Percutaneous Transvenous Retrograde Embolization of Adhesion-Related Small Bowel Varices: A Case Report
Ghanem Mohamed, Sondes Bizid, Hatem Ben Abdallah, Mohamed Riadh Bouali

TL;DR
A rare case of small bowel varices was successfully treated with a minimally invasive embolization technique, highlighting the importance of imaging and proper diagnosis.
Contribution
This case report introduces a novel percutaneous retrograde embolization approach for adhesion-related small bowel varices.
Findings
The embolization achieved immediate hemostasis and no recurrence was observed over nine years.
Cross-sectional imaging was critical for diagnosis and planning the treatment approach.
Superficial venous puncture is a minimally invasive and effective access route for transvenous obliteration.
Abstract
Small bowel varices are a distinct subtype of ectopic varices that typically develop following prior abdominal surgery. Diagnostic delays are common because of their deep location within the gastrointestinal tract and the limited awareness among clinicians. Transvenous obliteration is the preferred treatment; however, obtaining a suitable and minimally invasive venous access route remains challenging. We report the case of a 54-year-old woman with advanced-stage primary biliary cholangitis (PBC) and celiac disease who presented with persistent melena requiring multiple transfusions. Endoscopic evaluations failed to identify the bleeding source. Contrast-enhanced computed tomography revealed adhesion-related jejunal varices arising from a mesenteric-iliac shunt. Percutaneous venous access was achieved via the efferent vein coursing within the anterior abdominal wall. Retrograde…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
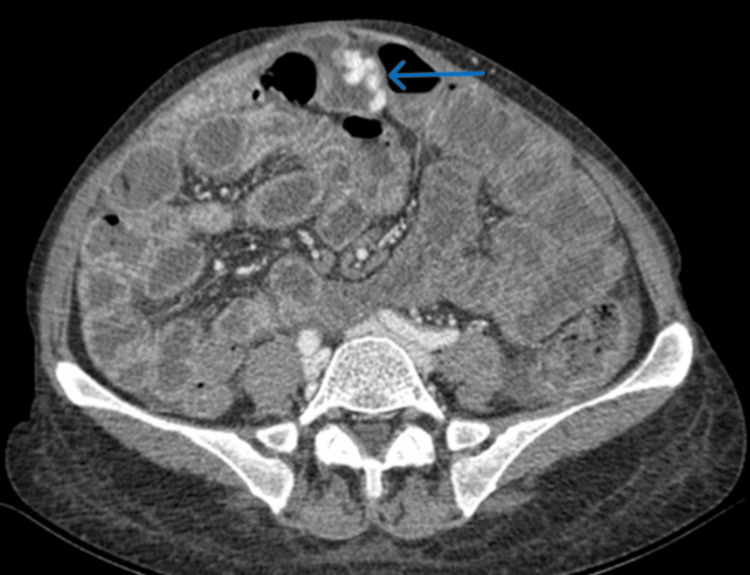 Figure 1
Figure 1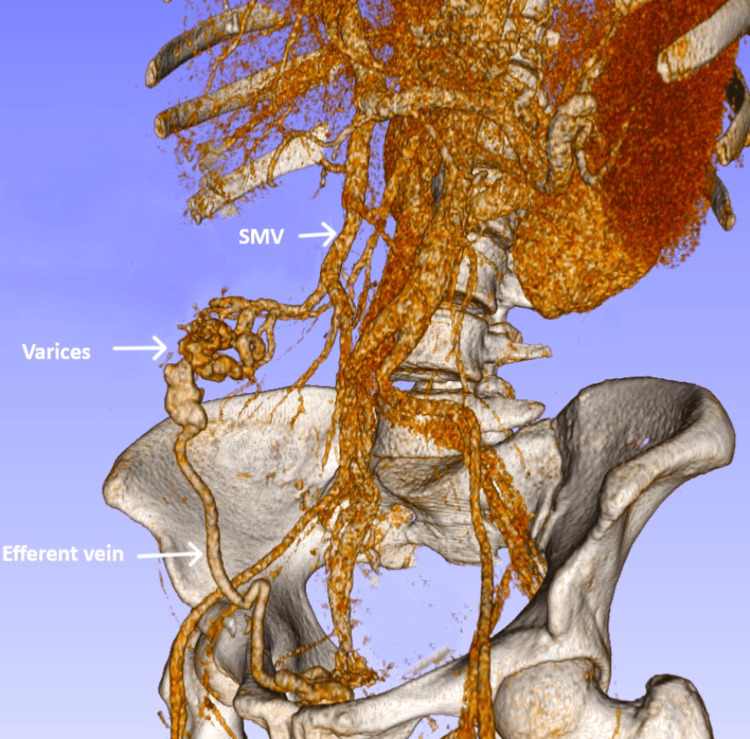 Figure 2
Figure 2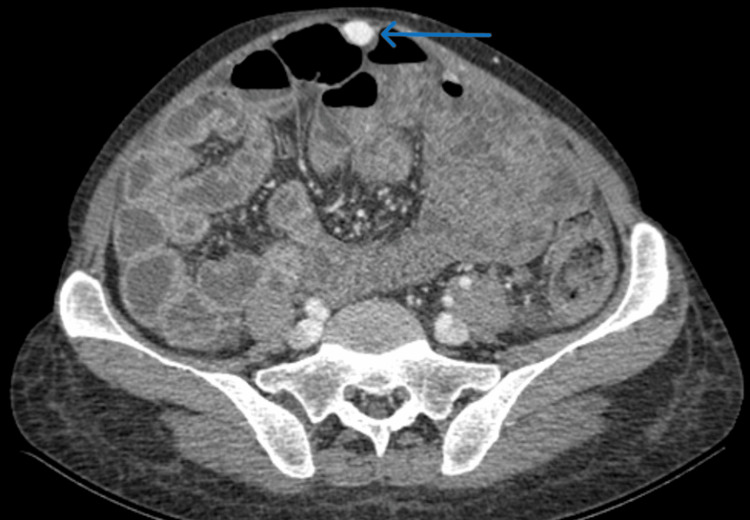 Figure 3
Figure 3 Figure 4
Figure 4| Parameter | Result | Reference Range |
| Hemoglobin | 4.0 g/dL | 13-18 g/dL |
| Platelet count | 132 × 10³/μL | 150-450 × 10³/μL |
