Therapeutic Challenges in Managing Triple-Negative Breast Cancer in a Patient With Central Core Disease
Fatima Ibrahim, Eeman Noor, Asfandyar Khalil, Usman Sehbai, Aasim Sehbai

TL;DR
This paper discusses the challenges of treating a patient with both central core disease and triple-negative breast cancer, emphasizing the need for careful monitoring and multidisciplinary care.
Contribution
The paper presents a novel case study highlighting the management of a patient with coexisting central core disease and breast cancer.
Findings
The patient completed treatment without exacerbation of her myopathy.
Multidisciplinary management and close monitoring were crucial for successful treatment.
Precautions during surgery helped prevent malignant hyperthermia.
Abstract
Central core disease (CCD) is a congenital myopathy characterized by muscle weakness, skeletal deformities, delayed motor milestones, and susceptibility to malignant hyperthermia. Symptoms of CCD can be exacerbated by various physiological and pharmacological triggers, necessitating careful monitoring, particularly during medical interventions. Breast cancer treatment typically involves modalities such as surgery, radiation, chemotherapy, immunotherapy, and endocrine therapy, all of which may exacerbate underlying myopathic conditions. Chemotherapy and immunotherapy especially have the potential of causing myopathy, myositis, or rhabdomyolysis. Therefore, patients with CCD undergoing breast cancer treatment require vigilant surveillance to mitigate the risks associated with disease exacerbation. We report the case of a 41-year-old female patient with coexisting CCD and breast cancer who…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
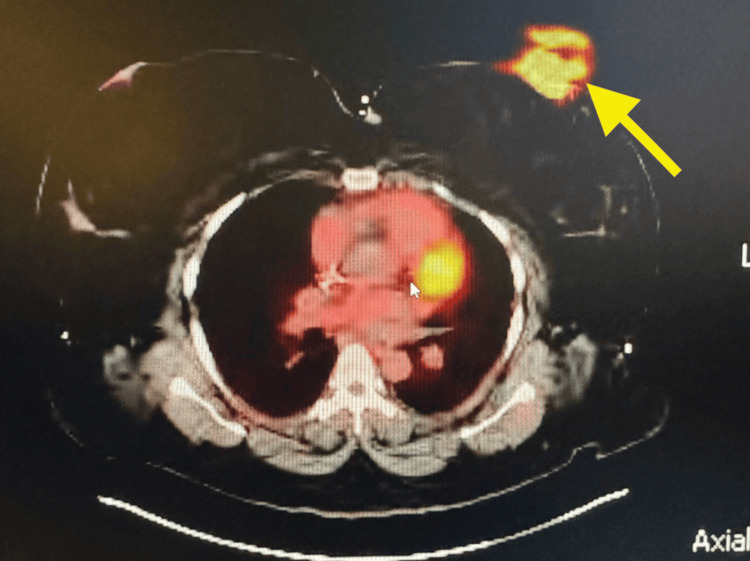 Figure 1
Figure 1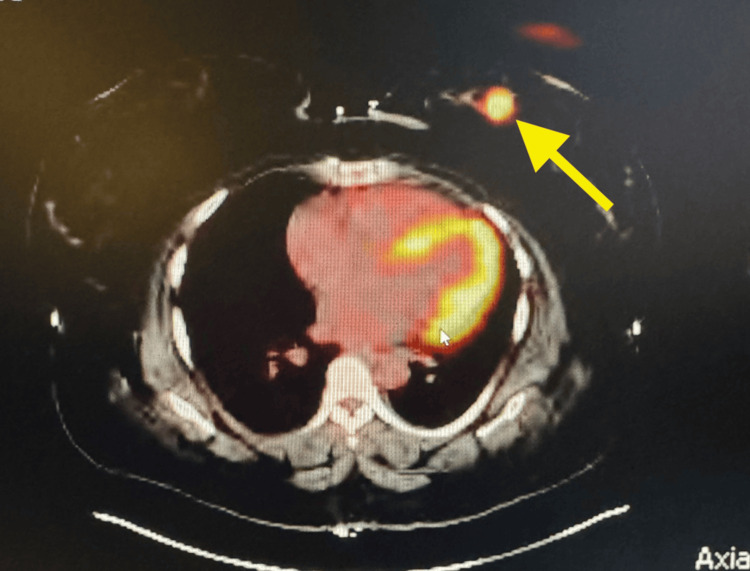 Figure 2
Figure 2| Phase | Date(s) | Medications | Notes |
| Neoadjuvant (Keynote-522) | Feb-May 2024 | Keytruda + Paclitaxel (Taxol) + Carboplatin | 4 cycles: Keytruda q3w, Taxol/Carbo on D1, D8, D15 |
| Post-neoadjuvant chemotherapy | May-July 2024 | Epirubicin + Cyclophosphamide (Cytoxan) + Keytruda | 4 cycles: Every 21 days, with Neulasta support |
| Supportive therapy | Ongoing | Iron, B12, Folic Acid, Gabapentin, Zofran, Imodium | To manage anemia, neuropathy, and chemo side effects |
| Radiation therapy | Jan-Apr 2025 | External Beam Radiation | Completed; postmastectomy radiation |
| Maintenance immunotherapy | Ongoing through mid-2025 | Keytruda q3w | 9 total cycles post-surgery; 2 remaining as of April 2025 |
