Late Ileocolic Anastomotic Stricture Due to Subserosal Lipoma: A Case Report
Yoichi Miyaoka, Shingo Shimada, Kazuhiro Ogasawara, Akinobu Taketomi

TL;DR
A rare case of a late ileocolic anastomotic stricture caused by a subserosal lipoma is reported, highlighting the need for early surgical intervention when endoscopic treatment fails.
Contribution
This case report identifies a subserosal lipoma as a rare cause of anastomotic stricture and emphasizes the importance of early surgical evaluation.
Findings
A subserosal lipoma was identified as the cause of an anastomotic stricture 10 years after ileocecal resection.
Endoscopic passage failed, necessitating surgical resection of the affected anastomotic segment.
Histology confirmed a benign subserosal lipoma without atypia or lipoblasts.
Abstract
Anastomotic strictures after ileocolic surgery are most often related to technical, ischemic, or inflammatory factors, with tumor recurrence also in the differential; a subserosal lipoma arising at the anastomosis is rare. We report a man in his 60s, 10 years after an ileocecal resection for appendicitis with abscess, who presented with right-sided abdominal pain and repeated vomiting. Contrast-enhanced CT demonstrated small-bowel wall hyperenhancement with fluid retention and a tight narrowing at the ileocolic anastomosis. After stabilization, colonoscopy showed edematous, ulcerated mucosa and a non-traversable stricture; biopsies revealed only inflammatory changes. Fluoroscopic balloon dilation was attempted, but guidewire cannulation failed, and conservative management was judged unlikely to succeed; therefore, the anastomotic segment was resected. Gross examination revealed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
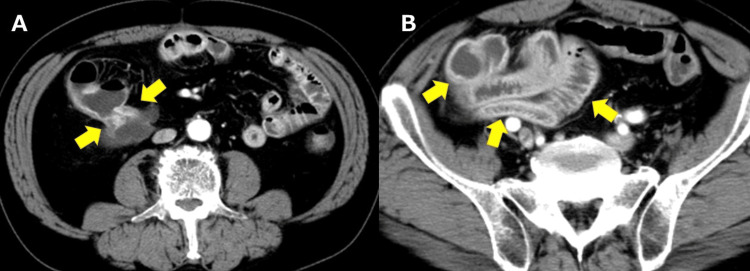 Figure 1
Figure 1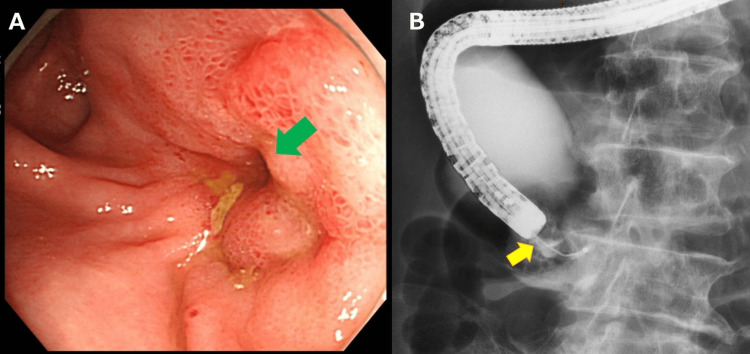 Figure 2
Figure 2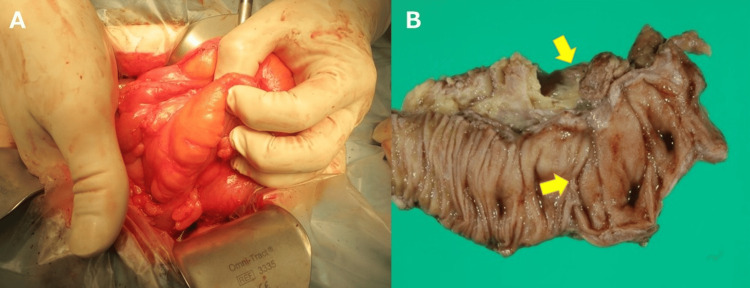 Figure 3
Figure 3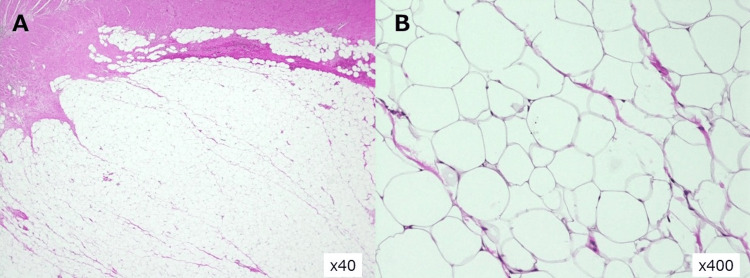 Figure 4
Figure 4| Authors | Country | Type | Year | Site and Layer | Presentation | Endoscopic Traversal | Management | Relevance to Present Case |
| Present case | Japan | CR | 2025 | Ileocolic anastomosis; subserosal | Fixed, non-traversable anastomotic stricture with pain/vomiting | Not traversable; biopsy inflammatory only; GW failed | Segmental resection incl. anastomosis; benign subserosal lipoma | Index case showing extramural (subserosal) lipoma at an anastomosis causing fixed stricture |
| Bronswijk et al. [ | Belgium | Systematic review | 2020 | Colon; predominantly submucosal, intraluminal | Obstruction/intussusception (bleeding less common) | Often traversable; variable | Endoscopic resection; surgery for broad-based/complicated lesions | Size/morphology-based selection framework; literature mainly intraluminal |
| Crocetti et al. [ | Italy | Systematic Review | 2014 | Colon; symptomatic lipomas | Larger size → more obstruction/intussusception | Variable (case-dependent) | Surgery favored when large/broad-based/complicated | Supports surgery in obstructive settings |
| Jiang et al. [ | China | CR | 2007 | Colon; submucosal giant lipoma | Obstruction from intraluminal mass | Usually visible/traversable endoscopically | Segmental resection | Intraluminal (submucosal) mechanism vs. our extramural (subserosal) |
| Mouaqit et al. [ | Morocco | CR | 2013 | submucosal; intraluminal | Obstruction due to intussusception | Not reported | Surgical resection | Comparator - intraluminal/intussuscepting lipoma vs. our extramural |
