Homologous Recombination Deficiency Testing in Women With Ovarian Cancer: An Egyptian Multicentre Study
Kyrillus S. Shohdy, Loay Kassem, Boules Gabriel, Emad Barsoum, Tamer Elnahas, Hamdy A. Azim

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
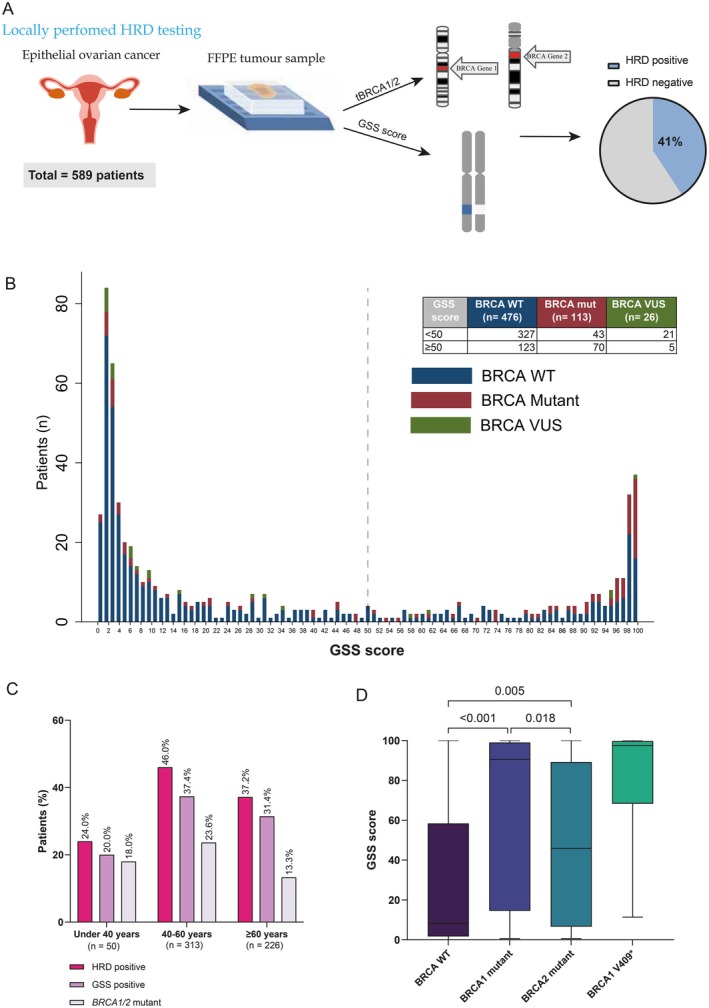 Figure 1
Figure 1- —Cancer Research UK10.13039/501100000289
- —Cairo University10.13039/501100002386
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPARP inhibition in cancer therapy · DNA Repair Mechanisms · BRCA gene mutations in cancer
Identification of patients with homologous recombination deficiency (HRD) is crucial for the better management of patients with epithelial ovarian cancer (EOC) [1]. In limited‐resource countries, there is a shortage of HRD testing outcomes due to costly testing, substandard infrastructure and lack of expert know‐how [2].
We conducted a multicentre registry study aiming to evaluate the feasibility and outcomes of in‐house HRD testing for patients with EOC in Egypt (Figure 1A). From 2019 to 2022, 589 consecutive patients with a median age of 56 years (range 20–86), from five cancer centres across Egypt, had undergone a successful HRD testing. The study was approved by the Institutional Review Board at Dar El Salam Cancer Centre (Ministry of Health and Population—Egypt).
HRD testing included BRCA1/2 tumour mutation status (tBRCA1/2) and genomic scar score (GSS) status. Briefly, for each FFPE sample submitted, DNA extraction was performed using QIAamp DNA Mini kit (QIAGEN). Then, appropriate libraries preparation according to the manufacturer's protocol with the AmoyDx HRD Panel (Amoy Diagnostics Co. Ltd.) and sequencing was performed using the Illumina NextSeq500 system (Illumina). A custom hybridisation capture panel that targets 27 000 SNPs distributed across the genome was used to infer the GSS. Patients with BRCA1/2 mutations or GSS ≥ 50 (i.e., GSS‐positive) were considered HRD‐positive as previously validated [3] (Figure 1A).
GSS‐positive tumours were detected in 198 (33.6%) of our patients while tBRCA1/2 mutations were detected in 113 (19.2%) (Figure 1B). Collectively, 241 patients (41%) were diagnosed as HRD‐positive EOC at a median turnaround time of 13 days (range 8–26 days).
We examined the contribution of the GSS score and tBRCA1/2 status to the overall HRD positivity (Figure 1B). In total, 128 patients (21.7%) were positive due to a positive GSS score alone without identified tBRCA1/2 mutations. Meanwhile, 43 (7.3%) were HRD‐positive due to having BRCA1/2 mutations with a negative GSS score. Expectedly, the majority (62%) of patients with BRCA mutations had a positive GSS score, and the majority (80.7%) of patients with BRCA variants of uncertain significance (VUS) were GSS‐negative (Figure 1B).