| Surgery | Jan 2025 | Bilateral mastectomy + sentinel node biopsy | Reconstruction planned |
| Date | CK (U/L) | Myoglobin (ng/mL) | Aldolase (U/L) | Notes | ||||||
| Pt value | Normal range | Threshold | Pt value | Normal range | Threshold | Pt value | Normal range | Threshold | ||
| 03/2024 | 105 | 22-198 | >5,000 U/L | 40 | 25-72 | >300 ng/mL | 3.5 | 1.0-7.5 | >20-25 U/L | Baseline pre-therapy |
| 05/2024 | 190 | 22-198 | >5,000 U/L | 69 | 25-72 | >300 ng/mL | 6.8 | 1.0-7.5 | >20-25 U/L | Post-epirubicin + cytoxan |
| 08/2024 | 175 | 22-198 | >5,000 U/L | 68 | 25-72 | >300 ng/mL | 5.2 | 1.0-7.5 | >20-25 U/L | Post-chemo, pre-surgery |
| 01/2025 | 193 | 22-198 | >5,000 U/L | 73 | 25-72 | >300 ng/mL | 7.3 | 1.0-7.5 | >20-25 U/L | Post-surgery |
| 04/2025 | 145 | 22-198 | >5,000 U/L | 55 | 25-72 | >300 ng/mL | 4.0 | 1.0-7.5 | >20-25 U/L | End of radiation |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreast Cancer Treatment Studies · Advanced Breast Cancer Therapies · Cancer Treatment and Pharmacology
Introduction
Breast cancer remains one of the most common cancers among women in the United States, with approximately one in eight affected during their lifetime [1]. Among its various subtypes, triple-negative breast cancer (TNBC) is considered the most aggressive. Although relatively uncommon, representing about 10-15% of all breast cancer cases, TNBC is known for its rapid growth and high potential for metastasis. A 23% risk of recurrence and metastasis has been seen with TNBC, significantly higher than that seen with other subtypes of breast cancer [2]. Given its aggressive nature, it is important to understand TNBC, its clinical presentation, and treatment options [3].
TNBC differs from the other subtypes in that it lacks expression of the three key receptors commonly involved in breast cancer growth: estrogen, progesterone, and human epidermal growth factor receptor 2 (HER2) [3]. Due to the absence of these targets, TNBC is associated with a poor prognosis and more limited treatment options compared to other forms of breast cancer. Current therapeutic approaches often include neo-adjuvant chemotherapy and immunotherapy, followed by surgery and radiation [4]. However, in patients with pre-existing myopathy, such treatments may worsen symptoms such as muscle weakness and peripheral neuropathy or lead to anesthetic complications, further restricting available therapies.
