Updated systematic review of current randomised controlled trials in chronic subdural haematoma
R. Fakhry, C. Yesildal, J. Bartek, J. Duerinck, T. S. R. Jensen, J. Soleman, C. Iorio-Morin, C. M. F. Dirven, R. Dammers, E. Edlmann, D. C. Holl

TL;DR
This paper updates a review of recent clinical trials for chronic subdural haematoma, showing a shift in research focus and a significant increase in ongoing studies.
Contribution
The study provides an updated analysis of RCTs in CSDH, highlighting changes in research trends and interventions since 2019.
Findings
The number of ongoing RCTs in CSDH has increased from 26 in 2019 to 54 in 2025.
Middle meningeal artery embolisation is now the most studied intervention, with active trials rising from 2 to 21.
Research on corticosteroids has decreased, while studies on tranexamic acid and other drugs have increased.
Abstract
Chronic subdural haematoma (CSDH) is a common neurosurgical condition with an increasing incidence due to an aging population. Given the expanding research landscape, assessing the state of recent trials is essential. This systematic review updates a previous review, which included randomised controlled trials (RCTs) up to 2019, by summarizing recently published and ongoing RCTs in CSDH, highlighting key areas of investigation and identifying directions for future research. Clinical trial registries – including the Cochrane Controlled Register of Trials, WHO ICTRP, clinicaltrials.gov, and Clinical Trials Information System – were systematically searched for RCTs on CSDH from June 1, 2019, to February 18, 2025. Both published and ongoing trials were included in this review. This review identified 41 recently published RCTs and 54 ongoing RCTs, compared to 26 ongoing trials in 2019. Of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
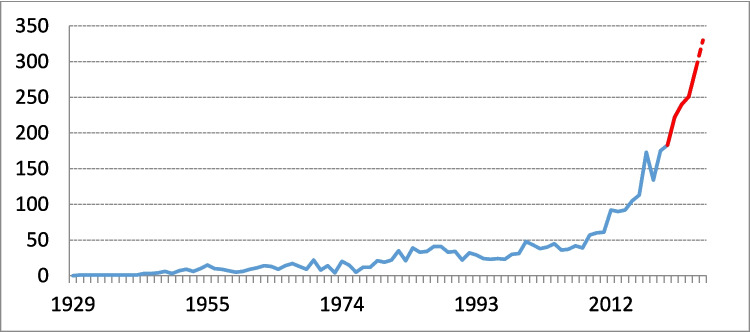 Figure 1
Figure 1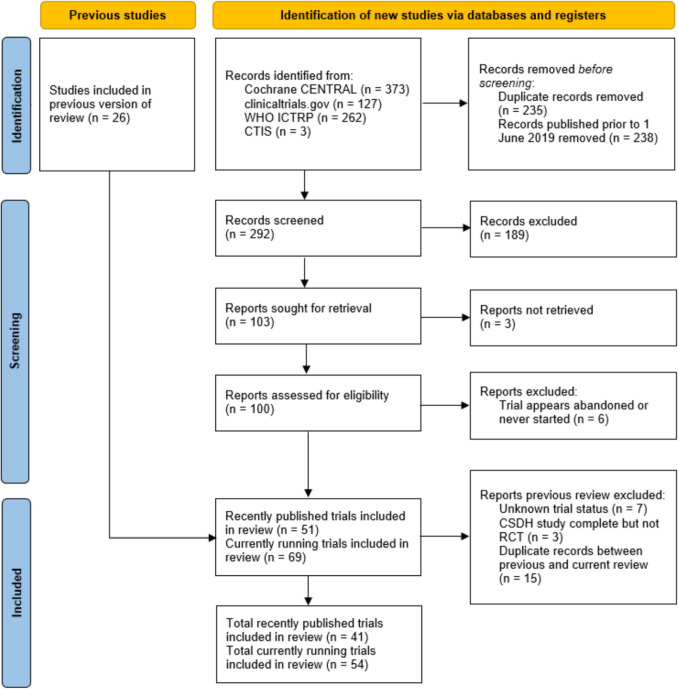 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurosurgical Procedures and Complications · Traumatic Brain Injury and Neurovascular Disturbances · Epilepsy research and treatment
Introduction
Chronic subdural haematoma (CSDH) is one of the most common neurosurgical conditions. It occurs most frequently in elderly patients, with an incidence that continues to rise due to the aging population [5, 9, 90, 104, 119]. Despite its prevalence, there is currently no consensus on the optimal treatment strategy for CSDH.
The current management of CSDH involves a broad range of treatment options. Surgical intervention, particularly burr hole evacuation with postoperative drainage, remains the most widely used approach for symptomatic CSDH [15, 40, 93, 111]. However, variations in surgical technique persist, not only globally but also at national and even intrahospital levels [12, 13, 50, 67]. These variations include, among other factors, the type and duration of postoperative drainage, the choice between general or local anesthesia, and the number of burr holes used. Alternative treatment strategies may also be considered depending on the patient’s clinical presentation. These may include different surgical interventions, such as craniotomy, pharmacological therapies, middle meningeal artery embolisation (MMAE), or watchful waiting. The publication of recent clinical practice guidelines represents an important step toward standardizing CSDH care [106, 118]. These guidelines, however, acknowledge the limited evidence supporting both optimal surgical and non-surgical approaches, emphasising the need for further high-quality research to address these gaps.
To address these evidence gaps, randomised controlled trials (RCTs) play a crucial role in advancing evidence-based care for CSDH. A systematic review conducted in 2019 by the international COllaborative Research Initiative on Chronic subdural haematoma (iCORIC) identified 26 active RCTs investigating treatment approaches for CSDH [35]. This review highlighted the growing interest in improving CSDH outcomes and emphasized the need for future RCTs to guide clinical decision-making. In the years since, this research field has continued to expand exponentially, reflected by a significant increase in the number of CSDH-related publications (Fig. 1).Fig. 1. Evolution of the number of publications per year on chronic subdural haematoma from 1929 to 2025, based on title-specific search terms: (chronic) AND (subdural) AND (hematomas OR haematomas OR hemorrhages OR haemorrhages OR hematoma OR haematoma OR hemorrhage OR bleeding). The red segment marks recent years (2020–2025), representing the period since the previous review. The dashed line indicates the number of publications for 2025, extrapolated based on trends from previous years
Importantly, several of the RCTs identified in the 2019 review have now been completed, providing valuable insights into the field and have already been translated into clinical practice. For example, trials on steroids as either an adjunct or alternative to surgery in CSDH demonstrated inferior outcomes for treatment with dexamethasone [53, 76]. This has led to a significant move away from steroid use in CSDH, which is reflected in clinical practice guidelines in some countries [59, 118]. This demonstrates the significant and rapid influence well-designed RCTs can have on clinical practice and in shaping future research directions. Alternative pharmacological agents such as tranexamic acid and statins are now more of a research focus, alongside the minimally invasive MMAE.
Considering the progress made in CSDH therapies since 2019 and the emergence of new studies, this systematic update of RCTs in CSDH is aimed to help inform both clinicians and researchers of current evidence in this field. Critical evaluation of recently completed and ongoing RCTs will provide a comprehensive overview of the therapeutic landscape, identify overlap between studies, and propose directions for future research to address persistent knowledge gaps.
Methods
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement [96]. The review was prospectively registered in the PROSPERO register under the identifier CRD42024604895.
Four trial registries were systematically searched from June 1, 2019 to February 18, 2025: the Cochrane Controlled Register of Trials (CENTRAL), the World Health Organization International Clinical Trials Registry Platform (WHO ICTRP), clinicaltrials.gov, and Clinical Trials Information System (CTIS). The search strategy from the 2019 review was updated and is detailed in Table 1. Table 1. Search terms for trials databasesCochrane CENTRALWHO ICTRPClinicaltrials.govCTIS (separate searches)([mh "Hematoma, Subdural, Chronic"] OR (Chronic* NEAR/3 ((subdural*) NEAR/3 (hematom* OR haematom* OR hemorrhag* OR haemorrhag* OR bleeding*))):ab,ti,kw)subdural AND hematoma OR subdural AND haematoma OR subdural AND hemorrhage OR subdural AND haemorrhage OR subdural AND bleeding((subdural) AND (hematoma OR haematoma OR hemorrhage OR haemorrhage OR bleeding))- subdural hematoma- subdural haematoma- subdural hemorrhage- subdural haemorrhage- subdural bleeding
Two independent reviewers (RF, DCH) screened the titles and abstracts of all identified trials published from June 1, 2019 up to February 18, 2025. Trials were excluded if they were duplicates, did not focus on CSDH, or were not an RCT by design. Both ongoing and published trials were included if a summary was available in English. Any disagreements between the reviewers were resolved through discussion until consensus was reached.
The final list of identified trials was further categorized into two groups: published trials and ongoing trials. Trials that appeared in both groups were removed from the ‘ongoing’ category. However, if only interim results had been published and the trial was still ongoing, it remained in the ‘ongoing’ category and was excluded from the ‘published’ group. The trials included in the 2019 review were cross-referenced with the new set of trials to ensure overlap and to categorize them as either ‘published’ or ‘ongoing’, based on their current status.
Ongoing trials underwent further review to verify their status. This process involved electronic searches of research groups and trial titles, as well as email communication with registered principal investigators (PIs) to assess trial progress and estimated completion dates. Trials were excluded if they were explicitly reported as abandoned or if there was no response from the PI and the estimated completion date was at least three years prior to the search.
The methodology of all published trials was assessed using the Cochrane Risk of Bias 2 (RoB 2) tool [116]. One reviewer (RF) conducted the initial assessment of all trials. In cases of uncertainty, the final judgment was reached through discussion and consensus with two additional reviewers (DCH, EE).
