Imaging Characteristics of Pediatric Renal Cell Carcinoma and Wilms Tumor and Its Impact on Their Management and Outcomes—A Case Report and Review of Literature
Anand Chetan Shah, Prasanth Srinivasan, Shalini Shree Krishnamurthy, Shirley Sunder Singh, Venkatraman Radhakrishnan, Anand Raja

TL;DR
This case report describes a rare pediatric kidney cancer diagnosed through imaging and surgery, highlighting its distinct features and successful treatment.
Contribution
The paper presents a detailed case of translocation-associated RCC in a child, emphasizing imaging's role in diagnosis and management.
Findings
Imaging features like cystic components and calcifications helped avoid biopsy and guide surgery.
Translocation-associated RCC was confirmed through histopathology and immunohistochemistry.
The patient showed no recurrence after 36 months of follow-up following radical nephrectomy.
Abstract
Renal cell carcinoma (RCC) in children is rare, comprising only 1.4–6.3% of pediatric renal tumors. Differentiating RCC from Wilms tumor, the most common pediatric renal tumor is crucial due to differing management and prognosis. Imaging characteristics, such as the presence of calcifications and cystic components, guided the decision to perform surgery without pretreatment biopsy, reducing the risk of needle tract seeding. Translocation-associated RCC is the most common subtype in children, and surgical resection remains the cornerstone of treatment. Long-term follow-up is essential due to the potential for late recurrences. We are reporting the details of a 4-year-old boy, who presented with a 15-day history of fever and abdominal distension, accompanied by a ballotable mass in the right lumbar region. Imaging studies, including a CT scan, revealed a large complex cystic mass in the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
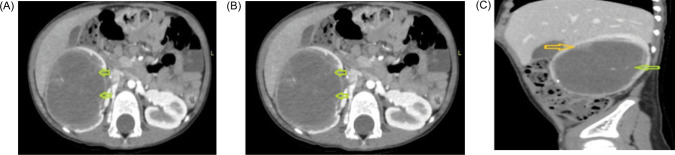 Figure 1
Figure 1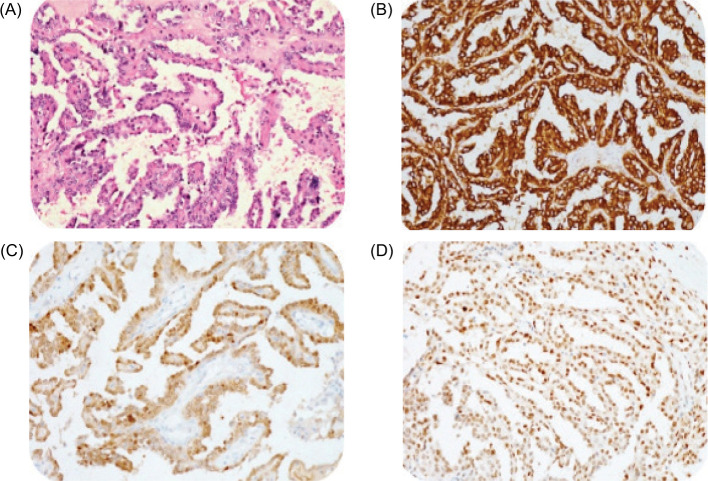 Figure 2
Figure 2| Parameters | Wilms tumor | Renal cell carcinoma | |
|---|---|---|---|
| Age | 1–5 years (peak 3–4 years) | More than 5 years (predominately 2nd decade) | |
| Clinical presentation | Local symptoms | Asymptomatic abdominal mass | Hematuria, abdominal pain and abdominal mass |
| Metastasis | Less frequent presentation with bone metastasis | High chance of metastasis to bone | |
| Radiology | Size | Large mass | Small mass |
| Consistency | Solid but can be cystic | Predominately cystic (more than Wilms) | |
| Calcifications | Less frequent | More frequent | |
| Involvement of nodes | Less frequent | More frequent | |
| Management | Multimodality (surgery and chemotherapy ± radiotherapy) | Surgery (role of chemo, radiotherapy and immunotherapy not clear) | |
| Microscopically | Solid single mass | Hemorrhagic and necrotic areas with calcifications | |
| Prognosis | Stage I | 98.4% | 92.4% |
| Stage II | 97.7% | 84.6% | |
| Stage III | 94.4% | 72.7% | |
| Stage IV | 86.1% | 13.9% | |
| Translocation-associated RCC (Xp11.2) | Papillary or nested architecture with ample acidophilic cytoplasm |
| Papillary RCC (Type 1 and 2) | Single layer of cuboidal cells with scant cytoplasm (type 1) and high – nuclear-grade pseudostratified cells with eosinophilic cytoplasm (Type 2) |
| Clear cell RCC | Clear cytoplasm and cells are arranged in nest with intervening blood vessels |
| Medullary RCC | High-grade epithelial cells with acidophilic cytoplasm arranged in a tubular, often cribriform architecture are occasionally solid or sarcomatoid. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRenal and related cancers · Renal cell carcinoma treatment · Pediatric Urology and Nephrology Studies
Introduction
Childhood renal tumors account for around 7% of all childhood cancers, the commonest being Wilms tumor in the first decade of life (1). Renal cell carcinoma (RCC) is more common than Wilms tumor in the second decade of life (1). Among RCC, translocation-associated RCC (20–40%) is commonest in the pediatric population (2). Factors influencing prognosis include symptomatic presentation, performance status, stage, grade, and histology (3). Surgery forms the mainstay of treatment and results in a cure when the tumor is localized and completely resected (4). We present the case of a child who reported to our institute with a renal mass and was ultimately diagnosed with RCC.
