Infants′ Sunlight Exposure Practice and Associated Factors Among Mothers in Northwest Ethiopia: A Community‐Based Cross‐Sectional Study Community‐Based Cross‐Sectional Study
Tesfaye Shumet Mekonnen, Eneyew Talie Fenta, Anley Shiferaw Enawgaw, Fassikaw Kebede Bizuneh, Amare Mebrat Delie

TL;DR
This study in Ethiopia finds that only 38% of mothers expose their infants to adequate sunlight, with education and postnatal care being key factors.
Contribution
The study identifies specific sociodemographic factors influencing infant sunlight exposure practices in a community setting in Ethiopia.
Findings
Only 38% of mothers reported adequate infant sunlight exposure.
Mothers aged 25–34 and those with higher education were more likely to practice good sunlight exposure.
Lack of postnatal care was linked to reduced likelihood of adequate sunlight exposure.
Abstract
Sunlight is crucial for infant health, as it contributes to bone development, immune function, and overall well‐being. However, Maternal sunlight exposure practices are influenced by various sociodemographic and healthcare‐related factors, including maternal age, education level, and access to postnatal care. This study aimed to assess sunlight exposure practices and associated factors among mothers in Gindewoin town. A community‐based cross‐sectional study included 397 randomly selected mothers with infants. Data were collected through structured interviews, entered into EpiData version 4.2, and analyzed using SPSS version 26. Binary logistic regression was performed to identify determinants of good sunlight exposure practices. Only 38% of mothers reported practicing adequate sunlight exposure for their infants. Mothers aged 25–29 years (AOR = 3.01) and 30–34 years (AOR = 4.11) were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
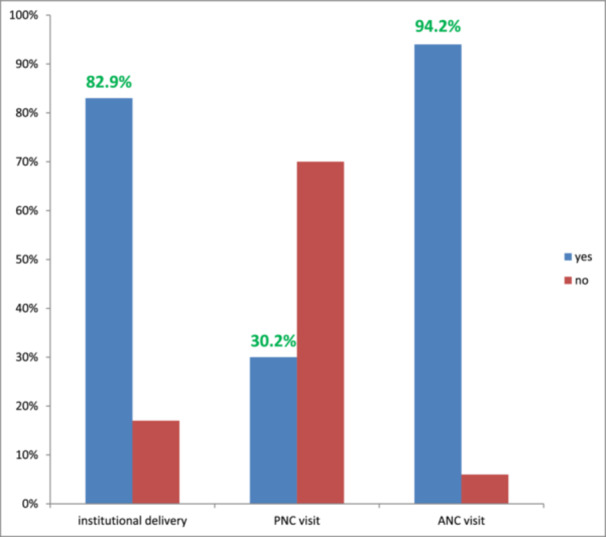 Figure 1
Figure 1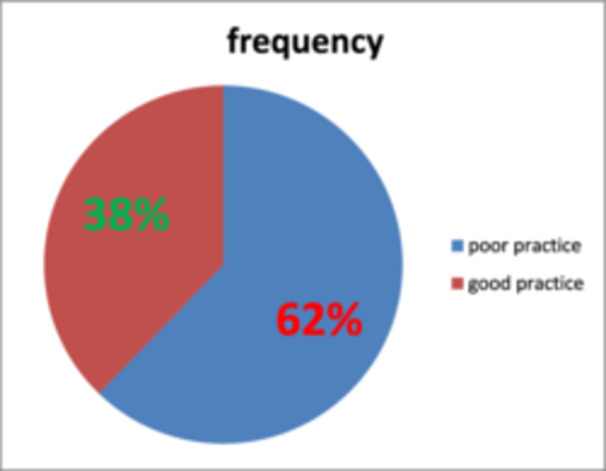 Figure 2
Figure 2| Demographic variables | Category | Frequency | Percentage (%) |
|---|---|---|---|
| Maternal age | Less than 20 years | 58 | 14.61 |
| 20–24 years | 92 | 23.17 | |
| 25–29 years | 109 | 27.5 | |
| 30–34 years | 64 | 16.1 | |
| 35 and older age | 74 | 18.6 | |
| Infant age | One month and younger | 32 | 8.1 |
| 2–5 months of age | 210 | 52.9 | |
| 6 month and older | 155 | 39.0 | |
| Religion | Orthodox | 206 | 51.9 |
| Muslim | 163 | 41.1 | |
| Protestant | 28 | 7.1 | |
| Marital status | Unmarried | 34 | 8.6 |
| Married | 308 | 77.5 | |
| Divorced | 33 | 8.3 | |
| Widowed | 22 | 5.5 | |
| Maternal education status | Up to grade 12 | 249 | 62.72 |
| College diploma and above | 148 | 37.28 | |
| Fathers education ( | Up to grade 12 | 145 | 47.1 |
| College diploma and above | 163 | 52.9 | |
| Family income | Less than 2500 birr | 72 | 18.1 |
| 2500–4000 birr | 87 | 21.9 | |
| 4001–7500 birr | 86 | 21.7 | |
| More than 7500 birr | 152 | 38.3 | |