Results
A total of 291 eligible records were identified and screened for inclusion following the search strategy. After initial screening, 100 articles met the inclusion criteria. Of these, 6 trials were either apparently abandoned or never initiated, leaving 94 studies for further analysis. Cross-referencing with ongoing trials identified in the 2019 review led to the inclusion of one additional study, bringing the final total to 95 trials. These were categorized as published trials (n = 41) and ongoing trials (n = 54) (Fig. 2). Among the published trials, eleven had been identified in the previous review, along with five of the ongoing trials.Fig. 2. Flowchart of the identification, screening and inclusion of RCTs in this review
The RCT topics were categorized into the most common trial themes; steroids, tranexamic acid, other pharmacological agents, surgical techniques, perioperative management, MMA embolisation, and miscellaneous trials. The published and ongoing trials are presented in Tables 2 and 3, respectively. Table 2. Overview of all recently published RCTs in CSDH included in reviewReferenceTrial name; titlePrimary objectiveYearCountryTrial designNRoBPatientsInterventionComparisonOutcome (primary)ConclusionsSteroid trials = 5P. J. Hutchinson et al. [53]Dex-CSDH; DXM for CSDHTo assess the effect of a 2-week tapering course of DXM on functional outcomes in patients with symptomatic CSDH2020United KingdomMulticenter, double-blind, placebo-controlled RCT748Low riskPatients ≥ 18 years with symptomatic CSDH, predominantly iso- or hypodense on imagingDXM for 14-day tapering course; starting with 16 mg/day for 3 days, reducing every 3 daysPlacebo as per DXM regimenModified Rankin Scale at 6 monthsIn adults with symptomatic CSDH, most of whom underwent surgical evacuation during the index admission, treatment with DXM resulted in fewer favorable outcomes and more adverse events than placebo at 6 months, but resulted in fewer repeat operationsI. P. Miah et al. [76]DECSA; DXM versus surgery for CSDHTo investigate noninferiority of primary DXM therapy versus BHC on functional outcome2023NetherlandsMulticenter, noninferiority RCT with PROBE design252Low riskPatients ≥ 18 years with CSDH with MGS 1–3DXM for 20-day tapering course; starting with 16 mg/day for 4 days, reducing every 3 daysBurr hole craniostomyModified Rankin Scale at 3 monthsDXM treatment was not found to be noninferior to burr-hole drainage with respect to functional outcomes and was associated with more complications and a greater likelihood of later surgeryS. Ng et al. [91]HEMACORT; Corticosteroids as adjuvant treatment to surgery in CSDHTo compare the recurrence rate at 6 months in patients receiving post-operative prednisolone or placebo2021FranceMulticenter, triple-blind, placebo-controlled RCT155Low riskPatients ≥ 18 years with primary symptomatic CSDH (hypo- or isodense on imaging) treated with surgeryPrednisone within 72 h of surgery, 1 mg/kg/day for 1 week. Decreasing by 10 mg/week until 5 mg/day for last week (average 2 months)Placebo as per prednisone regimenClinical and radiological recurrence of CSDH within 6 months postoperativelyPrednisone, as an adjuvant treatment to surgery, may reduce early radiological recurrence of CSDH, although clinical benefits are unclearJ. Tariq et al. [121]Adjunctive postoperative DXM in CSDHTo compare the effect of BHC with and without a postoperative course of DXM on the recurrence rate of CSDH2021PakistanSingle-center, parallel RCT92High riskPatients ≥ 18 years with CSDH and required BHCDXM initiated preoperatively (16 mg/day) and tapered over two weeks postoperatively following BHC reducing 3 mg every 3 daysBHC without DXMComplication rate and recurrence of CSDH within 12 weeks postoperativelyNeurological and radiological outcome, and mortality rates were similar in both groups. The recurrence rate was lower and the complication rate higher in the DXM group, but not statistically significantK. Mebberson et al. [75]Adjuvant DXM with surgery for CSDHTo evaluate the efficacy and safety of adjuvant DXM in reducing recurrence rates after CSDH surgery with postoperative drainage2020AustraliaSingle-center, triple-blind, placebo-controlled RCT presenting interim results47High riskPatients ≥ 18 years with symptomatic CSDH on CT requiring surgical evacuationDXM for 14-day tapering course; starting with 16 mg/day for 3 days, reducing 4 mg every 3 daysPlacebo as per DXM regimenPostoperative mortality And recurrence rate requiring reoperation within 6 months, and postoperative morbidity by 30 daysInterim analysis suggested that DXM was safe and significantly reduced recurrence ratesTranexamic acid trials = 2T. Yamada et al.* [133]TXA and Goreisan preventing CSDH recurrenceTo evaluate the efficacy of orally administered TXA and Goreisan in preventing recurrence after BHC for CSDH2020JapanSingle-center, 3-arm RCT193High riskPatients undergoing initial BHC for CSDH* TXA group: 750 mg orally per day from day after surgery for 3 months* Goreisan group: 7.5 g orally per day for 3 monthsNo medicationRecurrence of CSDH within 3 months requiring reoperationOral administration of TXA or Goreisan does not minimize recurrence after BHC for CSDH; however, TXA can reduce the haematoma volumeK. R. Wan et al. [128]TXA for reducing CSDH recurrenceTo assess whether adding TXA to standard neurosurgical treatment reduces reoperation rates for recurrent CSDH2020SingaporeMulticenter, open-label RCT90High riskPatients ≥ 21 years with CSDH requiring surgeryStandard neurosurgical treatment with TXA (500 mg twice daily for 21 days)Standard neurosurgical treatment onlyRecurrence of CSDH requiring reoperation within 6 months postoperativelyThe addition of TXA treatment did not significantly reduce recurrence. TXA did cause a delay in CSDH recurrence and a reduced residual haematoma volume at 6 weeks, but not sustained beyond 6 weeksOther pharmacological trials = 8N. Fujisawa et al. [45]Effect of Goreisan to prevent CSDH recurrenceTo investigate whether Goreisan treatment decreases the recurrence rate of CSDH2020JapanSingle-center, parallel RCT224High riskPatients who underwent initial surgery for symptomatic CSDH confirmed on CTGoreisan (7.5 g three times a day for at least 3 months)No medicationSymptomatic recurrence of CSDH within 3 months postoperativelyAdjuvant Goreisan treatment did not prove beneficial, although it approached significance to lower the recurrence rate in overall patientsT. Yamada et al.* [133]TXA and Goreisan preventing CSDH recurrenceTo evaluate the efficacy of orally administered TXA and Goreisan in preventing recurrence after BHC for CSDH2020JapanSingle-center, 3-arm RCT193High riskPatients undergoing initial BHC for CSDH* TXA group: 750 mg orally per day from day after surgery for 3 months* Goreisan group: 7.5 g orally per day for 3 monthsNo medicationRecurrence of CSDH within 3 months requiring reoperationOral administration of TXA or Goreisan does not minimize recurrence after BHC for CSDH; however, TXA can reduce the haematoma volumeKamenova et al. [65]SECA; CSDH and aspirinTo investigate the impact of continuing or discontinuing low-dose aspirin after CSDH surgery2025SwitzerlandDouble-blind, placebo-controlled RCT150Low riskPatients ≥ 18 years with CSDH already taking low-dose aspirin (100 mg/day) for secondary preventionAcetylsalicylic acid (ASA) (100 mg/day) for 12 days then resumed normal ASA treatmentPlacebo for 12 days then resumed normal ASA treatmentRecurrence requiring reoperation within 6 monthsDiscontinuing ASA treatment did not reduce the recurrence rate of surgically treated CSDH within 6 monthsM. Shafiei et al. [112]Safety and timing of enoxaparin initiation after CSDH evacuationTo investigate the safety and timing of enoxaparin in the postoperative period in CSDH operated with BHC2023IranMulticenter, partially assessor-blinded RCT136High riskPatients with CSDH eligible for surgical evacuationEnoxaparin initiated 24 h after surgeryEnoxaparin initiated 72 h after surgeryIncidence of postoperative venous thromboembolism (VTE) and intracranial haemorrhagic eventsIn terms of VTE chemoprophylaxis, following BHC for CSDH, enoxaparin (early or late) will effectively prevent VTE development without any clinically significant rebleedingH. Matsumoto et al. [73]Japanese herbal medicine for preventing recurrent CSDHTo investigate the effect of 3 months of Goreisan versus Saireito for CSDH recurrence after surgical drainage2024JapanSingle-center, 3-arm RCT118High riskPatients > 20 years who underwent initial surgery for symptomatic unilateral CSDH with objective neurological deficits* Goreisan (6.0 g twice per day) for 3 months after surgery* Saireito (8.1 g twice per day) for 3 months after surgeryNo medicationSymptomatic recurrence of CSDH requiring reoperation within 3 months postoperativelyJapanese herbal medicine (Goreisan and Saireito) significantly reduced postoperative recurrence in CSDHD. Wang et al. [129]CSDH treatment with ATO and low-dose DXMTo test the hypothesis that adding DXM to ATO potentiates the effects of ATO on CSDH2020ChinaSingle-center, open-label, assessor-blinded, proof-of-concept RCT60High riskPatients ≥ 18 years with primary CSDH with MLS < 1 cm, MGS < 3, and no immediate need for surgeryATO (20 mg daily for 5 weeks) combined with low-dose DXM (2.25 mg daily for 2 weeks, 0.75 mg twice daily for 2 weeks, then once daily for 1 week)ATO (20 mg daily for 5 weeks) aloneHaematoma reduction at 5 weeksATO + DXM resulted in significantly greater haematoma reduction and neurological improvement than ATO aloneK. Yang et al. [134]Efficacy and safety of ATO for CSDHTo observe the effects of ATO on clinical efficacy, neurological function, inflammation, haematoma absorption, adverse reactions and recurrence rate in patients with CSDH2020ChinaSingle-center, parallel RCT58High riskPatients with symptomatic CSDH on imaging showing haematoma thickness < 5 mm, MLS < 1 cm, and suitable for conservative managementOral ATO 20 mg daily for two months alongside standard conservative managementStandard conservative management with conventional nutritional neuropharmacology but without ATOEffectiveness and safety of the treatmentAtorvastatin could reduce inflammatory response, promote haematoma absorption, protect neurological status and reduce the recrudescence rate for patients with CSDHA. B. Pradhanang et al. [99]Prophylactic phenytoin against postoperative seizure for CSDH patientsTo evaluate the efficacy of prophylactic phenytoin in preventing early postoperative seizures in patients undergoing burr hole drainage for CSDH2019NepalSingle-center parallel RCT54High riskPatients ≥ 14 years with imaging confirmed CSDH requiring surgical interventionIntravenous phenytoin (loading dose of 17 mg/kg followed by 100 mg three times daily for 7 days postoperatively)No antiepileptic drug administrationOccurrence of early postoperative seizureIncidence of postoperative seizure in patients undergoing burr holedrainage for CSDH was low. Routine prophylactic use of phenytoin, did not reduce seizure in the early postoperative periodSurgical trials = 13R. Raj et al. [100]FINISH; Burr hole drainage with or without irrigation for CSDHTo test the therapeutic effect of haematoma irrigation2024FinlandMulticenter, double-blind (except operating neurosurgeon and OR staff), noninferiority RCT589Low riskPatients ≥ 18 years with symptomatic CSDH requiring burr-hole drainage, hypo- or isodense on imagingBurr hole drainage without irrigationBurr hole drainage with irrigation with saline at body temperature (± 37 °C)Symptomatic recurrence requiring reoperation within 6 months postoperativelyBurr hole drainage without irrigation was not found noninferior to drainage with irrigation and had a higher reoperation rateA. Bartley et al. [11]SIC!; Irrigation fluid temperature in the evacuation of CSDHTo investigate the effect of irrigation fluid temperature on CSDH recurrence rate2022SwedenMulticenter RCT with blinding