There was no significant difference in HRD‐positive rate in younger age (< 50‐year‐old) compared to older (63 (38.2%) vs. 178 (42%), p = 0.42) neither in the rate of GSS‐positive (51 (30.9%) vs. 147 (34.7%), p = 0.38). However, we identified a significant trend for increasing the rate of HRD‐positive across age categories with the highest at age category 40 to < 60 years and lowest at under 40 years (46% vs. 24%, p trend = 0.034) (Figure 1C).
We also examined the differences among BRCA1/2 mutations in relation to the GSS score. Intriguingly, patients with BRCA1 mutations had significantly higher median GSS scores compared to the BRCA2 mutant patients (90 vs. 46, p = 0.018) (Figure 1C). The top recurrent mutation was BRCA1 V409*, which was associated with the highest median GSS score of 97 (Figure 1D). It is noteworthy that the three Ashkenazi Jewish pathogenic founder mutations were not detected in our cohort. Taken together, our findings suggest a differential phenotypic impact of BRCA1 mutations compared to BRCA2 mutations.
Several reports have shown high concordance of in‐house HRD testing compared with central testing using Myriad MyChoice CDx [2, 4, 5]. The HRD rate in our cohort was similar to results from locally performed Myriad testing in a real‐world cohort [6]. However, the rate was relatively lower than what was reported in clinical trials, likely due to biomarker enrichment bias in these trials. To the best of our knowledge, this is the first report from limited resource settings aiming to bridge the gap in cancer care disparities. Locally performed HRD testing was found to be feasible and mitigated the high cost and lengthy turnaround time associated with central testing.
Author Contributions
K.S.S., L.K. and H.A.A.: conceptualization and study design. H.A.A., L.K., B.G., E.B. and T.E.: data curation and patient recruitment. B.G.: project administration. K.S.S. and L.K.: formal analysis. K.S.S.: writing – original draft. All authors: writing – review and editing.
Conflicts of Interest
K.S.S.: outside of this scope of work, has received research funding from Novartis Pharma AG Basel, Cellular Therapeutics Limited, InstillBio and Adaptimmune. L.K. received honoraria from Roche, AstraZeneca, Novartis, Jansen, Pfizer, Eva, Sandoz, Hikma and MSD. H.A.A. received honoraria from Roche, AstraZeneca, Novartis, Jansen, Pfizer, Eva, Sandoz, Hikma and MSD. All other authors have no conflicts of interest to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A. González‐Martín , B. Pothuri , I. Vergote , et al., “Niraparib in Patients With Newly Diagnosed Advanced Ovarian Cancer,” New England Journal of Medicine 381, no. 25 (2019): 2391–2402.31562799 10.1056/NEJ Moa 1910962 · doi ↗ · pubmed ↗
- 2G. Magliacane , E. Brunetto , S. Calzavara , et al., “Locally Performed HRD Testing for Ovarian Cancer? Yes, We Can!,” Cancers (Basel) 15, no. 1 (2022): 43.36612041 10.3390/cancers 15010043 PMC 9817883 · doi ↗ · pubmed ↗
- 3W. Yuan , J. Ni , H. Wen , et al., “Genomic Scar Score: A Robust Model Predicting Homologous Recombination Deficiency Based on Genomic Instability,” BJOG: An International Journal of Obstetrics and Gynaecology 129, no. S 2 (2022): 14–22.36485068 10.1111/1471-0528.17324 · doi ↗ · pubmed ↗
- 4C. Fumagalli , I. Betella , A. Ranghiero , et al., “In‐House Testing for Homologous Recombination Repair Deficiency (HRD) Testing in Ovarian Carcinoma: A Feasibility Study Comparing Amoy Dx HRD Focus Panel With Myriad my Choice C Dx Assay,” Pathologica 114, no. 4 (2022): 288–294.36136896 10.32074/1591-951X-791PMC 9624133 · doi ↗ · pubmed ↗
- 5N. Pfarr , K. von Schwarzenberg , D. Zocholl , et al., “High Concordance of Different Assays in the Determination of Homologous Recombination Deficiency‐Associated Genomic Instability in Ovarian Cancer,” JCO Precision Oncology 8 (2024): e 2300348.38513168 10.1200/PO.23.00348 PMC 10965219 · doi ↗ · pubmed ↗
- 6C. Denkert , M. Romey , B. Swedlund , et al., “Homologous Recombination Deficiency as an Ovarian Cancer Biomarker in a Real‐World Cohort: Validation of Decentralized Genomic Profiling,” Journal of Molecular Diagnostics 24, no. 12 (2022): 1254–1263.10.1016/j.jmoldx.2022.09.00436191839 · doi ↗ · pubmed ↗