| Occupation of mother | Student | 20 | 5.0 |
| House wife | 138 | 34.8 | |
| Government employee | 60 | 15.1 | |
| Private employee | 34 | 8.6 | |
| Daily laborer | 48 | 12.1 | |
| Merchant | 97 | 24.4 | |
| Number of children | 1–3 | 297 | 74.81 |
| 4 and more | 100 | 27.19 |
| Characteristics | Category | Frequency | Percentage |
|---|---|---|---|
| Intentionally expose to sunlight | Yes | 270 | 68.3 |
| No | 127 | 31.7 | |
| Age to start sunning | 0–15 days | 72 | 26.6 |
| 15–30 days | 54 | 20.0 | |
| 30–45 days | 32 | 11.8 | |
| After 45 days | 112 | 41.5 | |
| Condition of clothing | Only diaper | 48 | 17.8 |
| Partially covered | 132 | 48.9 | |
| Completely covered | 90 | 33.3 | |
| Application of lubricants | Yes | 146 | 54.1 |
| No | 124 | 45.9 | |
| Frequency of exposure | Daily | 76 | 28.2 |
| Sometimes | 194 | 71.8 | |
| Duration of exposure | Less than 10 min | 6 | 2.2 |
| 10–15 min | 92 | 34.1 | |
| 16–30 min | 56 | 20.7 | |
| More than 30 min | 116 | 43.0 | |
| Time of exposure | Morning 8–10 AM | 192 | 71.1 |
| After noon | 78 | 28.9 |
| Variables | Category | Good practice ( | Poor practice ( | COR with 95% CI | AOR with 95% CI |
| |
|---|---|---|---|---|---|---|---|
| PNC follow‐up | Yes | 68 | 53 | Reference | Reference | ||
| No | 81 | 195 | 0.32(0.20–0.49) | 0.26(0.15–0.46) |
| ||
| Number of ANC follow‐ups | Only one | 10 | 12 | Reference | Reference | ||
| Two times | 40 | 72 | 3.77(0.80–17.65) | 5.51(0.95–31.85) | 0.06 | ||
| Three times | 58 | 87 | 3.82(0.82–17.70) | 4.68(0.79–27.44) | 0.09 | ||
| Four times | 44 | 51 | 5.29(1.12–24.93) | 5.92(0.99–35.15) | 0.051 | ||
| Place of delivery | Health institution | 129 | 199 | Reference | Reference | ||
| Home delivery | 21 | 48 | 0.64(0.36–1.13) | 1.57(0.75–3.29) | 0.23 | ||
| Maternal education | Up to grade 12 | 71 | 178 | Reference | Reference | ||
| Diploma and above | 79 | 69 | 2.91(1.90–4.45) | 3.28(1.88–5.73) |
| ||
| Maternal age | < 20years | 14 | 44 | Reference | Reference | ||
| 20–24 years | 31 | 61 | 1.52(0.72–3.19) | 0.85(0.35–2.01) | 0.71 | ||
| 25–29 years | 54 | 55 | 3.14(1.54–6.39) | 2.86(1.28–6.42) |
| ||
| 30–34 years | 29 | 35 | 2.60(1.19–5.66) | 4.15(1.58–10.90) |
| ||
| > 35 years | 22 | 52 | 1.32(0.60–2.90) | 2.19(0.75–6.44) | 0.15 | ||
| Marital status | Unmarried | 12 | 22 | Reference | Reference | ||
| Married | 123 | 185 | 2.31(0.91–5.86) | 0.98(0.34–2.83) | 0.98 | ||
| Divorced | 14 | 19 | 2.70(0.86–8.42) | 1.73(0.47–6.33) | 0.41 | ||
| Widowed | 12 | 10 | 1.83(0.40–8.23) | 0.80(0.15–4.35) | 0.80 | ||
| Religion | Muslim | 66 | 95 | Reference | Reference | ||
| Orthodox | 75 | 131 | 0.83(0.54–1.27) | 0.92(0.55–1.52) | 0.74 | ||
| Protestant | 10 | 20 | 0.58(0.24–1.39) | 0.48(0.17–1.35) | 0.17 | ||
| Family size | 1–3 | 118 | 179 | Reference | Reference | ||
| 4 and more | 32 | 68 | 0.72(0.44–1.16) | 0.39(0.17–0.89) |
| ||
- —The authors received no specific funding for this work.