| Total bilirubin | 2.51 mg/dL | <1 mg/dL |
| AST | 109 IU/L | 10-60 IU/L |
| ALT | 94 IU/L | 10-42 IU/L |
| ALP | 561 IU/L | 42-121 IU/L |
| GGT | 662 IU/L | 7-64 IU/L |
| Creatinine | 0.54 mg/dL | 0.6-1.2 mg/dL |
| CRP | 5.0 mg/L | <8 mg/L |
| INR | 1.12 | 0.8-1.2 |
| Albumin | 32 g/L | 35-50 g/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Intestinal and Peritoneal Adhesions · Abdominal vascular conditions and treatments
Introduction
Acute variceal bleeding is a severe and life-threatening complication of portal hypertension. Despite advances in pharmacological therapy, endoscopic management, and endovascular interventions such as transjugular intrahepatic portosystemic shunt (TIPS) and transvenous obliteration, six-week mortality remains high at 10%-15% [1,2]. Prognosis depends on the severity of portal hypertension, the stage of liver disease, and the site of the varices [1,2]. While gastroesophageal varices are the most common source of bleeding, varices can also develop outside this region and are classified as ectopic varices [1,2].
Ectopic varices may occur in any part of the gastrointestinal tract, as well as in the gallbladder, bladder, uterus, or vagina [3,4]. They account for approximately 5% of all hemorrhagic events related to portal hypertension, with reported mortality rates as high as 40% [3]. Small bowel varices represent a distinct subtype of ectopic varices, typically arising after abdominal surgery in patients with portal hypertension [3-6]. Diagnostic delays are common due to their deep intraluminal location and limited clinician awareness [3,4]. The management of ectopic varices remains non-standardized, as current evidence is largely limited to case reports and small series [7-10]. Transvenous obliteration is considered the preferred treatment for small bowel varices; however, obtaining suitable and minimally invasive venous access can be challenging [4]. Here, we report a case of adhesion-related small bowel varices successfully treated with transvenous obliteration through an uncommon percutaneous approach.
