The Diagnostic Pitfalls of Invasive Breast Lobular Carcinomas Around Involuting Fibroadenomas With Coarse Calcifications: A Case Report
Taisuke Yagyu, Shoji Oura

TL;DR
A case report shows how invasive lobular breast cancer can develop around a calcified fibroadenoma and be missed on certain mammograms.
Contribution
Highlights a diagnostic challenge where invasive lobular carcinoma is masked by calcified fibroadenoma on mammography.
Findings
Invasive lobular carcinoma was found around a calcified fibroadenoma despite normal MLO mammography.
MRI and ultrasound features helped identify the tumor, leading to a biopsy and diagnosis.
Post-surgery pathology confirmed multiple ILC foci near the fibroadenoma with hormone receptor positivity.
Abstract
A 69-year-old female with an involuting fibroadenoma (FA) was referred to our hospital for detailed examination of mammographic abnormalities around the coarse calcifications. Despite the lack of meaningful findings on medio-lateral oblique (MLO) view mammography, cranio-caudal (CC) view mammography showed spiculae around the calcifications. Ultrasound showed an oval mass with indistinct margins, disruption of the anterior borders of the mammary gland, and haloes just above the disruption areas. MRI depicted an irregular mass that showed low signals on T1-weighted images, slightly high signals on fat-suppressed T2-weighted images, and a plateau pattern on dynamic