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreastfeeding Practices and Influences · Skin Protection and Aging · Neonatal Health and Biochemistry
Introduction
1
Infancy is a critical period marked by rapid growth and development, making the role of environmental influences, such as sunlight exposure, particularly crucial [1]. Sunlight serves as a primary natural and cost effective means of obtaining vitamin D [2, 3]. Vitamin D is a vital nutrient essential for bone health, immune system function, and overall well‐being [4, 5, 6, 7]. The practice of ensuring adequate sunlight exposure for infants is, however, contingent upon a myriad of factors deeply embedded in cultural and socioeconomic contexts [8].
According to a World Health Organization (WHO) report, the prevalence of vitamin D deficiency (VDD) in children, specifically infants, ranges from 30% to 80%. It is an important public health problem in both developed and underdeveloped countries and will cause many health related problems including rickets [4, 9]. Infants, in particular, rely heavily on external sources of vitamin D, as their skin is more sensitive and they may not consume enough through diet alone [10, 11]. The duration, timing, and quality of sunlight exposure during infancy can significantly impact a child′s health outcomes [12].
Mothers, as primary caregivers, play a central role in determining infants′ exposure to sunlight [13]. Maternal knowledge, attitudes, and practices regarding sunlight exposure are crucial in shaping the health outcomes of their infants [14]. Understanding the factors that influence mothers′ decisions related to sunlight exposure for their infants is vital for developing targeted interventions and educational programs [15].
Ethiopia′s multicultural society, comprising various ethnic groups and communities, adds complexity to the study of infants′ sunlight exposure practices [16]. Practices related to clothing, outdoor activities, and beliefs about the effects of sunlight on health may differ significantly among these groups, influencing the duration and quality of sunlight exposure for infants [17].
Additionally, access to healthcare services and information about the importance of sunlight exposure can vary across different regions of Ethiopia [16]. Factors such as maternal education, awareness of nutritional requirements, and engagement with healthcare providers can all impact the decisions mothers make regarding infants′ sunlight exposure [18, 19].
Based on the previous studies conducted in Ethiopia, the magnitude of good practice of sunlight exposure ranges from 44% to 58% in various regions [14, 18, 20, 21, 22, 23]. For instance, a study in Dessie Town reported that 41% of mothers exposed their infants to sunlight adequately, whereas in Yirgalem, the proportion was higher, around 54.3% [20, 23]. This variability highlights the presence of regional, cultural, and healthcare disparities affecting maternal practices. According to studies, different factors like maternal and husband education, mother occupation, family size, poor living conditions and unfavorable weather conditions were determining factors of infants′ sunlight exposure [24]. Additionally, fear of cold, fear of evil eyes, and fear of witchcraft were reported as a cause of inadequate sunlight exposure in some studies [14].
Despite the known benefits of sunlight exposure, there is a growing concern about inadequate exposure among infants in various communities, including Ethiopia [10, 16]. This issue is multifaceted and influenced by a range of factors [25]. This includes cultural beliefs and practices, urbanization, lifestyle changes, and prevailing health recommendations [26, 27]. Cultural norms related to clothing practices, perceptions of sunlight as a health risk, and urban living conditions contribute to the variability in infants′ sunlight exposure practices [28].