of patient, outcome assessor, and statistician541Low riskPatients ≥ 18 years with CSDH requiring burr hole evacuationBurr hole evacuation of CSDH with irrigation fluid at room temperature (± 22 °C)Burr hole evacuation of CSDH with irrigation fluid at body temperature (± 37 °C)Recurrence requiring reoperation within 6 monthsIrrigation at body temperature was superior to irrigation at room temperature in terms of fewer recurrencesJ. Duerinck et al. [33]COMPACT; Optimal surgical treatment for CSDHTo evaluate the 30-day reoperation rate in CSDH for mini-craniotomy, twist drill craniostomy, and BHC2022BelgiumMulticenter 3-arm RCT245Some concernsPatients ≥ 18 years with CSDH requiring surgery* Mini-craniotomy (bone flap > 30 mm replaced and drain)* Twist drill craniostomy (twist drill burr hole < 5 mm and drain)* Burr hole craniostomy (2 burr holes 5–30 mm and drain)NoneReoperation for recurrent or persistent CSDH within 30 days of primary surgeryAll 3 techniques are effective at treating patients with CSDH with eventual 6-month outcome being similar. BHC offers the lowest recurrence rate combined with manageable complication rate (not statistically significant)J. Soleman et al. [114]cSDH-Drain-Trial; Subperiostal drainage (SPD) versus subdural drainage (SDD)To investigate if SPD is noninferior to SDD in reducing recurrence rates of CSDH after burr-hole evacuation2019SwitzerlandMulticenter, assessor-blinded, noninferiority RCT220Low riskPatients ≥ 18 years with symptomatic CSDH on imaging requiring surgerySubperiosteal drainSubdural drainRecurrence of CSDH indicating reoperation within 12 monthsAlthough the noninferiority criteria were not met, SPD insertion led to lower recurrence rates, fewer surgical infections, and lower drain misplacement ratesD. Sale et al. [110]Single versus double burr hole drainage for CSDHTo compare the recurrence rate following double burr holes and a single burr hole for CSDH2021NigeriaSingle-center, parallel RCT192High riskPatients with imaging diagnosis of subacute or chronic SDHDouble burr hole drainageSingle burr hole drainageClinical recurrence within 6 monthsA single burr hole is as efficacious as a double burr hole in terms of relief of symptoms and recurrence, and it has a shorter duration of surgeryY. Bozhkov et al. [14]Efficacy of subperiosteal drains in CSDHTo evaluate the efficacy of subperiosteal drain placement in reducing recurrence rates after BHC in patients with CSDH2024GermanySingle-center, parallel RCT88High riskPatients ≥ 18 years with primary CSDH, suitable for BHCSingle BHC with saline irrigation followed by placement of a subperiosteal drainSingle BHC with saline irrigation without drain placementRecurrence of CSDH requiring reoperation within 3 months postoperativelySubperiosteal drain placement can be used safely and effectively to treat CSDH in conjunction with a single BHC procedure, significantly reducing the rate of recurrenceS. Zhang et al. [136]A novel active bone hole drainage system for CSDHTo evaluate the efficacy of a novel active bone hole drainage system in reducing post-operative subdural pneumatosis (PSP) after CSDH surgery2022ChinaSingle-center, assessor-blinded RCT86High riskPatients with traumatic, symptomatic CSDH on imaging requiring surgeryModified surgery with an active bone hole drainage system designed to reduce PSP by venting air during the procedureTraditional drilling and drainage surgery without the additional drainage systemIncidence of PSP and primary endpoints (recurrence of CSDH and post-operative haematoma re-increasement) within 6 monthsThe modified surgery significantly reduced PSP incidence and primary endpoints compared to traditional surgery, improving prognosisM. N. Stienen et al. [117]CORRECT-SCAR; Covers to improve aesthetic outcome after surgery in CSDHTo evaluate if burr hole covers improve patient satisfaction of the scar in CSDH surgery2024SwitzerlandSingle-center, patient-blinded RCT78Low riskPatients ≥ 18 years with primary CSDH (GCS > 8, able to communicate) requiring burr hole surgeryAny burr hole on intervention side is covered by a burr hole coverNone of the burr holes on the intervention side are covered by a burr hole coverPatient satisfaction (using patient-reported outcome And scale 1–10) with the aesthetic result of the scar at 90 daysSatisfaction with the aesthetic result of the scar among CSDH patients after burr hole surgery is very high, and this study does not show evidence for improvement by applying a burr hole coverT. Sun et al. [120]Drilling drainage combined with intraoperative MMA occlusion for CSDHTo evaluate the therapeutic efficacy of drilling drainage combined with intraoperative MMA occlusion in managing CSDH2024ChinaSingle-center, parallel RCT72Some concernsPatients > 30 years with symptomatic CSDH on imaging requiring surgery, with MLS > 5 mm or haematoma thickness > 10 mmDrilling drainage with intraoperative occlusion (severing) of the MMA using Digital Subtraction Angiography (DSA) guidanceStandard surgical drainage without MMA occlusionRecurrence rate within 5 months postoperativelyMMA occlusion during drainage reduced the recurrence rate and shortened drainage tube retention time without increasing surgical complicationsM. Mahmoodkhani et al. [71]Half-saline (HS) vs. normal-saline (NS) in CSDH surgeryTo evaluate the efficacy and safety of HS serum as an irrigation solution in CSDH surgery using BHC2022IranMulticenter, statistician-blinded RCT61High riskPatients with CSDH eligible for BHC as treatmentHS irrigation during surgeryNS irrigation during surgeryUnspecifiedHS as an irrigation fluid in BHC effectively reduced postoperative effusion and hospital stay duration without considerable complicationsF. Roohollahi et al. [107]Effect of number of burr holes on CSDH recurrenceTo compare the effect of single burr hole versus double burr hole drainage on the recurrence rate of CSDH2023IranSingle-center, assessor-blinded RCT44Low riskPatients ≥ 18 years with primary CSDH on CT and with MLS > 5 mm requiring surgerySingle BHC with subperiosteal drainage and irrigationDouble BHC with subperiosteal drainage and irrigationRecurrence rate of CSDH requiring reoperation within 6 months postoperativelySingle BHC was equally effective as double BHC in terms of recurrence rates but had a significantly shorter surgical duration. Single BHC is recommended for all patientsO. Akar et al. [7]Simultaneous versus consecutive drainage of bilateral CSDHTo compare the clinical outcomes of simultaneous versus consecutive BHC for bilateral CSDH evacuation2024TurkeySingle-center, parallel RCT43Some concernsPatients ≥ 18 years with symptomatic bilateral CSDH measuring > 10 mm in thickness on both sidesSimultaneous BHC of bilateral CSDH under general or local anesthesia with subdural drainage placementConsecutive BHC, first evacuating the side with the thicker haematoma, followed by the contralateral side, with subdural drainage placementTreatment success rate at 12 months, defined by absence of surgical complications, recurrence requiring reoperation, and good clinical outcomesThere were no significant differences in outcomes between the simultaneous and consecutive evacuation groupsK. Pathoumthong et al. [97]Subdural drain (SDD) versus subperiosteal drain (SPD) for CSDHTo compare the clinical and radiographic outcomes of SDD versus SPD placement in patients undergoing burr hole evacuation for CSDH2021ThailandSingle-center parallel RCT42Some concernsPatients ≥ 18 years with symptomatic CSDH on imagingBHC followed by SDD placement (subdural drain inserted through frontal burr-hole and connected to a gravity drainage system)BHC followed by SPD placement (subperiosteal drain connected to a suction drainage system)Clinical And radiographic recurrence of CSDH within 6 monthsDrain type (SDD or SPD) has no effect on the outcome. The surgeon’s preference determines which procedure is usedPerioperative management trials = 8T. S. R. Jensen et al. [60]24vs48CSDH; Subdural drainage time after CSDH evacuationTo investigate the effect of drainage duration on recurrence and mortality after burr-hole evacuation of CSDH2021DenmarkMulticenter, double-blind (until 24 h postoperatively) RCT420Some concernsPatients ≥ 60 years with symptomatic CSDH confirmed on imaging48 h postoperative passive subdural drainage24 h postoperative passive subdural drainageRecurrence requiring reoperation within 90 daysNo significant differences in the rates of recurrent haematoma or death during 90-day follow-up were identified between 24 and 48 h passive subdural drainage after burr hole evacuation of CSDHM. Hjortdal Grønhøj et al. [49]DRAIN TIME 2; Optimal drainage after evacuation of CSDHTo investigate the shortest possible drainage time without increasing the haematoma recurrence rate2024DenmarkMulticenter, assessor-blinded, 3-arm noninferiority RCT (patients and treating physicians blinded until 6 h post-surgery)347Some concernsPatients ≥ 18 years with symptomatic CSDH, predominantly iso- or hypodense on imaging, undergoing single burr-hole evacuation with a passive subdural drain* 6 h postoperative passive subdural drainage* 12 h postoperative passive subdural drainage24 h postoperative passive subdural drainageSymptomatic haematoma recurrence within 3 months requiring reoperation6 h and 12 h drainage times resulted in significantly higher recurrence rates compared to 24 h. 24 h drainage is recommended as the standard approachS. Sousa et al. [115]GET-UP; Impact of early out-of-bed in postoperative outcomes of CSDHTo compare early mobilisation and 48 h bed rest on postoperative complications2023PortugalSingle-center, open-label RCT with retrospective outcome assessment review208Some concernsPatients ≥ 18 years with CSDH requiring BHC drainageEarly mobilisation within 12 h post-surgery with closed subdural drains (removed 48 h post-surgery)Bed rest with head of bed at 0° for 48 h and subdural drains removed > 48 h post-surgeryMedical complications until discharge: infections, venous thromboembolism, seizuresEarly mobilization was associated with a reduction in medical complications without a significant effect on surgical recurrence, compared with a 48-h bed rest protocolR. Hestin et al. [47]NEURANESTH; General anaesthesia versus locoregional anaesthesia for CSDHTo compare the effect of local versus general anaesthetic during CSDH surgery on length of stay and functional outcome2022FranceSingle-center, assessor-blinded RCT60Low riskPatients ≥ 18 years with CSDH requiring surgeryGeneral anaesthesia with propofol (2.5 mg/kg), remifentanil (1 yg/kg), atracurium (0.5 mg/kg) and orotracheal intubation with mechanical ventilationLocoregional anaesthesia with Lidocaine 1% for a scalp nerve blockLength of post-operative hospitalisation required until fit for following completion of medical checklistIn patients requiring CSDH evacuation, general and regional anaesthesia are comparable in terms of duration of time until medically fit for discharge and occurrence of postoperative complicationsS. Anand et al. [8]Superficial cervical plexus block for neck pain after CSDH surgeryTo assess the effect of unilateral superficial cervical plexus block (SCPB) on managing neck pain as assessed by the numerical rating scale (NRS)2024IndiaDouble-blind, placebo-controlled RCT60Low riskPatients ≥ 18 years with unilateral CSDH, ASA grade I-III, undergoing BHCUltrasound-guided SCPB with 5 mL of 0.5% bupivacaine plus 1 mL of dexmedetomidine (50 µg/ml) administered preoperativelyPlacebo SCPB using 5 ml of normal saline administered preoperativelyNRS pain score during neck movement in the postoperative periodPreoperative superficial cervical plexus block decreases neck pain and facilitates neck rotation in the postoperative period. It also decreases the analgesic requirement in the post-operative periodA. Kamel et al. [64]Monitored anesthesia care of CSDHTo compare the efficacy and safety of combining dexmedetomidine with ketamine (DK) versus propofol (DP) for