| Fiordaliso et al. [ | Italy | Narrative review | 2024 | Colonic lipoma overview | Patterns of obstruction/intussusception | Context-dependent | Algorithms for endoscopic vs. surgical strategies | Contemporary framework; anastomosis-specific cases rare |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Gastrointestinal Tumor Research and Treatment · Diverticular Disease and Complications
Introduction
Postoperative anastomotic stricture is a clinically relevant problem after ileocolic and colorectal surgery, with reported incidence varying widely (roughly 2-30%) according to definitions, anatomic site, and follow-up duration [1-3]. Major etiologies include technical factors (e.g., anastomotic diameter or tension), ischemia or leak-related scarring, and inflammatory conditions; in oncologic settings, recurrent tumor must also be excluded [1-3]. Strictures may present months to years after surgery and can lead to abdominal pain, vomiting, and obstructive symptoms that complicate endoscopic evaluation and delay definitive management.
Colonic lipomas are uncommon benign adipocytic tumors (estimated prevalence ~0.2-4.4%), the great majority (~90%) arising from the submucosa and projecting intraluminally; subserosal lesions constitute a minority [4,5]. Most symptomatic cases in the literature involve intraluminal bulk effects-bleeding, intermittent obstruction, or intussusception, where endoscopic visualization is often possible [4-6]. By contrast, extramural (subserosal) lipomas may present primarily through external compression, are more difficult to appreciate endoscopically, and are only sparsely represented in reviews. Within this context, a subserosal lipoma developing at a prior anastomosis and manifesting as a fixed, non-traversable anastomotic stricture appears exceedingly rare. This case highlights a distinct diagnostic challenge, as the extramural fatty component can mimic fibrotic or inflammatory stricture without mucosal abnormality.
We report a late ileocolic anastomotic stricture caused by a subserosal lipoma at a previous anastomosis, detailing the imaging-pathologic correlation and discussing practical implications for diagnosis and management. Unlike the more common intraluminal submucosal lipomas, a subserosal lipoma at a surgical anastomosis poses a diagnostic challenge because it produces extramural compression that may mimic fibrotic or inflammatory stricture without mucosal abnormality.
Case presentation
A man in his 60s with a history of ileocecal resection for appendicitis with abscess 10 years earlier presented with right-sided abdominal pain and repeated vomiting. On arrival, he was afebrile with localized right-flank tenderness and no peritoneal signs; laboratory tests showed a mild inflammatory response without organ dysfunction. Contrast-enhanced CT demonstrated a high-grade ileocolic anastomotic stricture with a fat-attenuating extramural component contiguous with the anastomosis (Figure 1A) and upstream small-bowel dilatation (Figure 1B).
Contrast-enhanced abdominal CT.(A, B) Axial images show a tight ileocolic anastomotic stricture with upstream small-bowel dilatation and mural hyperenhancement; low-attenuation tissue contiguous with the anastomosis (arrows) suggests an extramural fatty component.
The extramural component showed homogeneous fat attenuation with Hounsfield Unit values around -90 to -100 HU, consistent with mature adipose tissue. The patient had no prior postoperative imaging between the initial ileocecal resection and the current presentation. Upon admission, conservative therapy consisting of bowel rest and intravenous fluids was attempted for three days without improvement. The original anastomosis had been constructed in a side-to-side stapled fashion.