In light of these considerations, this study was designed as a community‐based cross‐sectional investigation to assess the level of infant sunlight exposure practices and to identify the sociodemographic and healthcare‐related factors influencing these practices among mothers in northwestern Ethiopia. The cross‐sectional design was selected to capture a snapshot of current maternal behaviors and associated factors across a representative sample. This approach allows for quantifying the magnitude of good sunlight exposure practices and exploring potential determinants in the population. Ultimately, the findings aim to inform targeted public health strategies that promote optimal infant sunlight exposure and improve maternal awareness in the local context.
Methods
2
Study Area and Period
2.1
The study was conducted from June 30, 2024, to July 30/2024 in Gindewoin town mothers, which is located in Goncha district, northwestern Ethiopia. Gindewoin town is located at 335 km far from Addis Ababa, the capital city of Ethiopia and at 150 km far from Bahir Dar, the city of Amhara regional state [29]. The town comprises 7) kebeles (smallest administrative unit in Ethiopia).
Study Design
2.2
Community based cross sectional study design was employed.
Source Population
2.3
The source population for this study consisted of all mothers with infants below the age of 12 months residing in Gindewoin town. The study included mothers with infants under the age of 12 months who were both living in Gindewoin town and available during the data collection period. This inclusion criterion was implemented to ensure that the sample represented the target population of interest—mothers with young infants—and those who were accessible and willing to participate in the study during the data collection phase.
Eligibility
2.4
The study included mothers with infants less than 12 months old who were both mentally and physically capable of providing responses. Exclusion criteria involved mothers who were not regular residents, defined as those living in the town for less than 6 months. These criteria aimed to ensure that the study focused on mothers with a stable and consistent presence in the town, while also selecting participants whose infants were within a specific age range to align with the study objectives.
Sample Size
2.5
The sample size was determined using the single population proportion formula, assuming a proportion of poor sunlight exposure practice at 44% (p = 0.44). This proportion is derived from a previous cross‐sectional study conducted in Dejen district [30]. The calculation was performed with a 95% confidence level (Z a/2 = 1.96) and an estimated margin of error of 5%. Taking into account a 5% nonresponse rate, the final total sample size required for the study is determined to be 397 mothers.
Sampling Procedure
2.6
The research utilized a systematic random sampling approach for participant selection. Mothers who had given birth within the past year were selected from health extension workers associated with each health post. Out of 1327 mothers with infants during the study period, 397 participants were chosen. The initial respondent was selected through a lottery, and thereafter, every third mother (with a constant interval of k = 3) from their respective households was interviewed systematically at regular intervals.
Variables and Their Measurement
2.7
The outcome variable was the mother′s practice of infant sunlight exposure, assessed using seven structured questions adapted from validated tools in previous studies. Each question was scored as 1 for good practice and 0 for poor practice, resulting in a total possible score ranging from 0 to 7. Mothers who scored equal to or above the sample mean were categorized as having good sunlight exposure practices, while those who scored below the mean were categorized as having poor practices. The questions assessed whether the mother exposed her infant to sunlight, the age at which sunlight exposure began (with earlier initiation, particularly before 6 months, considered favorable), the duration of each exposure session (with at least 15 min regarded as good practice), and the frequency of exposure (with daily exposure being preferred). The questionnaire also evaluated the time of day when exposure occurred, with morning hours between 8:00 and 10:00 AM considered optimal for vitamin D synthesis. Additionally, mothers were asked about the body parts exposed during sunning, where exposing the arms and legs or more was considered beneficial. Lastly, the use of lubricants such as butter or oils before sun exposure was assessed, with non‐use being considered a better practice due to potential interference with UVB absorption The socio‐demographic characteristics of respondents (age, religion, marital status, occupation, family income, educational status, family size), the source of information about sunlight exposure, and pregnancy and delivery‐related characteristics of mothers were assessed as independent variables in the study.
Data Collecting Tools and Procedures
2.8
A structured interviewer‐administered questionnaire was used for data collection. The questionnaire was developed based on an extensive review of previous studies and related literature on infant sunlight exposure practices in similar settings [13, 17, 21, 23, 31]. The tool was initially developed in English, translated into the local language (Amharic), and then back‐translated into English to ensure consistency. The questionnaire encompassed socio‐demographic, personal, environmental, and other pertinent variables. Trained Bachelor of Science (BSc) Nurses, along with supervision by one Master of Science (MSc) nurse, conducted face‐to‐face interviews with mothers and infants to collect the data. A day of training was provided to the data collectors, focusing on the study′s objectives, questionnaire content, and issues related to respondent confidentiality and rights. To prevent information contamination, a 5% pretest from the total sample size was conducted in neighboring town, located 27 km away from Gindewoin town.