Central core disease (CCD) is a rare congenital myopathy characterized by the presence of central cores on muscle biopsy [5]. It is most commonly associated with mutations in the skeletal muscle ryanodine receptor (RYR1) gene, which predisposes patients to malignant hyperthermia, a potentially fatal reaction triggered by certain anesthetic agents and muscle relaxants [5]. CCD can also present as varying degrees of muscle weakness, hypotonia, skeletal abnormalities, mild facial weakness, and respiratory issues causing increased risk of respiratory infections. Additionally, some chemotherapeutic agents contribute to the loss of body mass and skeletal muscle atrophy, leading to cachectic myopathy [6]. In rare cases, chemotherapy as well as immunotherapy can also induce rhabdomyolysis, posing further risk for individuals with CCD [6,7]. However, neoadjuvant pembrolizumab + chemotherapy followed by adjuvant pembrolizumab confers benefits in response and survival outcomes versus alternative neoadjuvant treatments for early-stage TNBC [8]. Hence, patients with CCD and early-stage TNBC who require cancer treatment need appropriate adjustments and frequent monitoring.
In this report, we present the unique case of a patient with TNBC and CCD, where the treatment approach required careful modification to accommodate her underlying neuromuscular condition.
Case presentation
A 41-year-old African-American female patient initially presented with a palpable left breast mass and associated discomfort. She was enrolled in the Alabama Breast and Cervical Cancer Early Detection Program (ABCCEDP), where a bilateral screening mammogram revealed a 2.5 cm mass in the lower inner quadrant (LIQ) of her left breast. A follow-up diagnostic mammogram and ultrasound demonstrated a 2.9 × 1.8 cm hypoechoic mass with microlobulated margins and associated left axillary lymphadenopathy, categorized as Breast Imaging Reporting and Data System Category 5 (BI-RADS 5). A core needle biopsy confirmed TNBC with estrogen receptor (ER) negative, progesterone receptor (PR) negative, and HER2 negative, which is histologically a poorly differentiated invasive ductal carcinoma. Her disease was staged as T2N1M0 based on imaging findings, including a Positron Emission Tomography/Computed Tomography (PET/CT) scan that showed intense 18F-fluorodeoxyglucose (FDG) uptake in the left breast and axillary nodes but no distant metastases, as can be seen in Figures 1, 2 (yellow arrows).
Axial PET/CT image demonstrating hyper-metabolic lesion in the left inner quadrant of the left breast (Slice 175/263)PET/CT: Positron Emission Tomography/Computed Tomography
Axial PET/CT image demonstrating hyper-metabolic lesion in the left inner quadrant of the left breast (Slice 164/263)PET/CT: Positron Emission Tomography/Computed Tomography
Prior to her presentation to our facility, the patient had undergone genetic testing at another clinic, which revealed a pathogenic RYR1 gene mutation consistent with CCD. Her daughter was also diagnosed with this genetic mutation and that prompted our patient's testing. Thus, her oncologic history was further complicated by this rare congenital neuromuscular disorder. The RYR1 gene mutation not only accounted for her lifelong muscle weakness and motor delays but also conferred a high risk of malignant hyperthermia in response to certain anesthetics. CCD has critical implications for perioperative care and chemotherapy-related myopathy risk. Additionally, she had a history of anemia, drug-induced neuropathy, and iron and folate deficiencies, requiring close hematologic monitoring throughout treatment.
Given the complexity of managing TNBC in a patient with an underlying RYR1 gene mutation and CCD, a multidisciplinary treatment plan was implemented. Table 1 below summarizes the patient’s therapeutic course, including chemotherapy, immunotherapy, surgery, and radiation interventions, along with relevant supportive care.
With confirmed TNBC and axillary lymph node involvement, treatment was initiated using the KEYNOTE-522 protocol, incorporating both chemotherapy and immunotherapy in the neoadjuvant setting. This included pembrolizumab, paclitaxel, and carboplatin, followed by pembrolizumab, cyclophosphamide, and epirubicin. The patient tolerated the regimen with expected side effects, including fatigue, neuropathy, anemia, and gastrointestinal symptoms. These were managed with supportive care, hydration, IV iron, folic acid, and vitamin B12 injections. Due to her severe anemia (Hb as low as 7.7 g/dL; normal 12-16 g/dL), she received transfusions and ongoing iron supplementation. Despite these complications, she demonstrated a significant clinical and radiographic response, and by August 2024, she reported no longer feeling the breast mass.