monitored anesthesia care during BHC for CSDH2024EgyptSingle-center RCT with blinding of patient and outcome assessor56Low riskPatients 50–80 years, ASA physical status II-III, BMI 25–35 kg/m^2^, scheduled for burr hole evacuation of CSDH under monitored anesthesia careDK group: Initial bolus of ketamine (1 mg/kg) and dexmedetomidine (1 µg/kg), followed by continuous infusion of ketamine (0.5 mg/kg/h) and dexmedetomidine (0.5 µg/kg/h)DP group: Initial bolus of propofol (0.5 mg/kg) and dexmedetomidine (1 µg/kg), followed by continuous infusion of propofol (0.5 mg/kg/h) and dexmedetomidine (0.5 µg/kg/h)Onset of sedation measured by the modified Observer’s Assessment of Alertness and Sedation score (OAA/S)Combining dexmedetomidine with ketamine is safer than with propofol for effective monitored anesthesia care in high-risk patients undergoing BHC for CSDH, although it results in a longer onset of sedationM. M. Mohamed et al. [80]Magnesium sulphate adjuvant during scalp block for CSDH surgeryTo evaluate the efficacy and safety of magnesium sulphate as an adjuvant to bupivacaine and lidocaine during scalp block in patients undergoing CSDH evacuation surgery2024EgyptSingle-center RCT with blinding of patient and investigator38Low riskPatients ≥ 45 years with unilateral CSDH, ASA physical status II or III, and GCS 14–15 undergoing surgical evacuationScalp block with lidocaine (1%) and bupivacaine (0.25%) combined with 5 mL of magnesium sulphate (500 mg)Scalp block with lidocaine (1%) and bupivacaine (0.25%) without magnesium sulphateTime to first dose of postoperative rescue analgesiaMagnesium sulphate can effectively and safely be used as an adjuvant to bupivacaine and lidocaine during scalp block for postoperative pain managementR. Fahmy et al. [41]Magnesium sulphate versus fentanyl sedation during BHCTo compare the hemodynamic and analgesic effects of magnesium sulphate versus fentanyl as adjuncts to propofol-induced conscious sedation in CSDH evacuation2022EgyptSingle-center, triple-blind RCT32Low riskPatients > 50 years with unilateral CSDH, ASA physical status I–II, And GCS 14–15, requiring BHCMagnesium sulphate infusion (loading dose of 50 mg/kg followed by continuous infusion at 15 mg/kg/h) combined with propofol sedationFentanyl infusion (loading dose of 1 μg/kg followed by continuous infusion at 0.5 μg/kg/h) combined with propofol sedationAverage intraoperative systolic blood pressureMagnesium sulphate resulted in better hemodynamic stability and less incidence of nausea and vomiting compared to fentanylMMAE trials = 5J. Liu et al. [70]MAGIC-MT; Usual care versus MMAETo determine whether MMA embolisation reduces the risk of symptomatic recurrence or progression of nonacute SDH2024ChinaMulticenter RCT with partial PROBE design722High riskPatients ≥ 18 years with symptomatic nonacute SDH on imaging, producing mass effect, and with a premorbid modified Rankin Scale of 0–2MMA embolisation using the Onyx liquid embolic system, performed adjunctively to surgical or nonsurgical standard treatmentUsual care, including burr hole drainage or conservative management as decided by the treating physicianSymptomatic recurrence or progression of SDH within 90 daysMMA embolisation did not significantly reduce recurrence or progression at 90 days compared to usual care but did reduce serious adverse eventsJ. Davies et al. [29]EMBOLISE; Adjunctive MMAE for CSDHTo assess whether MMA embolisation adjunct to surgery reduces the risk of haematoma recurrence or progression in CSDH patients2024USAMulticenter, partially assessor-blinded, adaptive-design RCT400High riskPatients 18–90 years with symptomatic subacute or chronic SDH on CT requiring surgical evacuation, with haematoma thickness > 15 mm or MLS ≥ 5 mmSurgical evacuation combined with MMA embolisation using the Onyx liquid embolic systemSurgical evacuation aloneHaematoma recurrence or progression leading to reoperation within 90 daysMMA embolisation significantly reduced the risk of haematoma recurrence or progression requiring reoperation. Further study is needed to evaluate the safety of MMA embolisationE. Shotar et al. [113]EMPROTECT; MMAE to prevent CSDH recurrenceTo investigate whether MMA embolisation after surgery reduces the risk of CSDH recurrence in patients at high risk of postoperative recurrence2025FranceMulticenter RCT with PROBE design342Low riskPatients ≥ 18 years who have undergone BHC for a recurrent CSDH or for a primary CSDH with at least one high-risk factor for recurrenceMMA embolisation with microparticles within 7 days after BHCStandard medical careRecurrence of CSDH within 6 monthsMMA embolisation did not lead to a significantly lower rate of recurrence at 6 months compared with standard medical care aloneD. Fiorella et al. [43]STEM; Adjunctive MMAE versus standard treatmentTo evaluate whether adjunctive MMA embolisation reduces the risk of treatment failure in patients with symptomatic CSDH2024USAMulticenter, open-label, international RCT310High riskPatients ≥ 18 years with symptomatic CSDH on imaging (≥ 50% iso- or hypodense) measuring > 10 mm in thicknessMMA embolisation using the Squid liquid embolic system, performed adjunctively to surgical or nonsurgical standard treatmentStandard treatment alone, either surgical or nonsurgical as decided prior to randomizationComposite of recurrent or residual CSDH (> 10 mm), reoperation or surgical rescue, or major disabling stroke, myocardial infarction, or death from neurologic causes at 180 daysAdjunctive MMA embolisation significantly reduced the risk of treatment failure without increasing the incidence of disabling stroke or death. The benefit was greater in patients receiving nonsurgical standard treatmentS. Ng et al. [92]MMAE as adjuvant to surgery for CSDHTo assess the effect of MMA embolisation as an adjuvant to surgery on haematoma volume resorption in symptomatic CSDH patients2020FranceSingle-center, assessor-blinded, pilot RCT46Some concernsPatients ≥ 18 years with symptomatic primary CSDH on CT requiring surgerySurgical treatment (twist drill craniostomy or craniotomy with drainage) followed by MMA embolisationSurgical treatment alone (twist drill craniostomy or craniotomy with drainage)Haematoma volume resorption at 3 months postoperativelyMMA embolisation significantly improved haematoma volume resorption at 3 months. Both groups had one recurrence, with no embolisation-related complicationsMiscellaneous trials = 1K. Osuka et al. [94]Sequential expression of chemokines in CSDH fluids after surgeryTo analyze the sequential expression of chemokines in CSDH fluids after trepanation surgery with or without irrigation2021JapanSingle-center, parallel RCT20Some concernsPatients undergoing trepanation surgery for CSDHIrrigation of CSDH fluid with artificial cerebrospinal fluid during surgery, followed by drainageNon-irrigation, with placement of a drainage tube without fluid irrigationChanges in chemokine concentrations in CSDH fluids over timeNeutrophil- and macrophage-attracting chemokines increased by day 1 post-surgery, regardless of irrigation, suggesting their key role in early healingTrials addressing multiple topics are represented in multiple entries within the tableASA* American Society of Anesthesiologists, ATO atorvastatin, BHC burr hole craniostomy, CSDH chronic subdural haematoma, CT computed tomography, DXM dexamethasone, GCS Glasgow Coma Scale, IV intravenous, MGS Markwalder Grading Scale, MLS midline shift, OR operating room, PROBE Prospective Randomised Open, Blinded Endpoint, RCT randomised controlled trial, RoB risk of bias, TXA tranexamic acidTable 3Overview of all currently running RCTs in CSDH included in reviewTrial name; titleRegistered numberCountryPrimary objectiveTrial designCompletion dateNPatientsInterventionComparisonOutcome (primary)****Steroid trials = 3ATOCH II; Atorvastatin combined with dexamethasone in CSDHChiCTR1900021659 [17]ChinaTo evaluate the clinical efficacy and safety of atorvastatin combined with dexamethasone for CSDH patientsMulticenter, double-blind, placebo-controlled RCTUnknown240Patients 18–90 years with CSDH on imaging and mRS 1–3, requiring surgical treatmentATO 20 mg daily + DXM (0.75 mg thrice per day for 2 weeks, twice per day for 1 week, once per day for 1 week) for 4 weeks in totalATO 20 mg daily + placebo as per DXM regimen for 4 weeks in totalComprehensive outcome within 4 weeksADTCSDH; Combining atorvastatin and dexamethasone for CSDH after surgeryChiCTR2000030156 [18]ChinaTo explore the clinical effect of combining atorvastatin and dexamethasone in the treatment of CSDH drilling and drainageMulticenter, 3-arm, open-label RCTUnknown90Patients 18–90 years with symptomatic CSDH on imaging undergoing surgical drilling and drainage* ATO 20 mg daily for 4 weeks* ATO 20 mg daily + DXM (0.75 mg thrice per day for 2 weeks, twice per day for 1 week, once per day for 1 week) for 4 weeks in totalStandard postoperative neurosurgical monitoringRecurrence rate within 12 weeksADELE; ATO and DXM in CSDHRPCEC00000436 [108]CubaTo evaluate the efficacy and safety of ATO and DXM in the postoperative treatment of patients with CSDHOpen-label, 4-arm parallel RCTApril 202648Patients 19–80 years with CSDH on imaging requiring surgical treatment ATO and conventional treatment (ATO for 8 weeks: 20 mg/day)* DXM and conventional treatment (DXM for 4 weeks: 16 mg IV days 1–3, reducing every 3 days to 4 mg orally daily from day 11)* ATO, DXM, and conventional treatmentConventional treatment (supportive treatment) during hospital admissionReduction in volume and reduction in recurrences at baseline, the 7th day and at a monthTranexamic acid trials = 7TORCH; Tranexamic acid to prevent operation in CSDHNCT03582293 [125]NetherlandsTo investigate the efficacy and safety of TXA as primary conservative treatment of CSDHMulticenter, double-blind, placebo-controlled RCTOctober 2029554Patients ≥ 50 years with CSDH on CT safe for primary conservative treatment based on symptoms and signsTXA 1 g/day for 28 daysPlacebo as per TXA regimenSurgery for CSDH within 12 weeks of start of treatmentTXA for treatment of CSDHNCT06718751 [124]USATo establish the safety and efficacy of using TXA to resolve CSDH without the need for surgical interventionDouble-blind, placebo-controlled RCTJanuary 2026300Patients 21–95 years with CSDH and eligible for conservative treatmentTXA 650 mg/day for 21 weeksPlacebo as per TXA regimenRate of resolution measured as CSDH volume or diameter at 6, 12, And 21 weeksTABASCO; TXA versus MMA embolisation as an adjunctive therapyDRKS00033515 [31]GermanyTo determine whether postoperative treatment of CSDH using adjuvant TXA is equivalent to MMA embolisationMulticenter, open-label RCTUnknown276Patients ≥ 18 years who underwent surgery for primary unilateral CSDH < 24 h before inclusionPostoperative adjuvant drug therapy with TXAPostoperative adjuvant MMA embolisation on the affected side using digital subtraction angiographyPostoperative volume decrease through time within 3 monthsTRACS: TXA in CSDHNCT02568124 [82]CanadaTo investigate if TXA can be used as conservative treatment for CSDH, lowering surgical procedures and decreasing recurrenceMulticenter, double-blind, placebo-controlled RCTJune 2025130Patients ≥ 18 years with CSDH confirmed on CT containing a chronic componentTXA 750 mg/day until complete radiological resolution of CSDH or a maximum of 20 weeksPlacebo daily until complete radiological resolution of CSDH or a maximum of 20 weeksRate of CSDH resolution at 20 weeks without intervening unplanned surgical procedure (surgery is at discretion of treating team)TRACE 2; TXA in the treatment of residual CSDHNCT05713630 [122]CanadaTo evaluate the effectiveness of TXA in improving patient-reported quality of life and reducing CSDH recurrenceMulticenter, triple-blind RCTNovember 2030130Patients ≥ 45 years with symptomatic CSDH ≥ 8 mm in thickness on CT (any density), requiring either conservative management or surgeryStandard care + TXA: 1 g oral or IV loading dose followed by 500 mg TXA orally or IV three times daily for 45 daysStandard care + placebo: identical capsule or IV saline injection, mimicking the TXA regimenEuropean Quality of Life 5 Dimensions 5 Level (EQ-5D-5L) questionnaire every two weeks for 45 daysTRACE; TXA in the treatment of residual CSDHNCT04898712 [123]CanadaTo compare haematoma volume 4–8 weeks after CSDH surgery in patients receiving TXA versus no treatmentDouble-blind, placebo-controlled RCTRecruitment completeDecember 202390Patients ≥ 18 years with CSDH requiring surgeryTXA for 4–8 weeks post-surgery: < 60 kg: 1 g/day60–100 kg: 1.5 g/day > 100 kg: 2 g/dayPlacebo as per TXA regimenChange in haematoma volume in mL from immediately post-operative to repeat CT at 4–8 weeksPostoperative TXA in CSDH patientsNot registered [30]BrazilTo determine whether postoperative TXA reduces risk of complications and CSDH recurrence after BHCSingle-center, open-label RCTDecember 2025Unknown (50 in pilot)Patients ≥ 18 years with symptomatic CSDH undergoing BHCPostoperative TXA at 750 mg/day in 3 daily doses for 3 monthsNo TXARecurrence requiring reoperation within 6 monthsOther pharmacological trials = 8REACH; Atorvastatin in CSDHNCT03956368 [101]Hong KongTo evaluate the efficacy and safety of atorvastatin in patients with CSDHMulticenter, double-blind, placebo-controlled RCTRecruitment completeMarch 2023690Patients ≥ 18 years with CSDH on CTATO 20 mg daily for 8 weeksPlacebo as per ATO regimenFavourable mRS score of 0–3 at 6 monthsPeiyuan Huayu formula for CSDH treatmentChiCTR2300072255 [23]ChinaTo develop a new plan for the treatment of CSDH by combining traditional Chinese and Western medicineMulticenter, statistician-blinded RCTDecember 2025400Patients 18–85 years with CSDH on imagingConventional treatment and Peiyuan Huayu formulaConventional treatmentHaematoma volume and recurrence time of CSDHRELACS; Restarting early versus later anticoagulation for CSDH with atrial fibrillationNCT06696079 [105]FinlandTo assess the benefit of early resumption versus late resumption of oral anticoagulation medication in adults with atrial fibrillation undergoing surgery for CSDHInternational, multicenter, assessor-blinded RCTJune 2027332Patients ≥ 18 years with symptomatic CSDH (predominantly hypo- or isodense on imaging) requiring surgery and previously prescribed oral anticoagulation medication due to atrial fibrillationEarly resumption: oral anticoagulation therapy is resumed on the 5th postoperative dayLate resumption: oral anticoagulation therapy is resumed on the 30th postoperative dayComposite outcome: thromboembolic events, hemorrhagic events, and vascular death within 90 daysATOCH II; Atorvastatin combined with dexamethasone in CSDHChiCTR1900021659 [17]ChinaTo evaluate the clinical efficacy and safety of atorvastatin combined with dexamethasone for CSDH patientsMulticenter, double-blind, placebo-controlled RCTUnknown240Patients 18–90 years with CSDH on imaging and mRS 1–3, requiring surgical treatmentATO 20 mg daily + DXM (0.75 mg thrice per day for 2 weeks, twice per day for 1 week, once per day for 1 week) for 4 weeks in totalATO 20 mg daily + placebo as per DXM regimen for 4 weeks in totalComprehensive outcome within 4 weeksCHARM; Chinese herbal formula HuoXue LiShui for CSDHNCT06427980 [38]ChinaTo compare haematoma progression or recurrence requiring reoperation at 24 weeks in patients with CSDH treated with HuoXue LiShui and placeboMulticenter, double-blind, placebo-controlled RCTMarch 2026160Patients 18–90 years with primary CSDH or residual haematoma after burr hole drainage, with no immediate need for surgery (GCS ≥ 14 and mRS ≤ 2)Chinese Herbal formula HuoXue LiShui, one bag (28.5 g) twice daily after meals for 8 weeksPlacebo as per HuoXue LiShui regimenRate of (re)operation within 24 weeksADTCSDH; Combining atorvastatin and dexamethasone for CSDH after surgeryChiCTR2000030156 [18]ChinaTo explore the clinical effect of combining atorvastatin and dexamethasone in the treatment of CSDH drilling and drainageMulticenter, 3-arm, open-label RCTUnknown90Patients 18–90 years with symptomatic CSDH on imaging undergoing surgical drilling and drainage ATO 20 mg daily for 4 weeks* ATO 20 mg daily + DXM (0.75 mg thrice per day for 2 weeks, twice per day for 1 week, once per day for 1 week) for 4 weeks in totalStandard postoperative neurosurgical monitoringRecurrence rate within 12 weeksADELE; ATO and DXM in CSDHRPCEC00000436 [108]CubaTo evaluate the efficacy and safety of ATO and DXM in the postoperative treatment of patients with CSDHOpen-label, 4-arm parallel RCTApril 202648Patients 19–80 years with CSDH on imaging requiring surgical treatment ATO and conventional treatment (ATO for 8 weeks: 20 mg/day)* DXM and conventional treatment (DXM for 4 weeks: 16 mg IV days 1–3, reducing every 3 days to 4 mg orally daily from day 11)* ATO, DXM, and conventional treatmentConventional treatment (supportive treatment) during hospital admissionReduction in volume and reduction in recurrences at baseline, the 7th day and at a monthTissue plasminogen activator (tPA) for clearing CSDHNCT05491356 [86]CanadaTo determine the utility of tPA, administered intra-catheter during twist drill craniostomy, in the clearance of CSDHTriple-blind, placebo-controlled pilot RCTRecruitment completeJuly 202440Patients ≥ 18 years with symptomatic CSDH requiring surgical drainage via twist drill craniostomyIntra-catheter administration of 2 mL tPA during twist drill craniostomyIntra-catheter administration of 2 mL sterile 0.9% saline solution during twist drill craniostomyStudy feasibility, assessed by patient recruitment rate, protocol adherence, and unexpected events within 8 monthsSurgical trials = 10CSDH removal with or without intraoperative irrigationjRCT1041220124 [62]JapanTo evaluate the effectiveness of irrigation subsequent to the evacuation of CSDH utilizing artificial spinal fluidOpen-label, parallel RCTFebruary 20261186Patients ≥ 20 years old with symptomatic CSDH requiring surgical intervention of a single sideBHC followed by irrigation with ≥ 200 mL of artificial spinal fluid until the fluid is clear. A closed drain remains for ≥ 12 h postoperativelyBHC without irrigation, with drain placement alone and a closed drain for at least 12 h postoperativelyReoperation within 6 months postoperativelySUPERDURA; Active subperiosteal versus passive subdural drainageNCT06621407 [2]DenmarkTo test the hypothesis that 24 h active subperiosteal drainage is noninferior to 24 h passive subdural drainage after single burr hole evacuation of a unilateral CSDHMulticenter, noninferiority RCT with blinding of patient and outcome assessorApril 2028598Patients aged ≥ 18 years with unilateral CSDH on imaging undergoing single burr hole evacuation24 h active subperiosteal drainage24 h passive subdural drainageComposite outcome: mortality and recurrent CSDH requiring reoperation within 90 daysDifferent skull burr hole sites and CSDH prognosisChiCTR2000033967 [19]ChinaTo compare the efficacy of different skull bore hole sites on the prognosis of CSDH2-arm parallel RCTRecruitment completeDecember 2022200Patients with CSDH requiring surgical treatmentBurr hole via frontal boneBurr hole via parietal boneHaematoma residual volume and ratio, gas volume in haematoma cavity, recurrence, modified MGS and mRS scoreIntraoperative irrigation in CSDHJPRN-UMIN000040527 [126]JapanTo study the benefit of adding irrigation to simple drainage in CSDH surgery2-arm, parallel RCTUnknown120Patients ≥ 20 years with novel CSDH requiring surgeryBurr hole drainage with irrigationBurr hole drainageRecurrence rateAugmented reality for subdural drain placementNCT06052124 [87]USATo assess the accuracy and feasibility of augmented reality (AR) guided subdural evacuating portal sytem (SEPS) placementSingle-center, open-label RCT with sequential assignmentDecember 2025100Patients 18–90 years with chronic or subacute SDH planned to be treated by SEPSAR-guided SEPS placement (first as a pilot for usability in five patients, then to guide SEPS drains)Standard anatomical guided SEPS placementAccuracy of SEPS placement, measured in mm difference between AR-guided and standard placement based on post-procedure CT scansSubperiosteal versus subdural drain after BHCCTRI/2024/10/075273 [28]IndiaTo find if the recurrence rate of CSDH when treated with subperiosteal drainage is noninferior to subdural drain placement at three monthsNoninferiority RCT with blinding of patient and outcome assessorNovember 2026100Patients ≥ 18 years with symptomatic CSDH on imaging or asymptomatic CSDH with midline shift > 10 mm requiring surgerySubperiosteal placement of the drainage catheterSubdural placement of the drainage catheterRecurrence rate requiring reoperation within 3 monthsMinimally invasive puncture and burr hole drainage in CSDH patientsChiCTR2200059808 [22]ChinaTo compare the clinical efficacy of minimally invasive puncture and drilling drainage in the treatment of CSDH2-arm, parallel RCTUnknown80Patients ≥ 18 years with symptomatic CSDH (predominantly hypo- or isodense on imaging) requiring burr hole evacuationMinimally invasive punctureBurr hole drainageRecurrence rate, mortality, cure rate, and surgical failure rateEndoscopic evacuation versus craniotomy for evacuating CSDHCTRI/2023/08/057000 [27]IndiaTo compare the effectiveness of endoscopic evacuation versus craniotomy for evacuating of CSDHSingle center, open-label RCTSeptember 202560Patients with CSDH requiring surgical interventionEndoscopic evacuation via a single burr holeCraniotomy and evacuation of CSDHRecurrence rate at 1, 3, and 6 months after surgeryEvaluation of siphon method in CSDHIRCT20211130053232N1 [57]IranTo compare the possible advantages and disadvantages of siphon washing method with traditional method in CSDH2-arm, parallel RCT with blinding of patient and outcome assessorUnknown60Patients with CSDH on CT with neurological deficit, GCS decline, and/or gait disorderBurr hole drainage utilizing the siphon methodStandard burr hole drainageRecurrence rate within 12 monthsNeuroendoscopic and non-endoscopic surgical techniques in treating septated CSDHIRCT20190618043934N14 [56]IranTo compare neuroendoscopic and non-endoscopic surgical techniques in treating septated CSDHSingle-center RCT with blinding of patient and outcome assessorRecruitment completeSeptember 202260Patients diagnosed with mixed-density CSDH on imagingNeuroendoscopic surgeryStandard surgical managementDuration of surgery, mortality, morbidity, recurrence rate within 6 months, and duration of hospitalizationPerioperative management trials = 7BP-CSDH; Body posture in preventing CSDH RecurrenceNCT06401772 [36]ChinaTo investigate the effectiveness and safety of body posture to improve intracranial pressure in CSDHMulticenter, assessor-blinded RCTJanuary 2028830Patients ≥ 60 years with symptomatic CSDH, with thickness ≥ 10 mm and MGS ≤ 2, undergoing burr hole drainageIntracranial hypotension targeted body posture, requiring lower limb elevation (30°) over head level for 3 months post-surgery when possibleStandard supine positioning post-surgerySymptomatic recurrence with haematoma thickness ≥ 10 mm within 90 days postoperativelyECHO; Exhaustive versus fixed-time drainage for CSDHNCT04573387 [103]ChinaTo evaluate whether exhaustive drainage after one burr-hole craniostomy reduces recurrence rates and improves clinical outcomesMulticenter, assessor-blinded RCTRecruitment completeDecember 2024309Patients 18–90 years with symptomatic CSDH on imagingExhaustive drainage following BHC, where the drain remains until haematoma volume is minimized, with up to 3 urokinase injections if neededFixed-time drainage following BHC, where the drain is removed 48 h postoperativelyRecurrence requiring reoperation within 6 months postoperativelyNerve block and sedative anesthesia versus general anesthesiaNCT05888389 [109]ChinaTo evaluate the safety of nerve block anesthesia combined with