After stabilization, colonoscopy revealed edematous, ulcerated mucosa at a non-traversable anastomotic stricture (Figure 2A); mucosal biopsies showed inflammatory changes only. Under fluoroscopic guidance, balloon dilation was attempted, but guidewire cannulation across the stricture failed, and the procedure was aborted (Figure 2B).
Lower endoscopy and fluoroscopic contrast study.(A) Colonoscopy shows edematous, ulcerated mucosa and a non-traversable anastomosis (green arrow). (B) During attempted balloon dilation under fluoroscopy, guidewire could not be advanced across the stricture and the procedure was aborted; contrast pools proximally (yellow arrow).
Given the non-traversable nature of the lesion and the low likelihood of success with conservative/endoscopic measures, segmental resection, including the anastomosis, was performed.
Intraoperatively, the anastomotic segment was circumferentially thickened and constrictive (Figure 3A). The resected specimen showed extramural (subserosal) adipose tissue compressing the bowel wall with blunted mucosal folds (Figure 3B).
Operative and gross findings.(A) Intraoperative view of the circumferentially thickened and constrictive anastomotic segment. (B) Resected specimen shows extramural (subserosal) adipose tissue compressing the wall with blunted mucosal folds (arrows).
Histopathology (H&E) demonstrated nodular proliferation of mature adipocytes in the subserosa without atypia or lipoblasts, consistent with a benign subserosal lipoma (Figure 4).
Histopathology (H&E).(A) ×40: subserosal lipomatous proliferation compressing the muscularis-mucosal layers. (B) ×400: mature adipocytes without atypia or lipoblasts, consistent with a benign subserosal lipoma.
Oral intake resumed on postoperative day (POD) 1, diet advanced on POD 5, and the patient was discharged in good condition on POD 15.
Discussion
Late ileocolic anastomotic stricture is most often attributable to technical factors, ischemia, or leak-related scarring, inflammatory disease, or prior radiation; in oncologic settings, recurrent tumor must also be excluded [1-3]. In our patient, 10 years after ileocecal resection, the triad of a non-traversable anastomotic narrowing, biopsy-negative mucosa, and fat attenuation contiguous with the anastomosis on CT favored an extramural rather than intrinsic scar etiology. Resection confirmed a subserosal lipoma compressing the bowel without atypia. To the best of our knowledge, no previous reports have described an extramural (subserosal) lipoma developing at a gastrointestinal anastomotic site, making this case a unique presentation.
Table 1 summarizes the present case alongside representative case reports and reviews, emphasizing the layer of origin, anatomic site, endoscopic traversability, and management.
Most symptomatic colonic lipomas in prior reports are submucosal and intraluminal, often visible endoscopically and sometimes traversable, with obstruction driven by bulk or intussusception-typified by the case reports of Jiang et al. and Mouaqit et al. [6,7]. By contrast, our case derives from the subserosa (extramural) at a prior anastomosis, producing a fixed, non-traversable stenosis - an anatomic context that appears rarely documented. Reviews by Bronswijk and Crocetti et al. emphasize size/morphology-based selection between endoscopic and surgical therapy [4,5], while the contemporary narrative review by Fiordaliso et al. outlines patterns of obstruction/intussusception and treatment algorithms but likewise contains few anastomosis-specific examples [8]. Read alongside these sources, the present case broadens the differential for late anastomotic narrowing to include extramural (subserosal) lipoma.
From a diagnostic standpoint, CT characteristics of lipoma-homogeneous fat attenuation with minimal enhancement help distinguish it from other subepithelial lesions (SELs); when the fatty signal is contiguous with the anastomosis, it argues against a simple inflammatory scar and toward a lipomatous extramural process [4,7,9-11]. When clinical status allows, MRI can serve as a problem-solving adjunct: lipomas typically show high T1/T2 signal with marked signal loss on fat suppression and on opposed-phase imaging, aiding confirmation of fat, assessment of the layer of origin (submucosal vs. subserosal), and evaluation for any non-fatty enhancing components suggestive of alternative pathology (e.g., well-differentiated liposarcoma) [12,13]. In our patient, an MRI was not obtained because of acute obstruction, and the CT triad (fat contiguous with the anastomosis, non-traversable stricture, negative biopsies) already supported an extramural lipomatous etiology and prompted early surgery. Routine mucosal biopsies have low yield for deeper or extramural pathology, as guidance on SELs underscores [10,11].