Method of Data Analysis
3
Following data collection, data entry was performed using EpiData version 3.1, and the data set was subsequently exported to the Statistical Package for the Social Sciences (SPSS) version 26 for analysis. Descriptive statistics were used to summarize socio‐demographic variables. Associations between independent and dependent variables were examined using binary logistic regression. In the bivariable analysis, crude odds ratios (COR) with 95% confidence intervals (CI) were calculated to identify candidate variables with a p‐value ≤ 0.25, which were then entered into the multivariable logistic regression model. Adjusted odds ratios (AOR) with 95% CI were calculated to control for potential confounders. Variables with a p‐value < 0.05 in the multivariable analysis were considered statistically significant factors influencing mothers′ practice of infant sunlight exposure.
Result
4
Socio‐Demographic Characteristics
4.1
A total of 397 mothers participated in the study, yielding a response rate of 100%. The mean age of the mothers was 27.4 ± 7 years, ranging from 15 to 53 years. More than half of the infants were younger than 4 months, with a mean age of 5 ± 3 months.
Regarding religion, more than half of the participants were Orthodox Christians. A majority (307/397, 77.3%) of the mothers were married. About 16.4% (65/397) of respondents had no formal education, while 37.3% (148/397) had attained a diploma or higher educational status. Most mothers were housewives (139/397, 35%) and merchants (59/397, 14.9%). The average monthly income was 6300 ± 3900 Ethiopian birr, with a range of 800 to 25,000 birr (Table 1).
Pregnancy‐Related Variables
4.2
Most respondents (327/397, 82.4%) gave birth at a health facility, with 153 mothers delivering at hospitals. Among all respondents, 374 (94.2%) had at least one Antenatal care (ANC) visit. Of those, 96/374 (25.7%) completed the recommended four ANC visits. Only 120/397 (30.2%) mothers reported postnatal care (PNC) follow‐up, with 62/120 (51.7%) having a single Postnatal care (PNC) visit (shown in Figure 1).
Distribution of pregnancy‐related characteristics among study participants in Gindewoin town, northwest Ethiopia, 2024 (n = 397). The bar chart displays the proportion of respondents who received the service (blue) and those who did not (red) for each pregnancy‐related characteristic assessed. Specifically, institutional delivery (Yes = 82.9%, 95% CI: 79.2%–86.6%), postnatal care (PNC) visit (Yes = 30.2%, 95% CI: 25.7%–34.7%), and antenatal care (ANC) visit (Yes = 94.2%, 95% CI: 91.5%–96.2%) are shown.
Mothers′ Practice of Sunlight Exposure
4.3
Among the participants, 272/397 (68.5%) mothers reported that they intentionally exposed their infants to sunlight. Of these, 72/272 (26.5%) began sunlight exposure within the first 15 days after birth, and 54/272 (19.9%) started within the first 30 days. The majority (192/272, 70.6%) exposed their infants between 8:00 AM and 10:00 AM. Regarding clothing during exposure, 48/272 (17.6%) exposed infants wore only a diaper, while 132/272 (48.5%) were partially covered. 76/272 (27.9%) exposed their infants daily, and 92/272 (33.8%) did so for 10–15 min per session. Additionally, 146/272 (53.7%) applied lubricants to their infants during exposure (see Table 2). Based on the operational criteria, the overall magnitude of good sunlight exposure practice was 38.0% (151/397; 95% CI: 33.0%–42.5%), as determined by responses to seven practice‐related questions (as shown in Figure 2).
Overall practice of infants′ sunlight exposure among mothers in Gindewoin town, northwest Ethiopia, 2024 (n = 397). The pie chart shows the proportion of mothers with good (red) and poor (blue) sunlight exposure practices for their infants. Good practice was assessed using seven practice‐related questions. Among the participants, 38% demonstrated good practice, while 62% had poor practice. Percentages and sample sizes are displayed for each category.