studies. Under the tentative diagnosis of breast cancer around the calcified FA, we performed a vacuum-assisted biopsy of the target lesion. Pathological examination showed small atypical cells growing in linear and scattered…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
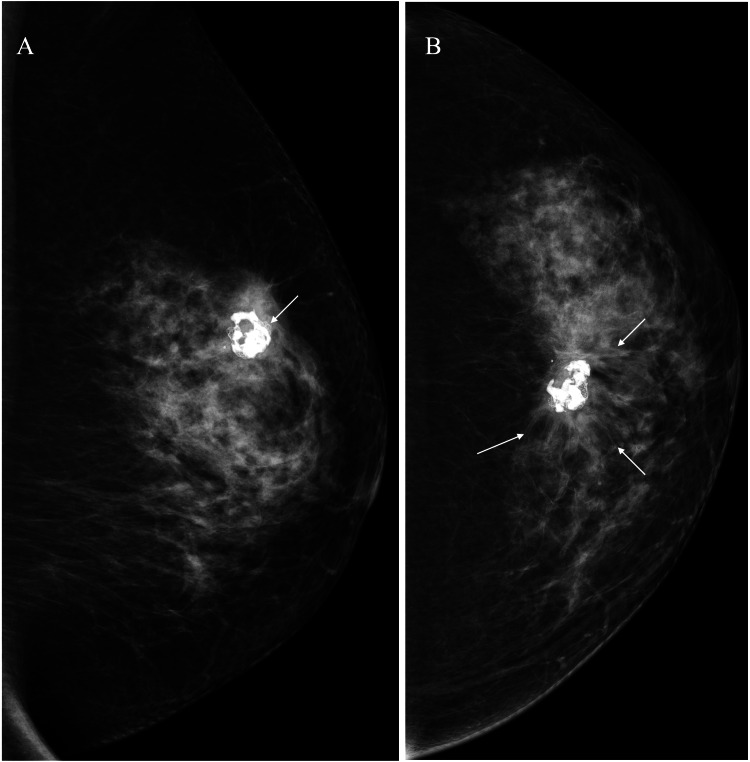 Figure 1
Figure 1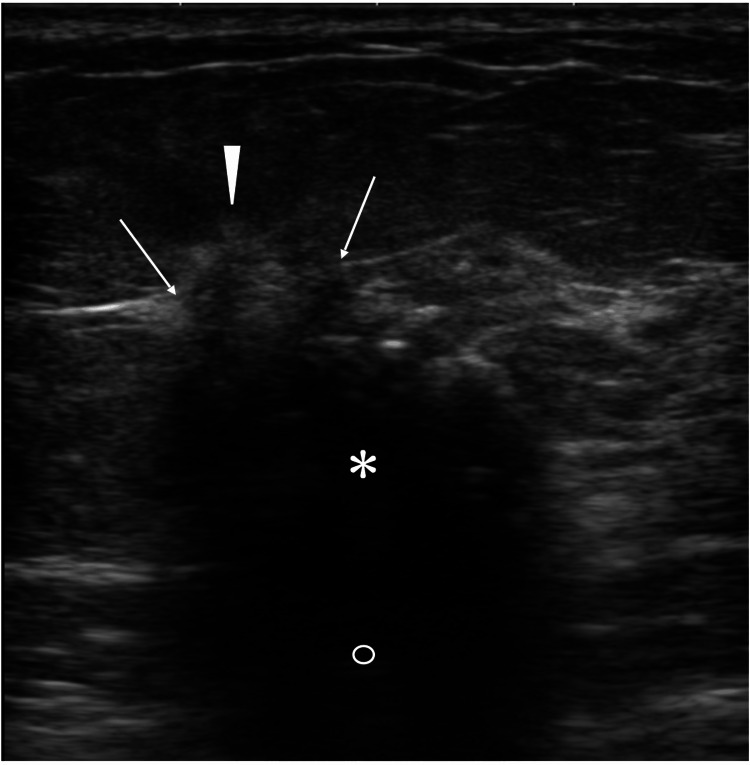 Figure 2
Figure 2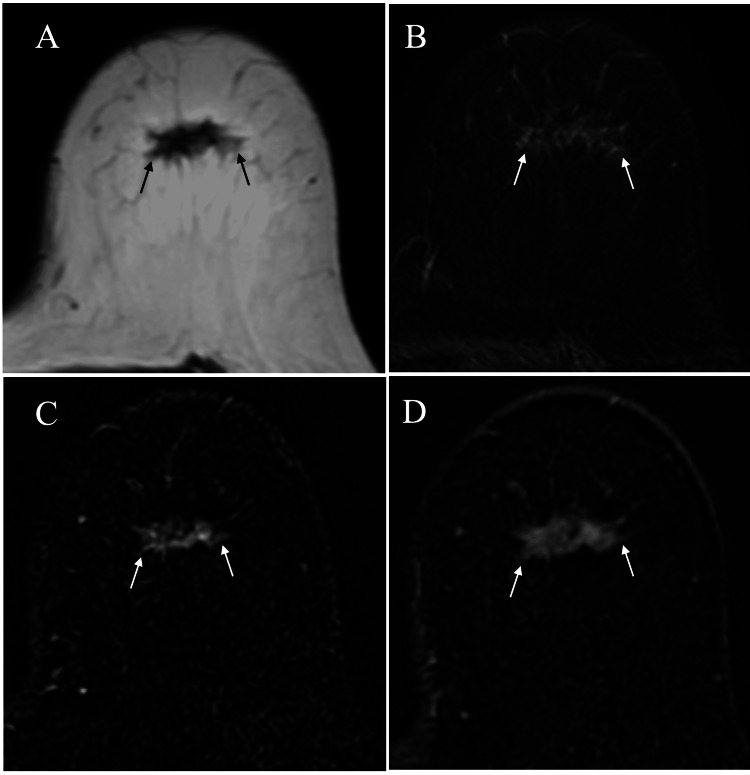 Figure 3
Figure 3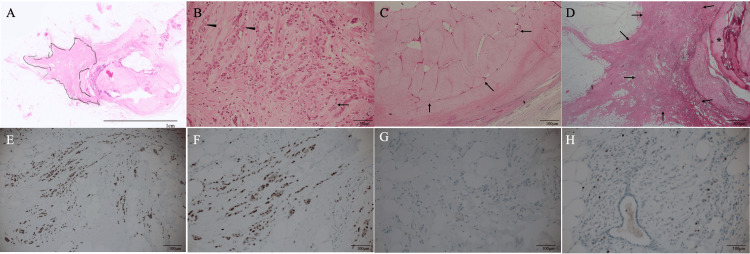 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreast Lesions and Carcinomas · Cancer and Skin Lesions · Breast Cancer Treatment Studies
Introduction
Invasive lobular carcinomas (ILCs) naturally develop from mammary lobules. They can be multicentric and bilateral, and characteristically metastasize to rare organs and sites such as the gastrointestinal tract and retroperitoneum [1,2]. ILCs generally have abundant fibrous components, which can cause distortion of the mammary gland and give ILCs a hardness. Scirrhous-type invasive ductal carcinomas also have a large amount of fibrous components, often leading to challenges in terms of differential diagnosis between scirrhous carcinomas and ILCs, not only pathologically but also radiologically. Scirrhous-type invasive ductal carcinomas, however, less often have multicentricity and bilaterality, and rarely develop distant metastasis to uncommon organs and tissues.