Case presentation
A 54-year-old woman with advanced-stage primary biliary cholangitis (PBC) and celiac disease was referred for evaluation of persistent melena. Her past surgical history included umbilical hernia repair. She had been hospitalized for two weeks at a local facility, during which she received multiple blood transfusions. The source of bleeding remained undetermined despite upper and lower gastrointestinal endoscopy.
On examination, her blood pressure was 90/58 mmHg and heart rate 90 beats per minute. There was no ascites or evidence of neurological impairment. Laboratory investigations showed severe anemia with a hemoglobin level of 4.0 g/dL and mild cholestasis. Complete laboratory findings are summarized in Table 1.
Repeat esophagogastroduodenoscopy revealed small esophageal varices without signs of recent bleeding. No gastric varices were observed. Colonoscopy demonstrated fresh blood in the lumen but no identifiable bleeding source.
Contrast-enhanced abdominal CT showed a dilated, tortuous vein within the wall of a jejunal loop adjacent to the anterior abdominal wall (Figure 1). A tributary of the superior mesenteric vein served as the feeding vein, while an anterior abdominal wall vein draining into the internal iliac veins acted as the efferent vein. No contrast extravasation was detected. These findings were consistent with bleeding from adhesion-related jejunal varices forming part of a mesenteric-iliac shunt (Figure 2).
Portal-phase abdominal CT showing jejunal varices (blue arrow)
3D reconstruction of the mesenteric-iliac shuntSMV: superior mesenteric vein.Note: This image was created using 3D Slicer v5.8.1 (https://www.slicer.org/).
After blood transfusion and initiation of vasoactive therapy, the superficial component of the shunt running within the anterior abdominal wall (Figure 3) was percutaneously accessed under ultrasound guidance (Figure 4). Retrograde embolization of the varices was then performed using N-butyl-2-cyanoacrylate mixed with ethiodized oil, without the use of balloon occlusion. This procedure achieved immediate bleeding control.
Portal-phase abdominal CT showing the superficial component of the shunt running within the anterior abdominal wall (blue arrow)
Venogram obtained after percutaneous access of the efferent vein
A complete and sustained biochemical response of PBC was achieved following the initiation of ursodeoxycholic acid (UDCA) therapy and adherence to a gluten-free diet. At nine years of follow-up, no hemorrhagic recurrence or additional hepatic events have been observed.
Discussion
Small bowel varices are a form of ectopic varices that develop in patients with portal hypertension, most commonly at sites of previous abdominal surgery. They arise due to postoperative adhesions that cause focal venous constriction and localized areas of portal hypertension [3,4].
The tributaries of the superior mesenteric vein form the afferent pathway, while the efferent pathway typically involves the anterior abdominal wall veins or the retroperitoneal veins of Retzius, which drain either directly into the inferior vena cava (IVC) or via the iliac, renal, or gonadal veins [5,6].
Bleeding from ectopic varices should be considered in any patient with portal hypertension when the bleeding source remains unidentified after upper endoscopy and colonoscopy. A history of previous abdominal surgery should further raise the level of suspicion [3-10].
Contrast-enhanced cross-sectional imaging allows accurate diagnosis, detailed delineation of shunt anatomy, and appropriate selection of the treatment approach and venous access route [4].