Factors Affecting the Practice of Sunlight Exposure
4.4
Fifteen variables were initially assessed for their association with mothers′ practice using bivariate logistic regression. Variables with p < 0.25 were entered into a multivariable logistic regression model. These included maternal age, marital status, religion, maternal education, place of delivery, family size, number of ANC visits, and PNC follow‐up.
In the final multivariable logistic regression model, four variables remained significantly associated with good sunlight exposure practice (p < 0.05). Compared to mothers aged less than 20 years (reference category), those aged 25–29 years were 2.86 times more likely to practice good sunlight exposure (AOR = 2.86; 95% CI: 1.28–6.42; p = 0.01), and those aged 30–34 years were 4.15 times more likely (AOR = 4.15; 95% CI: 1.58–10.90; p = 0.004). Mothers with a diploma or higher educational level had significantly better practice compared to those with no formal education (reference category), with an AOR of 3.28 (95% CI: 1.88–5.73; p < 0.001). Additionally, mothers without postnatal follow‐up were 74% less likely to practice good sunlight exposure than those with postnatal care (AOR = 0.26; 95% CI: 0.15–0.46; p < 0.001) (Table 3).
Discussion
5
This study aimed to estimate the prevalence of poor sunlight exposure practices and identify associated factors among mothers in Motta city administration, northwest Ethiopia, in 2023. The study revealed that 38% of mothers exhibited good practices of sunlight exposure, a percentage lower than those reported in previous studies conducted in Yirgalem (54.5%), Debre Birhan town (65.7%), Dessie town (41%), Farta district (54.3%), and Wolkitie University specialized hospital (67.3%) [17, 20, 22, 23, 31]. The higher proportion of poor practice in the current study may be attributed to differences in the study population and timing. Moreover, some of the aforementioned studies were institutional, potentially leading to an overestimation of good practice levels, as mothers with good healthcare‐seeking behavior may also exhibit relatively better sunlight exposure practices. However, the current findings were higher than those reported in Aleta Wondo [14], where only 32% of mothers demonstrated good sunlight exposure practices. This discrepancy could be attributed to sociocultural variations between populations.
In this present investigation, 68.3% of the participants deliberately exposed their infants to sunlight. This percentage was found to be less than the rates reported in previous research conducted in Debre Markos (93%), Debre Birhan (99%), and the study undertaken at Wolkitie University Hospital (73.6%) [17, 31, 32]. The variation in these figures may be attributed to sociocultural diversity and disparities in the utilization of health information among the different study populations.
In this study, 26.6% of mothers, among all those who intentionally exposed their infants to sunlight, initiated the exposure at the age of 15‐20 days after birth. This percentage was slightly higher than the findings in the study conducted in Debre Markos [32], where only 23.4%, and in Farta district [22], where 15.7% of mothers began sunlight exposure at this stage of the baby′s life. However, this result was lower than the findings in the studies conducted in Dejen (52%) and Debre Birhan (85%), where a higher percentage of mothers started exposing their infants to sunlight within 15‐20 days after birth [21, 31]. The variation may be attributed to differences in the health information provided to these populations regarding the appropriate age to commence sunlight exposure.
Among the study participants who intentionally exposed their infants to sunlight, only 28.2% did so daily in this study. This figure was lower compared to findings from Debre Markos (57.9%) and Debre Birhan town (60%) [31, 32]. Additionally, 71.1% of mothers in the current study exposed their infants to sunlight in the morning before 10 AM. This percentage was slightly less than the study conducted in Farta [22], where 73% of mothers exposed their infants during this time. Exposure to sunlight during the morning hours, particularly between 8:00 and 10:00 AM, is crucial for adequate vitamin D synthesis because the Ultraviolet B (UVB) radiation, responsible for triggering vitamin D production in the skin, is present in sufficient quantities during this period. Studies indicate that UVB rays in this time window play a key role in promoting bone health and immune function in infants by facilitating optimal vitamin D synthesis [1, 2]. Furthermore, 54.1% of mothers applied lubricants to their babies while sunning, a proportion higher than the study conducted in Debre Markos [32], where only 43% of respondents applied lubricants during sunlight exposure.
The study revealed that 34.1% of mothers exposed their infants to sunlight for 10‐15 min, and only 17.8% exposed their infants with just a diaper. These figures were notably lower compared to previous studies conducted in different areas [13, 20]. The lower findings in this study could be attributed to poor health information utilization in the study area, and it′s possible that the information regarding the duration of sunning may not be consistent across different regions.