Therapeutically, endoscopic balloon dilation (EBD) achieves high immediate success for benign colorectal or ileocolic strictures, but outcomes are poor when the stricture is non-traversable or caused by extrinsic compression [1,2,8,14-16]. In our patient, failed guidewire passage during attempted dilation predicted low endoscopic success and justified early surgery, which provided both definitive diagnosis and curative relief. Consistently, the systematic review by Crocetti et al. supports surgery for large/broad-based or complicated lipomas, and both Jiang and Mouaqit ultimately required segmental resection for obstructive disease despite intraluminal (submucosal) origin [5-7].
Although the concept of post-traumatic adipocytic proliferation has been described in soft-tissue literature [17], its application to gastrointestinal anastomoses remains speculative and should be interpreted cautiously.
The anastomotic interface is characterized by chronic scarring and low-grade mechanical irritation around sutures or staples, conditions that may provide a permissive niche for adipocytic proliferation in the subserosa. While still speculative in the gastrointestinal tract, this framework plausibly explains the emergence of an extramural lipoma at a prior anastomosis and the resulting fixed, non-traversable stenosis. Given the potential for extramural pathology to mimic fibrotic or inflammatory strictures, multidisciplinary evaluation - integrating radiologic pattern recognition (fat-attenuating components on CT/MRI), endoscopic assessment of traversability, and surgical judgment - can expedite accurate diagnosis and definitive treatment.
Putting this together, a practical heuristic for late anastomotic strictures is (i) scrutinize CT for a fat-attenuating component contiguous with the anastomosis; (ii) if the stricture is non-traversable and guidewire passage fails, prioritize operative management over repeated EBD; and (iii) in oncologic contexts, continue to exclude tumor recurrence in parallel [1-6,10,11].
This approach aligns with the aggregate signal from the literature while acknowledging that our case is an extramural, anastomosis-specific outlier relative to the predominantly intraluminal reports.
Limitations include the single-case nature of this report, the absence of (endoscopic ultrasound) EUS due to anatomic constraints at the ileocolic anastomosis, qualitative rather than prospective quantitative HU assessment, and the inability to pinpoint the exact site of origin within the adjacent bowel on the specimen. Nevertheless, the clinical course, imaging, and histology are coherent and mutually reinforcing.
Conclusions
This case suggests that when CT demonstrates a fat-attenuating lesion contiguous with a non-traversable anastomosis and biopsies are negative, early surgical resection may be preferable to repeated dilation. Multidisciplinary evaluation - combining radiologic pattern recognition and endoscopic assessment of traversability - can expedite accurate diagnosis and treatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Long-term results of endoscopic balloon dilation for treatment of colorectal anastomotic stenosis Surg Endosc Biraima M Adamina M Jost R Breitenstein S Soll C 443244373020162689591210.1007/s 00464-016-4762-8 · doi ↗ · pubmed ↗
- 2Long-term outcomes of endoscopic balloon dilation for benign strictures in patients with inflammatory bowel disease Gut Liver Lee HW Park SJ Jeon SR 5305361220182973090410.5009/gnl 17396 PMC 6143444 · doi ↗ · pubmed ↗
- 3Technical risk factors for benign anastomotic strictures in colorectal and/or coloanal anastomosis: a retrospective case-control study Colorectal Dis Garoufalia Z Meknarit S Emile SH 199620022620243935888310.1111/codi.17184 · doi ↗ · pubmed ↗
- 4Endoscopic treatment of large symptomatic colon lipomas: a systematic review of efficacy and safety United European Gastroenterol J Bronswijk M Vandenbroucke AM Bossuyt P 114711548202010.1177/2050640620948661 PMC 772453432746773 · doi ↗ · pubmed ↗
- 5Surgery for symptomatic colon lipoma: a systematic review of the literature Anticancer Res Crocetti D Sapienza P Sterpetti AV Paliotta A DE Gori A PedullàG de Toma G 62716276342014 https://pubmed.ncbi.nlm.nih.gov/25368224/25368224 · pubmed ↗
- 6Giant submucosal lipoma located in the descending colon: a case report and review of the literature World J Gastroenterol Jiang L Jiang LS Li FY Ye H Li N Cheng NS Zhou Y 566456671320071794894510.3748/wjg.v 13.i 42.5664 PMC 4172750 · doi ↗ · pubmed ↗
- 7Pedunculated lipoma causing colo-colonic intussusception: a rare case report BMC Surg Mouaqit O Hasnai H Chbani L Oussaden A Maazaz K Amarti A Taleb KA 511320132417170310.1186/1471-2482-13-51PMC 3818566 · doi ↗ · pubmed ↗
- 8Colonic lipoma, a rare cause of intestinal intussusception: a narrative review and how to diagnose it Medicine (Baltimore) Fiordaliso M Lovaglio UM De Marco FA Costantini R Nasti GA Lelli Chiesa P 0103202410.1097/MD.0000000000039579 PMC 1144195239331924 · doi ↗ · pubmed ↗