Fibroadenomas (FA) have both epithelial and connective tissue components and are the most common benign breast tumors. Despite the known frequent harboring of MED12 mutations [3], i.e., a gene encoding part of the RNA polymerase II mediator complex found in more than half of uterine myomas, the exact pathogenesis of FA remains unknown. Fibroadenomas grow in an estrogen-dependent manner and, therefore, do not grow larger after menopause, and frequently develop coarse calcifications [4]. Similar to ILCs, fibroadenomas develop from mammary lobules. Nevertheless, it is rare for breast cancer to develop within fibroadenomas, and when it does, it is most often ductal carcinoma in situ [5]. No studies, however, have reported a lobular carcinoma encompassing a calcified FA to date. We report a case of ILC surrounding a calcified fibroadenoma, which had obscured the ILC.
Case presentation
A 69-year-old female with no particular medical history, whose mother had a history of pancreatic cancer, had been aware of a benign tumor in her left breast for more than 20 years. She was referred to our hospital due to the abnormal mammography findings around the benign tumor. Mammography showed a dense breast pattern and no abnormalities except for the coarse calcifications on the medio-lateral oblique (MLO) view. Cranio-caudal (CC) view mammography, however, showed spiculae around the calcifications (Figure 1).
Mammography findings(A) Medio-lateral oblique view mammography only showed coarse calcifications (arrow). (B) Cranio-caudal view mammography showed evident distortion (arrows) around the calcifications
Ultrasound showed an oval mass, 18 mm in size, with indistinct margins, disruption of the anterior borders of the mammary gland, and haloes just above the disruption areas (Figure 2).
Ultrasound findingsUltrasound showed an oval mass (asterisk) with indistinct margins, internal low echoes, attenuated posterior echoes (open circle), disruption of mammary gland anterior borders (arrows), and focal haloes (arrowhead)
MRI depicted an irregular mass that showed low signals on T1-weighted images, slightly high signals on fat-suppressed T2-weighted images, and a plateau pattern on dynamic studies (Figure 3).
MRI findingsMRI of the mass showed low signals (arrows) on T1-weighted images (A), faint high signals (arrows) on T2-weighted images (B), and early (C) and retained (D) enhancement (arrows) on dynamic studiesMRI: magnetic resonance imaging
Under the tentative diagnosis of breast cancer around the calcified FA, we performed a vacuum-assisted biopsy of the target lesion. Pathological examination showed small atypical cells growing in linear and scattered fashions with connective tissue proliferation, leading to the diagnosis of ILC. Immunostaining showed that the ILC was a luminal subtype breast cancer with a low proliferating index. Based on the patient's wishes, we operate on the patient with nipple sparing mastectomy and sentinel node biopsy, followed by immediate breast reconstruction using the extended latissimus dorsi musculocutaneous flap. Postoperative pathological study revealed four ILC foci up to 18 mm in size and an intracanalicular type FA with massive calcifications. Immunostaining showed estrogen and progesterone receptor positivity (both with an Allred score of 8), human epidermal growth factor receptor type 2 negativity, and a low Ki-67 labelling index of 5% (Figure 4).
Pathological findings(A) Low magnified view showed invasive lobular carcinoma cells (closed areas) and the involuting fibroadenoma (asterisk) (H.E. ×4). (B) Magnified view showed atypical cells growing in linear (arrow) and cord-like (arrowheads) fashions against the abundant fibrous backgrounds (H.E. ×200). (C) Fibroadenoma (arrows) was of an intracanalicular phenotype (H.E. ×40). (D) Atypical cells (arrows) surrounded the coarse calcifications (asterisk) (H.E. ×40). (E) Immunostaining showed that invasive lobular carcinoma cells (brownish cells) had high estrogen receptor positivity (×200). (F) Immunostaining showed that invasive lobular carcinoma cells (brownish cells) had high progesterone receptor positivity (×200). (G) Tumor cells showed no positivity of human epidermal growth factor receptor on immunostaining (×200). (H) Tumor cells had a low Ki-67 labelling index of 5% (×200)
The patient recovered uneventfully; she was discharged on the 14th day after the operation and is scheduled for a 10-year outpatient follow-up on endocrine therapy.
Discussion
Coarse calcifications observed in this case could be either dystrophic calcifications or those developed in postmenopausal involuting fibroadenomas. Dystrophic calcifications can develop through various mechanisms, such as surgery to the breast and degenerative changes of the mammary gland. Especially, breast surgery can cause spiculae around the operative site, which often mimic breast cancer-induced spiculae. Coarse calcifications after breast surgery, however, are generally accompanied by evident surgery-related ultrasound findings and, therefore, were easily negated in this case. Coarse calcifications are naturally composed of calcium. Large calcifications have such high acoustic impedance that they reflect almost all ultrasound waves, preventing the diagnostic physicians from properly evaluating the tissue under the large calcifications on ultrasound. On the other hand, calcifications have a high X-ray attenuation coefficient on mammography, showing them as white and making small lesions in front of or behind them, and are often overlooked, like in this case.
