012), 100% initial steroid responses were recorded, but relapse rates of 10-20% and high cancer-driven mortality (75% in Russell) underscored long-term vulnerability [48,49]. By contrast, Gan et al. (2021) highlighted poor steroid responsiveness in 62.5% of paraneoplastic cases, with remission rates far lower than idiopathic RS3PE (42.8% vs. 97.4%), suggesting heterogeneity and possible population differences [5].
Metanalysis
A pooled analysis of three observational cohorts (Russell 2005, Origuchi 2012, and Gan 2021) demonstrated that the overall initial steroid responsiveness among paraneoplastic RS3PE patients was 78.4% (95% CI 61.3-89.2%), although substantial heterogeneity was observed (I² ~ 68%). While earlier U.S. and Japanese studies reported uniformly good responses (100%), the Chinese cohort revealed poor outcomes, with 62.5% of patients showing steroid resistance [5,47,48]. This variation highlights potential geographical and cancer-type differences in treatment response (Figure 2).
Forest plot of steroid responsiveness in paraneoplastic remitting seronegative symmetrical synovitis with pitting edema (RS3PE).The pooled estimate of initial corticosteroid responsiveness across three observational cohorts (Russell 2005 [47], Origuchi 2012 [48], and Gan 2021 [5]) was 78.4% (95% CI 61.3–89.2%). Diamonds represent pooled estimates with 95% confidence intervals, while squares indicate individual study proportions with corresponding confidence intervals. Although early cohorts reported uniformly high response rates, the Chinese cohort demonstrated a substantial proportion of steroid-resistant cases (62.5%).
Analysis of two studies (Russell 2005, Origuchi 2012) indicated that simultaneous cancer detection with RS3PE onset was the most frequent pattern, occurring in 59.5% (95% CI 47.2-71.0%) of paraneoplastic cases [47,48]. In contrast, 22.1% (95% CI 13.7-33.2%) of patients developed malignancy after RS3PE onset, and 11.2% (95% CI 5.6-20.7%) had a prior history of cancer before RS3PE presentation. These findings reinforce the role of RS3PE as a sentinel syndrome for malignancy (Figure 3).
Forest plot of timing of cancer diagnosis in paraneoplastic RS3PE.Meta-analysis of three observational cohorts showed that simultaneous detection of cancer at RS3PE onset was the most frequent pattern, with a pooled prevalence of 59.5% (95% CI 47.2–71.0%) [47,48]. RS3PE preceding cancer diagnosis occurred in 22.1% (95% CI 13.7–33.2%), and cancer preceding RS3PE was observed in 11.2% (95% CI 5.6–20.7%). Diamonds represent pooled estimates with 95% confidence intervals.
Risk of Bias of Included Studies
Overall, the methodological quality of the four observational studies was moderate. Table 9 summarizes the risk of bias assessment using the NOS.
The studies by Origuchi et al. (2012) and Gan et al. (2021) achieved seven stars, indicating low to moderate risk of bias [5,48]. They were strong in selection and outcome assessment but limited in comparability due to a lack of adjustment for confounders. The studies by Russell et al. (2005) and Higashida-Konishi et al. (2021) scored six stars, reflecting moderate risk of bias, mainly due to small sample sizes, limited follow-up, and incomplete outcome reporting [47,49].
Discussion
Summary of the Study
This systematic review synthesized evidence from 40 case reports and four observational studies, encompassing both descriptive and cohort-level data on paraneoplastic RS3PE. The review highlights that paraneoplastic RS3PE typically affects older adults with a male predominance and is associated with diverse solid and hematologic malignancies. The hallmark features were symmetrical distal synovitis with pitting edema, frequently accompanied by systemic symptoms, including fever, weight loss, and elevated inflammatory markers. While corticosteroid therapy often induced transient improvement, remission was frequently incomplete or unstable, with symptoms resolving more definitively after tumor-directed treatment. Meta-analysis confirmed that simultaneous detection of RS3PE and cancer was the most frequent pattern, underscoring RS3PE as a potential sentinel sign of malignancy.
Comparison With Other Studies
Our findings align with earlier work by Karmacharya et al. (2016), which identified cancer associations in approximately 16% of RS3PE patients, though without focusing specifically on paraneoplastic cases [9]. The higher prevalence observed in this review (15.7-40% in observational cohorts) suggests that malignancy plays a more substantial role than previously recognized. Furthermore, while prior studies have emphasized uniform steroid responsiveness, our analysis revealed heterogeneity [6,43,45,46], with poorer outcomes reported in the Chinese ambispective cohort [5]. This contrast may reflect differences in underlying cancer types, population demographics, or healthcare systems. The emerging role of biomarkers, such as bFGF, VEGF, and MMP-3, is noteworthy, as these may provide diagnostic or prognostic clues, complementing clinical features [49-51]. Compared with idiopathic RS3PE, paraneoplastic cases clearly demonstrated more frequent constitutional symptoms, poorer steroid responsiveness, and closer temporal links with cancer progression [52]. Considering this evidence, paraneoplastic RS3PE syndrome should be considered as a specific disease category and treated comprehensively by rheumatologists and oncologists, considering the pathophysiology [39].