To proactively manage the risk of muscle-related complications, particularly rhabdomyolysis and immune-mediated myositis, serial measurements of creatine kinase, myoglobin, and aldolase were obtained during therapy. A summary of these values is presented in Table 2 below.
All values remained within normal ranges throughout the course of treatment, with myoglobin going up to 73 once (normal range=25-72), but coming back to normal without any interventions.
She underwent bilateral mastectomy with sentinel node evaluation. The final pathology of the left breast revealed a 2.3 cm invasive ductal carcinoma with negative margins but tumor presence at the posterior inked margin; sentinel nodes were negative. The right breast showed no evidence of malignancy. Moreover, given her underlying susceptibility to malignant hyperthermia, dantrolene was made readily available prior to the administration of anesthetic agents as a precautionary measure. Postoperatively, she received radiation therapy, which she completed in April 2025, and was able to "ring the bell," marking the end of radiation. She has since resumed pembrolizumab maintenance every three weeks, with only two cycles remaining. Her post-treatment imaging, labs, and follow-up evaluations indicate continued remission, and she is scheduled to proceed with breast reconstruction in the coming months. This case emphasizes the importance of multidisciplinary coordination when managing cancer in patients with rare genetic disorders. It also highlights how personalized treatment plans can lead to excellent outcomes even in complex clinical scenarios.
Discussion
Congenital myopathies affect approximately six out of every 100,000 live births, with CCD being one of the most common subtypes [9]. CCD is characterized by the presence of well-demarcated, oval-shaped cores within type 1 muscle fibers, which lack oxidative enzyme activity [9,10]. Clinically, it presents with features typical of congenital myopathy. The condition is associated with mutations in the RYR1 gene located on chromosome 19q13.1 [10].
The RYR1 gene encodes the ryanodine receptor, a calcium release channel within the sarcoplasmic reticulum (SR) of skeletal muscle. This channel regulates cytosolic calcium levels and plays a critical role in muscle excitation-contraction coupling. As seen in CCD, mutations in the RYR1 gene lead to clinical manifestations such as symmetrical mild weakness, hypotonia, delayed motor milestones, and predominant involvement of the proximal, axial, and hip girdle muscles. Facial weakness may also be present. Additionally, musculoskeletal deformities such as hip dislocation, scoliosis, and foot abnormalities are commonly observed [10].
Importantly, RYR1 mutations are also associated with a predisposition to malignant hyperthermia, with gain-of-function mutations found in 50-70% of affected individuals [11]. Malignant hyperthermia is a life-threatening hypermetabolic reaction of skeletal muscle triggered by exposure to certain volatile anesthetics or depolarizing muscle relaxants. It is characterized by uncontrolled calcium release from the SR, resulting in persistent muscle contraction, muscle rigidity, hyperthermia, hypercarbia, and cardiac arrhythmias [12].
The diagnosis of CCD typically involves a combination of physical examination, detailed family history, and muscle biopsy demonstrating central cores. Muscle MRI can reveal characteristic patterns of muscle involvement, especially when histopathology is inconclusive. Advances in genetic testing have allowed for the detection of RYR1 mutations, enabling a noninvasive and definitive diagnosis, and reducing the need for invasive procedures such as muscle biopsies [10].
In patients with CCD who develop breast cancer, management requires careful consideration of the potential side effects of chemotherapy, surgery, immunotherapy, and radiation therapy on underlying muscle pathology. Rhabdomyolysis, although rare, is a potentially fatal complication associated with certain chemotherapeutic agents. Previous reports have documented the development of rhabdomyolysis in patients after receiving chemotherapy [13,14]. Our patient was frequently monitored in order to prevent the development of any such complication. While the exact mechanism remains unclear, it is hypothesized that chemotherapeutic drugs may cause direct muscle membrane injury, leading to the release of intracellular enzymes such as creatine kinase and myoglobin [13]. Clinically, rhabdomyolysis can present with muscle pain, weakness, confusion, and, in severe cases, acute kidney injury. Agents such as paclitaxel, cytarabine, and cyclophosphamide have been implicated [14].