sedative anesthesia versus general anesthesia during BHC with drainage for CSDHMulticenter, assessor-blinded, noninferiority RCTDecember 2025190Patients 18–80 years with CSDH requiring surgical treatment and with haematoma thickness > 10 mm or midline shift > 10 mmCranial nerve block anesthesia combined with IV dexmedetomidine for sedation at a rate of 2−4ug/kg for 10 min, followed by a continuous infusion of 0.5-1ug/kg/h until RASS −3General anesthesia with propofol or etomidate, sufentanil, rocuronium or cisatracuriumIncidence of intraoperative body movementDexmedetomidine during awake craniotomyPACTR202408593043200 [95]EgyptTo detect role of administration of dexmedetomidine during awake craniotomy on the inflammatory and stress response, potentially improving postoperative recoveryPatient-blinded, parallel RCTRecruitment completeDecember 202462Patients 18–90 years with CSDH and scheduled for elective craniotomyAwake craniotomy with dexmedetomidine: loading dose of dexmedetomidine at 1 μg/kg over 10 min, followed by a continuous infusion of 0.2–0.7 μg/kg/hr during the surgeryGeneral anesthesia with agents such as propofol, fentanyl, and sevofluraneLevels of inflammatory markers (C-reactive protein [CRP], interleukin-6 [IL-6], interleukin-8 [IL-8]) measured preoperatively, immediately postoperatively, and at 24 and 48 h postoperativelyKetofol versus dexmedetomidine as sedation for CSDH surgeryCTRI/2022/09/045494 [26]IndiaTo compare dexmedetomidine to ketofol for sedation to keep patients hemodynamically stable during operationSingle-center, open-label RCTRecruitment completeSeptember 202360Patients 20–65 years with CSDH requiring burr hole evacuationDexmedetomidine 1 µg per kg as loading dose followed by infusion at 0.2–0.7 mcg/kg/hr IVKetofol 0.5 mg per kg per hour IVIntraoperative hemodynamicsABC-SDH trial I; Awake BHC in CSDH patientsDRKS00034040 [32]GermanyTo determine whether awake burr hole trepanation under local anesthesia is a safe and feasible alternative to general anesthesiaSingle-center, open-label, safety and feasibility RCTRecruitment completeDecember 202450Patients ≥ 18 years with CSDH on imaging requiring surgeryBurr hole trepanation performed under local anesthesia (awake surgery)Burr hole trepanation performed under general anesthesiaRecruitment rate (consent rate and intended surgery rate after randomization) and complication rate within 1 month postoperativelyHOPE; High concentration oxygen for pneumocephalusNCT04725851 [48]Hong KongTo determine whether high-concentration oxygen therapy reduces pneumocephalus volume after burr hole drainage for CSDHSingle-center, assessor-blinded RCTRecruitment completeDecember 202436Patients ≥ 18 years with CSDH on imaging, treated with BHC, and presenting with postoperative pneumocephalusHigh-concentration oxygen therapy 12–15 L/min via Non-Rebreather Mask for 24 hRoom air or low-concentration oxygen therapy (0–2 L/min via nasal cannula)Reduction in pneumocephalus volume after 24 h on CTMMAE trials = 21PREMMA; Puerto Rico MMAE for CSDH trialNCT06466733 [89]Puerto RicoTo compare the effectiveness of MMA embolisation as a standalone treatment versus standard surgical evacuation via burr hole or craniotomyMulticenter, assessor-blinded RCTJuly 2031658Patients ≥ 21 years, with CSDH on imaging requiring treatment, with GCS ≥ 14 and MGS ≤ 2MMA embolisationStandard surgical evacuation, either BHC or craniotomyRecurrence requiring reoperation at 3, 6, and 12 monthsCOMPLEMENT; MMAE for CSDH patientsNCT06772740 [102]JapanTo assess the efficacy and safety of MMA embolisation for CSDH2-arm parallel RCT with PROBE designMarch 2029600CSDH patients ≥ 18 years with pre-mRS 0–3, haematoma thickness ≥ 10 mm, and ≥ 1 risk factor (e.g. age ≥ 75 years, bilateral haematoma, etc.)Conventional treatment with MMA embolisation within 7 days after randomizationConventional treatmentRate of recurrence of CSDH within 6 monthsLEADH; Cyanocrylate embolisation adjuvant to standard of careNCT05374681 [68]FranceTo evaluate the effectiveness of MMA embolisation in CSDHMulticenter, assessor-blinded RCTSeptember 2026550Patients ≥ 18 years with CSDH > 10 mm on CT, localized to convexityMMA embolisation with cyanoacrylates adjunct to surgical or conservative management as decided by the neurosurgeonSurgical or conservative management alone as decided by the neurosurgeonClinical or radiographic recurrence of CSDH within 6 monthsCHESS; CSDH with embolisation versus surgeryNCT06347796 [88]USATo test in moderately symptomatic CSDH patients if MMA embolisation can be used as an alternative to conventional open surgeryMulticenter, assessor-blinded RCTSeptember 2028520Patients 40–90 years with unilateral CSDH (≥ 10 mm in thickness) or bilateral CSDH (one side no symptoms and < 5 mm in thickness). CSDH at least 2/3 iso- or hypodenseParticle MMA embolisationSurgical drainage through BHC or craniotomyNeed for reoperation or death within 180–210 daysMETRICS; MMAE for high-risk intractable CSDHChiCTR2000032464 [21]ChinaTo evaluate whether MMA embolisation reduces treatment failure compared to traditional treatment strategies in patients with high risk for CSDH recurrenceMulticenter, assessor-blinded RCTRecruitment completeDecember 2024516Patients ≥ 18 years with CSDH on imaging and at least one risk factor for recurrence (e.g. > 80 years, use of antithrombotics, bilateral CSDH)MMA embolisation, either alone (for non-surgical patients) or adjunct to surgical evacuation (for surgical patients)Traditional strategies, including oral atorvastatin (20 mg daily for 8 weeks) for non-surgical patients and BHC for surgical patientsTreatment failure defined as substantial residual haematoma, haematoma enlargement, or recurrence/haematoma progression requiring reoperationEndovascular Therapy Combined with Operation vs Simple operationChiCTR2000039359 [20]ChinaTo compare the prognosis of burr hole drainage standalone or combined with MMA embolisation in the treatment of CSDH2-arm, parallel RCTUnknown480Patients 18–70 years with symptomatic CSDH on imaging (hypo- or isodense, or mixed density with acute component < 50%) in need of surgical treatmentMMA embolisation combined with burr hole drainageBurr hole drainageRecurrence rateOTEMACS; Onyx™ Trial for MMAE for CSDHNCT04742920 [84]FranceTo assess the safety and effect on recurrence rate and functional outcome of endovascular treatment in patients with CSDHMulticenter, RCT with PROBE designSeptember 2025440Patients ≥ 18 years with symptomatic CSDH on imaging and pre-mRS ≤ 3MMA embolisation in addition to standard management with Onyx non-adhesive liquid embolic agentStandard management (surgical or conservative)Recurrence rate within 90 daysMMAE versus surgery for CSDHChiCTR2500096266 [16]ChinaTo evaluate the safety and efficacy of MMA embolisation compared with surgery in the treatment of CSDHMulticenter, assessor-blinded RCTOctober 2027386Patients 18–90 years with symptomatic CSDH (< 30% high-density components) and haematoma thickness > 15 mm or MLS > 5 mmMMA embolisation + standard drug adjuvant therapySurgery + standard drug adjuvant therapyRecurrence rate within 90 daysMEMBRANE; MMAE for CSDH with TRUFILL n-BCANCT04816591 [78]USATo investigate the effect of MMA embolisation as an adjunct to standard of care treatment for CSDHMulticenter, open-label RCTMay 2025376Patients 18–90 years with confirmed CSDH and a pre-randomization mRS ≤ 3MMA embolisation using TRUFILL n-BCA, in addition to standard surgical or medical managementStandard of care surgery or medical management onlyRecurrence or progression of CSDH requiring re-intervention within 180 daysEmbotrial-1; Endovascular vs conservative CSDH treatmentNCT06274580 [39]ItalyTo assess the superiority of MMA embolisation over conservative treatmentMulticenter RCT with PROBE designJanuary 2028300Patients ≥ 18 years with CSDH with MGS ≤ 1, haematoma width ≤ 20 mm, MLS ≤ 7 mm, and pre-mRS score ≤ 2MMA embolisation using polyvinyl alcohol particles or liquid embolizing materialsStandard conservative managementRate of incomplete haematoma resolution or need for surgical rescue within 6 monthsSWEMMA; Swedish trial on MMAE versus surgeryNCT05267184 [85]SwedenTo compare efficacy of MMA embolisation on rates of reoperation in CSDH patients with mild to moderate symptomsMulticenter, asessor-blinded RCTMarch 2027288Patients 18–89 years with CSDH requiring surgical treatment, MGS < 2, and GCS > 13MMA embolisation with liquid embolic agentsSurgical drainage through BHC or craniotomyReoperation rate of CSDH within 3 monthsTABASCO; TXA versus MMAE as an adjunctive therapyDRKS00033515 [31]GermanyTo determine whether postoperative treatment of CSDH using adjuvant TXA is equivalent to MMA embolisationMulticenter, open-label RCTUnknown276Patients ≥ 18 years who underwent surgery for primary unilateral CSDH < 24 h before inclusionPostoperative adjuvant drug therapy with TXAPostoperative adjuvant MMA embolisation on the affected side using digital subtraction angiographyPostoperative volume decrease through time within 3 monthsEMMA-Can; Management of CSDH with or without EMMANCT04750200 [72]CanadaTo investigate the effect of MMA embolisation as an adjunct to standard of care treatment for minimizing CSDH recurrenceOpen-label parallel RCTMarch 2026200Patients ≥ 18 years with baseline mRS ≤ 2 and with symptomatic CSDH requiring surgical drainage or haematoma thickness ≥ 10 mmMMA embolisation as an adjunct to the standard of careStandard of care, including medical and/or surigcal treatmentRadiographic recurrence of CSDH within 90 daysSTORMM; MMAE for CSDHNCT06163547 [77]SwitzerlandTo evaluate the efficacy of MMA embolisation in CSDHMulticenter, open-label RCTJanuary 2027180Patients ≥ 18 years with symptomatic CSDH or large asymptomatic CSDH after ≥ 6 weeks of failed conservative treatmentMMA embolisation performed within 72 h post-surgery or as a standalone treatment in non-surgical patientsStandard surgical treatment without embolisation or no intervention for non-surgical patientsClinical or radiographic recurrence of CSDH within 6 monthsELIMINATE; MMAE in CSDHNCT04511572 [55]NetherlandsTo investigate the effect of MMA embolisation as an adjunct to surgical evacuationMulticenter, open-label multicenter RCTOctober 2025170Patients 50–90 years with symptomatic CSDH on imaging requiring surgeryMMA embolisation within 72 h after BHCOnly BHCRecurrence requiring reoperation within 24 weeks after the interventionMEMBRANE; MMAE after CSDH evacuationNCT05327933 [79]GermanyTo show that additional MMA embolisation reduces the risk of recurrent bleeding in patients with CSDHAssessor-blinded, parallel RCTOctober 2025154Patients ≥ 18 years who were operated on by one or more burr hole trepanations for primary CSDHMMA embolisation using digital subtraction angiographyStandard of careRecurrence of CSDH within 3 monthsEfficacy of postoperative MMAEACTRN12621000263897 [3]AustraliaTo evaluate the effectiveness of postoperative MMAE in reducing recurrence rate, residual haematoma thickness, and improving functional outcomes in CSDHMulticenter, asessor-blinded RCTUnknown106Patients ≥ 18 years requiring surgical evacuation of symptomatic CSDH with a maximal thickness of ≥ 10 mmMMA embolisation following burr-hole or craniotomyStandard postoperative monitoring (no embolisation)Symptomatic recurrence requiring reoperation within 3 monthsMMAE as primary treatment for CSDHACTRN12621000202864 [4]AustraliaTo demonstrate that MMA embolisation can reduce the need for surgical evacuation in stable patientsSingle-center RCT with blinding of the outcome assessor and statisticianDecember 202572Patients ≥ 18 years with CSDH not requiring emergency surgical evacuationMMA embolisation with Onyx liquid embolic agentObservation with repeat CT brain at 6 weeks, 3 months, and 6 monthsSymptomatic recurrent/residual CSDH that requires surgical evacuation at 6 weeks, 3 months, and 6 monthsEndovascular embolisation for CSDH after surgeryNCT04272996 [83]USATo