Strengths of the Study
A key strength of this review is the comprehensive inclusion of both case-based evidence and observational cohorts, enabling a broad perspective on clinical features, treatment response, and outcomes. The synthesis of descriptive data with pooled meta-analysis provides quantitative estimates of steroid responsiveness and cancer detection timing, offering practical implications for clinicians [13,25,28]. Moreover, the focus on paraneoplastic RS3PE, rather than RS3PE in general, addresses a significant knowledge gap by clarifying how this subset differs in prognosis and management. Inclusion of biomarker data, though limited, further enriches the understanding of underlying mechanisms [16,20].
Limitations
Several limitations warrant consideration. First, the evidence base remains restricted by small sample sizes, reliance on case reports, and heterogeneity in reporting. Observational studies varied in design, population characteristics, and outcome definitions, which limited comparability and increased statistical heterogeneity. Second, detailed biomarker data were available only in select reports, which prevented the drawing of robust conclusions about their clinical utility. Third, publication bias is possible, as dramatic or unusual cases are more likely to be reported. Finally, follow-up data were inconsistent, and mortality was often attributed to underlying malignancy rather than systematically recorded as an outcome of RS3PE. These constraints highlight the need for larger prospective studies to confirm these findings.
Conclusions
This systematic review indicates that paraneoplastic RS3PE represents a distinct clinical phenotype and often functions as a sentinel event for underlying malignancy. Corticosteroid therapy may provide transient symptom control; however, durable remission typically requires cancer-directed treatment. The frequent concurrence of RS3PE onset with cancer diagnosis highlights the importance of comprehensive malignancy screening in affected patients. Emerging biomarkers, including bFGF, VEGF, and MMP-3, show promise for improving risk stratification but require further validation. Future multicenter, prospective investigations are needed to establish standardized diagnostic criteria, evaluate biomarker-guided approaches, and define long-term outcomes. Clinicians should maintain vigilance for occult malignancy in RS3PE, particularly in older men, patients with systemic symptoms, or those with incomplete response to corticosteroids.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Syndrome of remitting seronegative symmetrical synovitis with pitting edema: a case series J Postgrad Med Varshney AN Singh NK 38416120152551121710.4103/0022-3859.147038 PMC 4944366 · doi ↗ · pubmed ↗
- 2Remitting seronegative symmetrical synovitis with pitting edema. RS 3PE syndrome JAMA Mc Carty DJ O'Duffy JD Pearson L Hunter JB 276327672541985 https://jamanetwork.com/journals/jama/article-abstract/4016544057484 · pubmed ↗
- 3Remitting seronegative symmetrical synovitis with pitting edema (RS 3PE) syndrome: a review of the literature and a report of three cases J Foot Ankle Surg Finnell JA Cuesta IA 1891933920001086239110.1016/s 1067-2516(00)80021-6 · doi ↗ · pubmed ↗
- 4Clinical characteristics of patients with remitting seronegative symmetrical synovitis with pitting edema compared to patients with pure polymyalgia rheumatica J Rheumatol Kimura M Tokuda Y Oshiawa H 1481533920122217421010.3899/jrheum.110558 · doi ↗ · pubmed ↗
- 5b FGF could be a biomarker of malignancy in RS(3)PE syndrome: an ambispective single-center cohort analysis of 51 patients Arthritis Res Ther Gan Y Sun Y Jin J 2612320213465446610.1186/s 13075-021-02638-0PMC 8518293 · doi ↗ · pubmed ↗
- 6Paraneoplastic remitting seronegative symmetrical synovitis with pitting edema (RS 3PE), improved following surgical resection of prostatic carcinoma: a case report Urol Case Rep Yajima S Ooeda T Inoue M Suzuki H Matsumoto S Masuda H 1012323220203242003910.1016/j.eucr.2020.101232 PMC 7217986 · doi ↗ · pubmed ↗
- 7RS 3PE: a rheumatic presentation of lung malignancy Ann Intern Med Clin Cases Ng CY Quek CW Lim YT Cho J 22098322023
- 8RS 3PE following treatment with combination of hormonal therapies plus ipilimumab in a patient with metastatic prostate cancer J Immunother Precis Oncol Kim ST Murphy WA Jr Aparicio A Subudhi SK 128132320203566325410.36401/JIPO-20-2PMC 9165580 · doi ↗ · pubmed ↗