In the current study, the age of the mother was found to be significantly associated with good practices of sunlight exposure for infants. Study participants aged 25–29 years and 30–34 years were three times and four times more likely, respectively, to exhibit good practices in infants′ sunlight exposure compared to younger mothers aged 20 years or younger. This finding is consistent with studies conducted in Wolkitie University Specialized Hospital, Dejen, and Debre Markos [17, 32]. All of these studies indicated that younger mothers were less likely to have good practices in infants′ sunlight exposure compared to older mothers. This observation may be explained by the notion that with increasing maternal age, there is a higher level of awareness regarding sunlight exposure and its importance. Additionally, older mothers may be more prepared for appropriate childbearing, as pregnancies for adolescent mothers may not be planned, potentially affecting their awareness and practices.
In the present study, having a history of postnatal care (PNC) follow‐up was found to have a statistically significant association with good practices in infants′ sunlight exposure. Mothers without a PNC visit were 74% less likely to exhibit good practices in sunlight exposure compared to those with a PNC history. This difference may be attributed to the likelihood that mothers with a PNC history received advice and information about the potential benefits of sunlight exposure for infants.
While institutional delivery was associated with good practices in sunlight exposure in a study conducted in Dejen [21], it did not show significant association in the current study′s multivariable analysis. However, both PNC and institutional delivery could be linked to acquiring proper information and awareness about good practices in sunlight exposure.
The study′s results suggest that mothers with a larger family size were over 60% less likely to adopt good practices in sunlight exposure for their infants compared to mothers with smaller families. This finding is consistent with similar studies conducted in Debre Markos, Mettu, and Debre Birhan town [18, 31, 32]. This suggests that as the size of the family increases, the likelihood of mothers implementing appropriate care practices for their infants, such as sunlight exposure, decreases. This trend may be attributed to the added complexity and increased burden on mothers in larger families, making it more challenging for them to prioritize and maintain optimal care practices for their infants.
The educational level of mothers was found to be significantly associated with good practices in infants′ sunlight exposure. Respondents with a diploma and above level of education were more than three times more likely to exhibit good practices in infant sunlight exposure compared to those with lower levels of education. This association is supported by studies conducted in Debre Markos and Dejen [21, 32]. The rationale behind this finding may be that educated mothers are more informed about the benefits of sunlight exposure and possess a better understanding of the appropriate ways to expose their infants to sunlight. Education appears to play a crucial role in enhancing mothers′ knowledge and practices related to infant care, specifically in the context of sunlight exposure.
Limitation
5.1
This study has some limitations. First, the cross‐sectional design limits the ability to establish causal relationships. Second, the data collection was conducted during a specific season, which may affect the generalizability of the findings, as sunlight exposure practices can vary by season. Future studies should consider longitudinal designs that encompass multiple seasons to better understand seasonal variations in infant sunlight exposure practices.
Conclusion
6
The level of good practice in infants′ sunlight exposure was found to be very low in the study area, with two‐thirds of the study participants not appropriately exposing their infants to sunlight. Younger maternal age, larger family size, poor maternal education, and lack of postnatal follow‐up were identified as statistically significant factors affecting mothers′ good practices in sunlight exposure. Strategic interventions should be implemented to minimize early‐age pregnancies, expand family planning initiatives, increase utilization of postnatal care services, and improve access to women′s education. Health education on the importance and correct timing of infant sunlight exposure should be integrated into postnatal care services, with particular emphasis on reaching younger and less‐educated mothers. Improving maternal knowledge through community‐based education and counseling can help ensure that caregivers understand when and how to safely expose their infants to sunlight, particularly during the early morning hours when ultraviolet B (UVB) rays are effective for vitamin D synthesis but less harmful to the skin.
Author Contributions
Tesfaye Shumet Mekonnen: conceptualization, data curation, formal analysis, funding acquisition, methodology, investigation, project administration, resources, software, writing – original draft, and writing – review and editing. Eniyew Talie Fenta: methodology, project administration, resources, software, and writing – review and editing. Anley Shiferaw Enawgaw: methodology, project administration, visualization, supervision, resources, software, and writing – review and editing. Fasikaw Kebede Bizuneh: methodology, investigation, project administration, validation, resources, supervision, software, and writing – review and editing. Amare Mebrat Delie: conceptualization, data curation, formal analysis, funding acquisition, methodology, investigation, project administration, resources, software, writing—original draft, and writing – review and editing. All authors have read and approved the final version of the manuscript. Tesfaye Shumet Mekonnen had full access to all of the data in this study and takes complete responsibility for the integrity of the data and the accuracy of the data analysis.