evaluate whether MMA embolisation following surgical evacuation of CSDH reduces the rate of recurrence compared to surgical evacuation aloneOpen-label, parallel RCTRecruitment completeJune 202460Patients 18–90 years with CSDH requiring surgical evacuation with GCS > 6 and mRs < 5Craniotomy followed by MMA embolisationCcraniotomy aloneRadiographic recurrence of CSDH within 3 monthsMMAE to Treat CSDHNCT04095819 [98]USATo evaluate the safety and efficacy of a new, less-invasive procedure to treat CSDHOpen-label, pilot RCTUnknown50Patients ≥ 18 years with symptomatic (acute-on) CSDH on imaging and ineligibile for conservative treatmentMMA embolisationSurgical drainage through BHC or craniotomyChange in size of SDH at 6 monthsMiscellaneous trials = 2CSDH-LP; Low intracranial pressure treatment for CSDHNCT04607447 [37]ChinaTo explore the effectiveness and safety of low intracranial pressure treatment strategies for CSDH patientsMulticenter, assessor-blinded RCTRecruitment complete2023160Patients ≥ 14 years with CSDH ineligible for surgical treatmentATO + DXM + low intracranial pressure:1. Supine position for 16 h-18 h daily, head to affected side, 15–20 cm elevation of lower limbs2. Abdominal belt compressionATO + DXMSubdural haematoma volume, MGS, mRS, and Extended Glasgow Outcome score at 3 monthsCraniocervical manual lymphatic massage for CSDHChiCTR2400093100 [24]ChinaTo investigate whether craniocervical manual lymphatic massage can promote haematoma absorption and improve meningeal lymphatic vessel drainage efficiency in conservative treatment of CSDH patientsSingle-center, assessor-blinded RCTJune 202630Patients 18–90 years with CSDH, mRS 1–3, and eligible for conservative treatmentMedical treatment + manual lymphatic drainage five times dailyMedical treatment (ATO 20 mg per dag + DXM placebo 0.75 mg three times daily for 2 weeks, two times daily for 1 week, and once daily for 1 week)Neurological function before admission, at 2 weeks, 4 weeks, and 3 months And function of the meningeal lymphatic vessel before admission and at 2 weeksTrials addressing multiple topics are represented in multiple entries within the tableASA American Society of Anesthesiologists, ATO atorvastatin, BHC burr hole craniostomy, CSDH chronic subdural haematoma, CT computed tomography, DXM dexamethasone, GCS Glasgow Coma Scale, IV intravenous, MGS Markwalder Grading Scale, MLS midline shift, (pre-)mRS (premorbid) modified Rankin Scale, PROBE Prospective Randomised Open, Blinded Endpoint, RCT randomised controlled trial, TXA tranexamic acid
Nearly 50% of recently published trials had a high risk of bias, primarily due to bias in the measurement of the outcome. The lowest risk of bias was observed in trials investigating perioperative management of CSDH. Detailed descriptions of the results from the risk of bias assessment using the RoB 2 tool are provided in the Supplementary Information (Online Resource 1).
Steroid trials
In recent years, five clinical trials investigating corticosteroids have been published, four of which were previously identified in the 2019 review [54, 75, 76, 91, 121]. Among these, dexamethasone emerged as the most extensively studied corticosteroid. These studies hypothesized that corticosteroids may improve outcomes in CSDH through inhibition of inflammation and membrane development [34, 52].
The two largest studies on dexamethasone are the Dex-CSDH and DECSA trials [54, 76]. The Dex-CSDH trial assessed dexamethasone as an adjunct to surgery whilst the DECSA trial compared dexamethasone alone to surgery. Both trials observed that dexamethasone reduced recurrence rates but led to worse functional outcomes, measured on the modified Rankin Scale, and a higher rate of adverse events. The HEMACORT trial evaluated prednisone as an adjunct to surgery and observed a reduction in radiological recurrence as well, but with no clear clinical benefit and increased complication rates [91].
Taken together, these trials do not support the routine use of steroids as either an adjunct or alternative to surgery. At this moment there are three active trials investigating dexamethasone, particularly in combination with atorvastatin [17, 18, 108].
Tranexamic acid trials
Tranexamic acid (TXA) has been hypothesized to reduce CSDH volume due to its anti-fibrinolytic effect [74]. Two recently published RCTs investigated TXA, as an adjunct to surgery, in reducing postoperative CSDH recurrence [128, 133]. Although neither trial showed a significant reduction in reoperation rates, both reported a significant reduction in haematoma volume, consistent with earlier findings in the literature [63, 81]. The lack of effect on reoperation rates, despite reductions in haematoma size, may be attributable to limited statistical power and methodological shortcomings, including high risk of bias of these studies. Consequently, larger trials with robust methodology are still warranted.
At present, seven trials investigating TXA in the context of CSDH are ongoing. Of these, three were identified in the previous review [82, 123, 125], while four are newly initiated [30, 31, 122, 124]. The previously identified trials include two evaluating TXA as stand-alone treatment (TRACS and TORCH) [82, 125], and one assessing TXA as an adjunct to surgery (TRACE) [123].
Among the newly initiated studies, two trials focus on TXA as stand-alone treatment [30, 124], whilst the TRACE-2 trial investigates patient-reported quality of life and CSDH recurrence with TXA either as stand-alone treatment or in combination with surgery [122]. Meanwhile, the TABASCO trial directly compares TXA and MMAE as adjuncts to surgery, aiming to clarify the comparative effectiveness of these two adjunctive strategies [31].
Collectively, these trials demonstrate that the role of TXA in CSDH treatment remains uncertain. Whether it can serve effectively as a stand-alone conservative therapy or as an adjunct to surgical intervention is the subject of continued investigation.
Other pharmacological trials
Atorvastatin is a lipid-lowering agent with proposed anti-inflammatory and angiogenesis-regulating effects [69]. Its effects in the treatment of CSDH were previously investigated in the ATOCH trial, which found a statistically significant, though clinically modest, reduction in haematoma size of 12 mL between the atorvastatin and placebo groups [61]. Two recently published trials have also evaluated the role of atorvastatin in the treatment of CSDH [129, 134]. One trial assessed patients managed conservatively [134], while the other combined atorvastatin with low-dose dexamethasone following surgery [129]. Both studies reported significant reductions in haematoma volume and improvements in neurological outcomes, with the combination therapy demonstrating more pronounced effects. However, findings are of limited value due to small sample sizes and a high risk of bias.
There are ongoing studies assessing atorvastatin as a stand-alone treatment compared to placebo (REACH trial) [101], and again as a post-operative combined therapy with dexamethasone (ATOCH II, ADTCSDH, and ADELE trials) [17, 18, 108]. The REACH and ATOCH II trials, in particular, may have a meaningful impact on clinical practice due to their double-blind design and planned large sample sizes.
Traditional Japanese and Chinese herbal medicines are also under investigation. In Kampo medicine, the traditional herbal medicine in Japan, Goreisan and Saireito are commonly used. Goreisan is known for its hydragogue effect, while Saireito combines both hydragogue and anti-inflammatory properties. Both have been used empirically in the treatment of CSDH [127, 135]. Three completed trials examined Goreisan and/or Saireito, with two reporting no significant reduction in recurrence using Goreisan [45, 133], and the other demonstrating a significant reduction in recurrence with both agents [73]. However, all of these studies are at high risk of bias, primarily due to the absence of blinding or the lack of a placebo control group. Two ongoing trials are exploring traditional Chinese medicine: the CHARM trial evaluating HuoXue LiShui [38] and another trial evaluating the Peiyuan Huayu formula [23], both in conjunction with standard treatment. The CHARM trial [38] appears particularly promising, as it has a placebo-controlled design. HuoXue LiShui is a concept in traditional Chinese medicine which refers to the use of herbal treatments aimed at promoting blood circulation and reducing fluid stasis [132]. The Peiyuan Huayu formula, on the other hand, has demonstrated anti-angiogenic properties, which may be beneficial in managing CSDH [42]. While these herbal therapies may be widely accepted in certain regions, their broader adoption will depend on the reproducibility of findings outside Asia.
Given the high prevalence of antithrombotic use in the CSDH population [46, 66], optimizing antithrombotic therapy in CSDH patients is another key research focus. The recently published SECA trial found no significant increase in recurrence in CSDH patients that continued aspirin as opposed to those that discontinued aspirin [65]. This suggests early resumption of low-dose acetylsalicylic acid, or perhaps its complete continuation, may be possible without negative effects on effective CSDH treatment or recurrence. At present, the RELACS trial is an ongoing study that aims to investigate the optimal postoperative timing for restarting oral anticoagulants in CSDH patients with atrial fibrillation [105].
Taken together, these trials reflect an expanding interest in pharmacological strategies for CSDH across different treatment pathways. Importantly, more ongoing studies are multicenter, with larger sample sizes, and assessor-blinded, often alongside the use of a placebo control. These factors underscore the methodological limitations of earlier single-center and unblinded studies.
Surgical trials
The optimal surgical management of CSDH has long been a subject of debate. While burr hole craniostomy (BHC) is generally considered the gold standard [15, 40, 93, 111], alternative surgical strategies such as craniotomy and twist-drill craniostomy (TDC) remain in clinical use. The COMPACT study [33], which was identified as ongoing in the 2019 review, compared these three operative modalities. Although it did not find a statistically significant difference in outcomes between the treatment arms, BHC was associated with the lowest recurrence rate (7.6% for BHC, 13.1% for craniotomy, And 19.5% for TDC) and a complication profile similar to the other treatment arms. BHC remains the most extensively studied surgical approach in recent years, and there has been additional focus on irrigation, drainage techniques and duration, and surgical cosmesis.
Two large Scandinavian trials (FINISH and SIC!) [11, 100] demonstrated that irrigation at body temperature significantly reduces operative recurrence rates, compared to irrigation at room temperature or no irrigation. An ongoing Japanese trial is currently investigating the use of artificial cerebrospinal fluid for irrigation [62], differing from the irrigation solutions used in the FINISH (saline) and SIC! (Ringer’s lactate) trials.
The method of postoperative drainage has also been investigated, comparing subdural drainage (SDD), the most commonly used technique, with subperiosteal drainage (SPD) [14, 97, 114]. All recent studies found SPD to be a safe and effective alternative to SDD. However, SPD did not meet the predefined non-inferiority margin in the cSDH-Drain-Trial, despite being associated with lower recurrence rates, fewer surgical site infections, and reduced drain misplacement [114]. More definitive conclusions may emerge from the ongoing SUPERDURA trial [2], which compares active SPD with passive SDD. Meanwhile, another ongoing study is evaluating the feasibility of using augmented reality to assist in subdural drain placement, potentially enhancing the safety and precision of standard SDD [87].