Similarly, immune checkpoint inhibitors, such as pembrolizumab, have been linked to rare cases of autoimmune myositis [15] and rhabdomyolysis [7]. Autoimmune myositis can present with muscle weakness (especially in the proximal muscles), muscle pain, and difficulty swallowing and breathing. Therefore, patients with CCD receiving these therapies require regular clinical assessment and monitoring of serum creatine kinase, myoglobin, and aldolase levels to detect early signs of muscle injury. Additionally, radiation-induced myopathy, although delayed, is another potential complication, often presenting years after therapy with muscle stiffness, weakness, and pain.
Surgical interventions, commonly necessary in breast cancer management, pose significant risks to patients predisposed to malignant hyperthermia. Volatile anesthetics such as halothane and isoflurane and depolarizing muscle relaxants such as succinylcholine are well-established triggers for malignant hyperthermia. The European Malignant Hyperthermia Group recommends the exclusive use of trigger-free anesthesia and ensuring that volatile anesthetic concentrations in the anesthesia workstation are kept at or below 5 parts per million (ppm) to prevent malignant hyperthermia in susceptible individuals [16].
This case highlights the unique challenges encountered when managing oncology patients with pre-existing myopathies. It emphasizes the critical role of early identification, individualized treatment planning, and vigilant monitoring for complications throughout cancer therapy. Through appropriate preventive strategies and close follow-up, the patient described in this report successfully completed her breast cancer treatment without exacerbation of her underlying myopathy, demonstrating the importance of proactive care in improving overall patient outcomes.
Conclusions
This case highlights the complexities of managing breast cancer in a patient with underlying CCD, emphasizing the need for early recognition, multidisciplinary coordination, and careful monitoring. Despite being at high risk, she was able to receive appropriate chemotherapy and the KEYNOTE-522 protocol. Through individualized planning that included anesthetic precautions, regular surveillance of muscle biomarkers, and supportive management during chemotherapy and immunotherapy, the patient completed her treatment without significant myopathic complications. This report illustrates that, with appropriate preventive strategies, patients with rare genetic disorders can achieve successful oncologic outcomes while minimizing treatment-related risks.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Breast Cancer Facts & Stats 5 2025 Team Team N.(2025 April 2 2025 https://www.nationalbreastcancer.org/breast-cancer-facts/
- 2Triple-negative breast cancer: current treatment strategies and factors of negative prognosis J Med Life Baranova A Krasnoselskyi M Starikov V 1531611520223541909510.25122/jml-2021-0108 PMC 8999097 · doi ↗ · pubmed ↗
- 3Triple negative breast cancer 5 2025 Team Team N.(2025 a March 25 2025 https://www.nationalbreastcancer.org/triple-negative-breast-cancer/
- 4Triple negative breast cancer treatment options and limitations: future outlook Pharmaceutics Obidiro O Battogtokh G Akala EO 1796152023 https://doi.org/10.3390/pharmaceutics 150717963751398310.3390/pharmaceutics 15071796 PMC 10384267 · doi ↗ · pubmed ↗
- 5Central core disease: facial weakness differentiating biallelic from monoallelic forms Genes (Basel) Cotta A Souza LS Carvalho E 760132022 https://doi.org/10.3390/genes 130507603562714410.3390/genes 13050760 PMC 9141459 · doi ↗ · pubmed ↗
- 6Chemotherapy-induced myopathy: the dark side of the cachexia sphere Cancers (Basel) Campelj DG Goodman CA Rybalka E 3615132021 https://doi.org/10.3390/cancers 131436153429882910.3390/cancers 13143615 PMC 8304349 · doi ↗ · pubmed ↗
- 7Myopathy leading to rhabdomyolysis as a rare side effect of lenvatinib and pembroluzimab therapy Chest Lord M Healey LA Negin B 011662024
- 8Neoadjuvant immunotherapy and chemotherapy regimens for the treatment of high-risk, early-stage triple-negative breast cancer: a systematic review and network meta-analysis BMC Cancer Cortes J Haiderali A Huang M 792232023 https://doi.org/10.1186/s 12885-023-11293-4 3761262410.1186/s 12885-023-11293-4PMC 10463750 · doi ↗ · pubmed ↗