Unlike pleomorphic ILCs [6], classic ILCs generally have better clinical outcomes than invasive ductal carcinomas [7]. In fact, the Ki67 labelling index was very low at 5% in this case. Due to the lack of detailed information about our patient's past screening mammography, we could not evaluate how coarse calcifications had obscured this less aggressive ILC. However, it cannot be denied that the Japanese standard screening mammography method, i.e., MLO view mammography without CC view mammography for patients aged 50 years or older [8], might have led to the underdetection of ILC in this case.
It is well known that MLO view mammography shows the breast in a more expanded form than CC view mammography. Many diagnostic physicians, however, have empirically known that the ILCs are more clearly visualized on CC view mammography than on MLO view mammography. Unfortunately, no research has proved to date why this phenomenon occurs. Clear tumor margins may be obscured by overlapping with the mammary gland and can often become evident by increased breast compression.
We have already clarified that fibrous components, when present at the mass borders mixed with cancer cells, can obscure tumor margins [9,10]. ILCs, therefore, have highly indistinct margins, which never become distinct with more breast compression. Conversely, when tumor margins show spicula-like structures, they become more unclear on the MLO view mammography due to the further magnification of unclear margins. In addition, the breasts are thinner on the MLO view mammography than on the CC view mammography, and make the mass opacity further lower, leading to more difficult identification of ILCs on MLO view mammography. These are presumably the main reasons why ILCs are less detectable on MLO view mammography.
Simple fibroadenomas are not known to increase the risk of breast cancer [11]. The clinical significance of why this ILC developed just around the calcified fibroadenoma is unclear. However, it is imperative that screening mammography with MLO and CC views be performed even for elderly people to avoid underdetection of ILCs around the coarse calcifications, if present.
Conclusions
Classic-type ILCs surrounding calcified fibroadenomas are extremely rare and can be overlooked on screening mammography. Therefore, if known calcified fibroadenomas are present, screening mammography should be performed by using both MLO and CC views, even for elderly people. In addition, diagnostic physicians should note that ILCs can be detected more easily on CC view mammography than MLO view mammography.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clinicopathologic characteristics of invasive lobular carcinoma of the breast: results of an analysis of 530 cases from a single institution Cancer Orvieto E Maiorano E Bottiglieri L 1511152011320081870498810.1002/cncr.23811 · doi ↗ · pubmed ↗
- 2Comparative analysis of lobular and ductal carcinoma of the breast: presentation, treatment, and outcomes J Am Coll Surg Winchester DJ Chang HR Graves TA Menck HR Bland KI Winchester DP 4164221861998954495510.1016/s 1072-7515(98)00051-9 · doi ↗ · pubmed ↗
- 3Mutational analysis of MED 12 in fibroadenomas and phyllodes tumors of the breast by means of targeted next-generation sequencing Breast Cancer Res Treat Mishima C Kagara N Tanei T 30531215220152609364810.1007/s 10549-015-3469-1 · doi ↗ · pubmed ↗
- 4Calcification in breast lesions: pathologists' perspective J Clin Pathol Tse GM Tan PH Pang AL Tang AP Cheung HS 1451516120081770426410.1136/jcp.2006.046201 · doi ↗ · pubmed ↗
- 5Breast carcinoma arising in a fibroadenoma: a case series of 16 patients and review of the literature Oncol Lett Xu L Luo S Mao Q Gao Y Luo L Qu W Cao Y 392720243811658010.3892/ol.2023.14172 PMC 10728692 · doi ↗ · pubmed ↗
- 6Invasive lobular breast carcinoma variants; clinicopathological features and patient outcomes Breast Cancer Res Treat Aktas A Gurleyik MG Akkus D Ucur Z Aker F 34735921220254039732110.1007/s 10549-025-07729-z PMC 12133914 · doi ↗ · pubmed ↗
- 7Distinct clinical and prognostic features of infiltrating lobular carcinoma of the breast: combined results of 15 International Breast Cancer Study Group clinical trials J Clin Oncol Pestalozzi BC Zahrieh D Mallon E 300630142620081845804410.1200/JCO.2007.14.9336 · doi ↗ · pubmed ↗
- 8Current status of screening for breast cancer and tasks for introduction of mammographic screening in Japan Breast Cancer Morimoto T Sasa M 227234519981109165310.1007/BF 02966701 · doi ↗ · pubmed ↗