The previous review identified the CORRECT-SCAR trial [117], which assessed the use of burr hole covers to improve aesthetic outcomes. The study reported high overall patient satisfaction after BHC, without significant therapy benefit from the use of burr hole covers.
Other new studies have compared single versus double burr hole techniques and found no difference in clinical effectiveness, but a significantly shorter operating time with single burr hole procedures [107, 110]. An ongoing study is examining the efficacy of burr holes drilled in the frontal versus parietal bone, which may affect operative strategy [19].
Perioperative management trials
Two large Danish trials assessed drainage duration following BHC [49, 60]. Shortening drainage time to 6 or 12 h was associated with increased recurrence, whereas no significant difference was observed between 24 and 48 h. These findings support a 24-h drainage period as a safe and efficacious drainage period. The ongoing ECHO trial further explores this topic by comparing exhaustive drainage to a fixed-time protocol, aiming to determine whether more intensive drainage with urokinase injections can reduce recurrence rates [103].
The GET-UP trial, identified in the previous review, demonstrated that early mobilisation (< 12 h after surgery, mean 5.5 h) was associated with fewer complications and lower CSDH recurrence compared to 48 h of bedrest, suggesting a potential shift in postoperative care standards [115].
The choice of anesthetic technique remains a subject of debate, with both general and locoregional anesthesia commonly used in CSDH surgery [1, 130]. The NEURANESTH trial compared these two approaches and found no significant difference in postoperative length of stay until medically fit for discharge, supporting flexibility in anesthetic choice [47]. However, since longer anesthesia durations have been associated with increased 1-year mortality in elderly patients with head injuries, locoregional anesthesia may offer a safer profile [131].
Finally, a novel concept is being evaluated in the BP-CSDH trial, which investigates whether postoperative posture (supine position with elevated lower body), aimed at managing intracranial hypotension, can reduce symptomatic recurrence [36].
Middle meningeal artery embolisation (MMAE) trials
MMAE is an emerging treatment strategy for CSDH that has gained substantial research attention in recent years. While only two ongoing trials on MMAE were identified in the previous review, this number has increased to 21 currently registered and ongoing trials.
In addition to ongoing studies, five RCTs on MMAE have been published in recent years [29, 43, 70, 92, 113]. Notably, three of these – MAGIC-MT, EMBOLISE, and STEM – were simultaneously published in the New England Journal of Medicine in November 2024, prompting significant discussion within the neurosurgical and broader medical communities. All three trials evaluated MMAE as an adjunct to surgical treatment. The MAGIC-MT and STEM trials also included MMAE as a stand-alone treatment.
The MAGIC-MT trial [70], the largest of the three, investigated MMAE using Onyx for embolization. This study reported a reduction in serious adverse events in the embolisation group without significant difference in symptomatic recurrence or haematoma progression within 90 days between the embolisation group and usual-care group (both conservatively and surgically managed CSDH patients).
The EMBOLISE trial [29], also employing Onyx, demonstrated a significant reduction in reoperation rates in the embolisation and operative treatment arm compared to operative treatment alone.
The STEM trial [43] utilized Squid liquid embolization and defined treatment failure as a composite outcome including recurrent or residual CSDH (> 10 mm), reoperation or surgical rescue, disabling stroke, myocardial infarction, or death from a neurologic cause. The trial found that MMAE significantly reduced the risk of treatment failure in the embolisation group compared to the usual-care group (both conservatively and surgically managed CSDH patients). This effect was particularly driven by patients managed non-surgically, although the study was not sufficiently powered to draw definitive conclusions for this subgroup.
Considering these findings, the clinical role of MMAE in the management of CSDH remains uncertain. The variability in results may be due to heterogeneity in patient populations and differences in outcome definitions across studies. The trials have been met with critical responses in the literature, including a recent multidisciplinary consensus statement and several letters to the editor [10, 44, 58]. These critiques highlight methodological concerns and reflect the high risk of bias assessments assigned to these studies in the present review.
Most recently, the EMPROTECT trial [113] investigated MMAE using microparticles rather than non-adhesive liquid agents. The study focused on a CSDH patient population considered at high risk for recurrence. Although the trial observed effect estimates similar to those reported in other recent MMAE studies, it did not demonstrate a statistically significant reduction in recurrence rates at 6 months. It remains uncertain which patient population benefits most from this intervention.
Further research is warranted. The 21 ongoing trials on MMAE explore a range of approaches, including its use as an adjunct to surgery or as a stand-alone treatment. They also compare different embolic materials, such as adhesive and non-adhesive liquid agents, polyvinyl alcohol particles, and cyanoacrylate compounds. Despite variations in design, most of these studies share a common objective: to determine the clinical effectiveness of MMAE in treating CSDH.
Discussion
This review builds upon the 2019 iCORIC systematic review by providing a detailed assessment of recently completed and ongoing RCTs in the field of CSDH. It offers a comprehensive overview of the therapeutic landscape, identifies overlap between studies, and suggests directions for future research to address persistent knowledge gaps. Findings from the RCTs presented in this review are crucial to reduce unwarranted practice variation at both international and intrahospital levels.
The recent publications of clinical practice guidelines in the United Kingdom and Denmark mark a significant milestone in the standardization of CSDH care. Several findings from this review are reflected in those recommendations. Notably, one example is the discouragement of dexamethasone following multiple trials reporting greater harm than benefit of the treatment [54, 76]. This reflects a clear shift from corticosteroids, previously the most studied intervention, to MMAE, which now dominates the research landscape.
This evolving focus suggests a parallel shift in clinical sentiment. Physicians should be less inclined to prescribe dexamethasone and may be more likely to consider MMAE as a potential adjuvant therapy. However, such shifts must be approached with caution. While the discouragement of routine dexamethasone use is supported by several trials, some findings suggest potential benefit in specific patient subgroups [6, 51]. Thus, while dexamethasone should not be part of routine care, further research into its targeted use, or at lower doses, may still hold value. Additionally, other pharmacological alternatives, such as tranexamic acid, are currently under investigation and may also prove beneficial in preventing surgery in vulnerable older patients with CSDH. Given limited resources and competing research priorities, a Value of Information (VOI) analysis [25] may help determine whether future research on the role of corticosteroids in CSDH treatment offers sufficient relevance relative to alternative therapies.
In contrast, MMAE has received increasing attention and is now the most studied intervention for CSDH. Although recent studies suggest that MMAE may be effective, its high resource cost and the limited evidence of clear clinical efficacy argue against its routine implementation in standard practice at this moment. Therefore, it has been proposed that MMAE should only be considered in carefully selected patients [10, 44, 58]. Additionally, the rapid expansion of research in this area raises concerns about potential saturation. Many ongoing studies share similar objectives and designs, which poses a risk of redundancy and inefficient resource use. Greater collaboration among research groups could consolidate efforts into fewer but larger, adequately powered trials.
As with any area of evidence-based medicine, the optimal treatment approach must be individualized to each patient based on the best available data. Continued research in CSDH is vital to expand the evidence base, but this expansion must be strategic. Uncoordinated proliferation of trials poses a risk of compromising overall research quality and diluting clinical impact.
This review has several notable strengths. First, it includes all relevant RCTs, both published and ongoing, providing a comprehensive overview of the current research landscape. By conducting a formal risk of bias assessment, we were able to identify and account for methodological concerns, while also highlighting studies with stronger internal validity and more reliable findings.
Nevertheless, some limitations should be acknowledged. A relatively large portion of included trials carry a high risk of bias, which limits the conclusions we can draw from them. This was especially the case for trials investigating pharmacological agents. This underscores the need for future RCTs to adopt rigorous designs that include placebo controls, power calculations, appropriate outcome selection and blinding where feasible, to enhance internal validity. Furthermore, the risk of publication bias due to trials that were abandoned or never initiated cannot be fully excluded. Thirteen trials were excluded because of unclear or discontinued trial status, as summarized in the Supplementary Information (Online Resource 1). Six trials reported discontinuation, typically for financial or logistical reasons, which would not in themselves introduce publication bias. Most of these involved novel research concepts, limiting their impact on the results summarized in this review. In contrast, seven trials were excluded because their estimated (or actual) completion date was more than three years before our search date, yet no publication or update was available. These trials appear to have been abandoned for unclear reasons, although the absence of registry updates does not necessarily confirm abandonment. To reduce the risk of missing trials for unknown reasons, we attempted to contact principal investigators. However, the lack of response leaves some uncertainty and the possibility of publication bias.
Conclusions
In conclusion, the number of ongoing RCTs in CSDH has increased substantially in recent years, with a noticeable shift in research focus from corticosteroids to MMAE. The growing number of MMAE trials may indicate research saturation, emphasizing the need for consolidation into fewer, larger, and methodologically robust studies. Only through coordinated, high-quality research efforts can the field continue to progress toward optimal, evidence-based, and patient-centred care for individuals with CSDH.
Supplementary Information
Below is the link to the electronic supplementary material.ESM 1Supplementary Material 1 (DOCX 930 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Active 24 Hours Subperiostal vs. 24 Hours Passive Subdural Drainage Following Burr Hole Evacuation of Chronic Subdural Hematoma (the SUPERDURA Trial) - Protocol for a Nationwide Randomized Clinical Non-inferiority Trial (2024) https://clinicaltrials.gov/study/NCT 06621407. Accessed 31 May 2025
- 2Actrn (2021) The role of middle meningeal artery embolisation as post-operative adjunct treatment for chronic subdural haematoma in adult patients. https://www.trialsearchwhoint/Trial 2aspx?Trial ID=ACTRN 12621000263897. Accessed 31 May 2025
- 3Actrn (2021) The role of middle meningeal artery embolisation as primary treatment for chronic subdural haematoma in adult patients. https://www.trialsearchwhoint/Trial 2aspx?Trial ID=ACTRN 12621000202864. Accessed 31 May 2025
- 4Bartek J, Biondi A, Bonhomme V, Castellan L, Catapano G, Cenzato M, Di Nuzzo G, De Robertis E, Giordano F, Iaccarino C, Kulcsar Z, Möhlenbruch MA, Raabe A, Rickard F, Romero CS, Schubert T, D S, Sicignano C, Muto M (2024) Multidisciplinary consensus-based statement on the current role of middle meningeal artery embolization (MMAE) in chronic Sub Dural hematoma (c SDH). Brain Spine 4:10414310.1016/j.bas.2024.104143 PMC 1166406539717364 · doi ↗ · pubmed ↗
- 5Chi Ctr (2025) Middle meningeal artery embolization versus surgery for chronic subdural hematoma: a multicenter, randomized, controlled clinical study in China. https://trialsearch.who.int/Trial 2.aspx?Trial ID=Chi CTR 2500096266
- 6Chi Ctr (2019) The efficacy and safety of combining AT Orvastatin and dexamethasone on Chronic subdural Hematoma: a randomized, double-blind, placebo-controlled trial. https://www.trialsearchwhoint/Trial 2aspx?Trial ID=Chi CTR 1900021659. Accessed 31 May 2025
- 7Chi Ctr (2020) Clinical study of the efficacy and safety of combining atorvastatin and dexamethasone in the treatment of chronic subdural hematoma after drilling and drainage. http://wwww.hoint/trialsearch/Trial 2aspx?Trial ID=Chi CTR 2000030156. Accessed 31 May 2025
- 8Chi Ctr (2020) The efficacy of different skull bore hole sites on the prognosis of chronic subdural hematomas: a randomized controlled trial. https://www.trialsearchwhoint/Trial 2aspx?Trial ID=Chi CTR 2000033967. Accessed 31 May 2025