Treatment options for ectopic varices include endoscopy, surgery, and endovascular therapy [3]. Unlike duodenal or rectal varices, jejuno-ileal varices cannot be reached with conventional endoscopy, making endovascular therapy the mainstay of treatment [3,4]. Endovascular options include TIPS placement or transvenous obliteration. TIPS placement is preferred in patients with liver decompensation, although it may be insufficient alone because it does not address focal venous constriction and localized portal hypertension [4]. Transvenous obliteration can be performed either retrogradely or anterogradely. In small bowel varices, the retrograde approach is rarely feasible because a single major outflow vein that is readily accessible through systemic venous routes (e.g., the internal jugular or common femoral vein) is uncommon [4]. In contrast, the anterograde approach often represents the only viable option. It involves catheterizing the afferent vein via percutaneous transhepatic or transsplenic access. When a recanalized paraumbilical vein is present, direct puncture of its superficial abdominal wall segment offers a less invasive alternative [4,10]. Whenever anatomically feasible, superficial venous puncture should be considered the first-line approach for transvenous obliteration, as it provides optimal access with reduced morbidity [4,10]. In patients with a TIPS, the anterograde approach can also be performed through the shunt via internal jugular vein access [4]. Retrograde embolization through direct percutaneous puncture of the efferent abdominal wall vein is an uncommon but minimally invasive technique for small bowel variceal obliteration. This approach was used in our case because of the superficial course of the shunt. Saad et al. previously described and supported a similar percutaneous method for managing parastomal varices, which are also superficial adhesion-related mesenteric varices [11]. In our case, a mixture of N-butyl-2-cyanoacrylate and ethiodized oil was used. N-butyl-2-cyanoacrylate polymerizes immediately upon contact with blood, eliminating the need for balloon or vascular plug occlusion to prevent systemic diffusion [2].
Conclusions
Small bowel varices are a distinct subtype of ectopic varices that most often develop after prior abdominal surgery. Diagnostic delays are common due to their deep location within the gastrointestinal tract and limited clinician awareness. Ectopic varices should be considered in any patient with portal hypertension who presents with unexplained gastrointestinal bleeding, particularly following abdominal surgery. Contrast-enhanced cross-sectional imaging is essential for diagnosis and treatment planning. Transvenous obliteration remains the mainstay of therapy, though obtaining suitable venous access can be challenging. When anatomically feasible, superficial venous puncture should be the preferred first-line approach for transvenous obliteration because of its minimally invasive nature.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1AASLD practice guidance on risk stratification and management of portal hypertension and varices in cirrhosis Hepatology Kaplan DE Ripoll C Thiele M Fortune BE Simonetto DA Garcia-Tsao G Bosch J 118012117920243787029810.1097/HEP.0000000000000647 · doi ↗ · pubmed ↗
- 2AASLD practice guidance on the use of TIPS, variceal embolization, and retrograde transvenous obliteration in the management of variceal hemorrhage Hepatology Lee EW Eghtesad B Garcia-Tsao G 2242507920243739048910.1097/HEP.0000000000000530 · doi ↗ · pubmed ↗
- 3Diagnosis and management of ectopic varices in portal hypertension Lancet Gastroenterol Hepatol Tranah TH Nayagam JS Gregory S 1046105682023 https://www.thelancet.com/journals/langas/article/PIIS 2468-1253(23)00209-1/fulltext 3768368710.1016/S 2468-1253(23)00209-1 · doi ↗ · pubmed ↗
- 4Interventional radiology for bleeding ectopic varices: individualized approach based on vascular anatomy Radiographics Kim HC Miyayama S Lee EW Lim DY Chung JW Jae HJ Choi JW 044202410.1148/rg.23014038990775 · doi ↗ · pubmed ↗
- 5A comprehensive review of portosystemic collaterals in cirrhosis: historical aspects, anatomy, and classifications Int J Hepatol Philips CA Arora A Shetty R Kasana V 6170243201620162807415910.1155/2016/6170243 PMC 5198179 · doi ↗ · pubmed ↗
- 6Collateral pathways in portal hypertension J Clin Exp Hepatol Sharma M Rameshbabu CS 338352220122575545610.1016/j.jceh.2012.08.001PMC 3940321 · doi ↗ · pubmed ↗
- 7Recurrent hematochezia due to ileal varices: a case report Cureus Ho S Azizian J Tey K 017202510.7759/cureus.80479 PMC 1199071240225482 · doi ↗ · pubmed ↗
- 8Small bowel variceal bleeding in patients with liver cirrhosis treated with transarterial embolization: case series Korean J Gastroenterol Seo B Lee JH Jang EJ 3043098220233813000110.4166/kjg.2023.116PMC 12285437 · doi ↗ · pubmed ↗