Ethics Statement
The study was conducted following ethical guidelines, including the Declaration of Helsinki. The research procedures and objectives were thoroughly reviewed by the institutional review board of Woldia University College of Health Sciences. Ethical approval was granted on June 25, 2024, with reference number RCS, TT & UIL; 0025/2016. The study was conducted while the corresponding author was affiliated with Woldia University, which granted ethical approval for this study. The current affiliation with Debre Markos University reflects a subsequent institutional transfer. Following approval, an official letter was submitted to both the town health office and the administrative body. Informed consent was secured from every study participant, accompanied by a clear explanation of the study′s purpose and assurance of confidentiality. Participants were informed of their full right to choose not to partake in the study or to discontinue participation at any point during the interview.
Conflicts of Interest
The authors declare no conflicts of interest.
Transparency Statement
The lead author Tesfaye Shumet Mekonnen affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A. Jindal , A. Gupta , K. Vinay , and A. Bishnoi , “Sun Exposure In Children: Balancing the Benefits and Harms,” Indian Dermatology Online Journal 11, no. 1 (2020): 94–98.32055519 10.4103/idoj.IDOJ_206_19PMC 7001416 · doi ↗ · pubmed ↗
- 2N. M. M. Mansibang , M. G. Y. Yu , C. A. Jimeno , and F. L. Lantion‐Ang , “Association of Sunlight Exposure With 25‐hydroxyvitamin D Levels Among Working Urban Adult Filipinos,” Osteoporosis and Sarcopenia 6, no. 3 (2020): 133–138.33102807 10.1016/j.afos.2020.08.006PMC 7573503 · doi ↗ · pubmed ↗
- 3A. Y. Kurihayashi , R. A. Augusto , F. M. D. Escaldelai , and L. A. Martini , “Estado Nutricional De Vitaminas A E D Em Crianças Participantes De Programa De Suplementação Alimentar,” Cadernos de Saúde Pública 31, no. 3 (2015): 531–542.25859720 10.1590/0102-311x 00082814 · doi ↗ · pubmed ↗
- 4S. Agarwal , O. Kovilam , and D. K. Agrawal , “Vitamin D and Its Impact on Maternal‐Fetal Outcomes in Pregnancy: A Critical Review,” Critical Reviews in Food Science and Nutrition 58, no. 5 (2018): 755–769.27558700 10.1080/10408398.2016.1220915 PMC 6056893 · doi ↗ · pubmed ↗
- 5A. Asyary and M. Veruswati , “Sunlight Exposure Increased Covid‐19 Recovery Rates: A Study in the Central Pandemic Area of Indonesia,” Science of the Total Environment 729 (2020): 139016.32361458 10.1016/j.scitotenv.2020.139016 PMC 7184988 · doi ↗ · pubmed ↗
- 6H. B. Kim and J. H. Kim , “Sunlight Exposure in Association With Risk of Lymphoid Malignancy: A Meta‐Analysis of Observational Studies,” Canc Er Causes & Control: CCC 32, no. 5 (2021): 441–457.33606147 10.1007/s 10552-021-01404-6 · doi ↗ · pubmed ↗
- 7S. T. Kent , M. Cushman , G. Howard , et al., “Sunlight Exposure and Cardiovascular Risk Factors in the REGARDS Study: A Cross‐Sectional Split‐Sample Analysis,” BMC Neurology 14 (2014): 133.24946776 10.1186/1471-2377-14-133PMC 4075775 · doi ↗ · pubmed ↗
- 8M. G. Yu , N. Castillo‐Carandang , M. E. G. Sison , et al., “Attitudes, Behaviors and Beliefs of Urban Adult Filipinos on Sunlight Exposure: A Qualitative Study,” Journal of the ASEAN Federation of Endocrine Societies 33, no. 1 (2018): 37–43.33442109 10.15605/jafes.033.01.06PMC 7784093 · doi ↗ · pubmed ↗