Case Report
A 4-year-old boy presented to our institute with abdominal distension and a fever of 15 day duration. Clinical examination revealed a ballotable mass in the right lumbar region. Routine blood investigations including renal function tests (RFT) were within normal limits. 24-hour
urinary vanillylmandelic acid (VMA) level was 0.4 mg/day (normal: 0–8). A computerized tomography scan (CT) revealed a large single complex cyst of size 8.6 x 6.3 x 6.1cm in the right kidney with enhancing septations, peripheral wall calcifications, and ill-defined soft tissue component within the cyst wall (BOSNIAK category IV) with few enlarged para-aortic nodes (Figure 1). CT scan of the chest was negative for metastasis. The fludeoxyglucose-18 (FDG) positron emission tomography (PET) scan revealed uptake only in the right kidney with no other sites of abnormal metabolic uptake. He underwent a right radical nephrectomy with retroperitoneal lymph node dissection (paracaval, precaval, and interaortocaval). Light microscopy revealed slender papillae with hyalinized fibrovascular cores, papillae lined by a single layer of uniform-looking epithelial cells with hyperchromatic nuclei, psammoma bodies, and necrosis (70%). Mitosis was scanty. Immunohistochemistry (IHC) showed positive reaction to transcription factor E3 (TEF3), keratin, vimentin, cytokeratin (CK-7), cluster of differentiation (CD10), and carbonic anhydrase-9, and negative reaction to alpha-methylacyl coenzyme-A racemase (AMACR), Epithelial membrane antigen (EMA), and variable Paired box gene (PAX-8) (Figure 2). KI-67 was 10–20%. The final histopathology was suggestive of translocation-associated RCC. All nodes were free (0/40). He was staged as pT2aN0. The patient had an uneventful postoperative recovery period and continues to be on regular follow-up with a disease-free survival of 36 months.
Contrast-enhanced CT scan (abdomen and pelvis). (A) Axial noncontrast images, showing a heterodense solid cystic mass in the right kidney, showing the presence of calcifications (yellow arrow). (B) and (C) Axial and sagittal CECT images showing a cystic lesion in the right kidney with thin enhancing internal septations (green arrow) and peripherally placed solid components (yellow arrow).
(A) Papillary structures lined by round to polygonal cells with moderate cytoplasm and vesicular nuclei with nucleoli. H&E 200X. (B) Tumor cells show diffuse positive reaction for cytokeratin. DAB 200X. (C) Tumor cells show a positive reaction for PAX8. DAB 200X. (D) Tumor cells show a positive reaction for TFE3. DAB 200X.
Discussion
Wilms tumor is the most common pediatric renal tumor in the first decade of life (85%) (5). Other common tumors include RCC (1.8–6.3%) (1), clear cell sarcoma, congenital mesoblastic nephroma, malignant rhabdoid tumors, and lymphoma (6). The peak incidence of Wilms tumor occurs around 3 years of age (5), while RCC presents between 9 and 15 years of age (7). RCC accounts for 1.4% of all renal tumors in patients younger than 4 years,15–20% in patients aged 5–9 years, and 52.6% in patients aged 10–15 years (5). Differentiating between RCC and Wilms tumor in children less than 5 years with renal masses is important as the management and prognosis of both conditions vary widely. Clinical, radiological, therapeutic, and prognostic differences between RCC and Wilms tumor are summarized in Table 1. Wilms tumor typically presents as a large, solid, cystic renal mass with infrequent calcifications and less common lymph nodal involvement, whereas RCC tends to be smaller, predominantly cystic, and more frequently associated with calcifications and regional lymphadenopathy (1).
Our patient, a 4-year-old boy presented with a fever and abdominal mass. Differentiation between Wilms tumor and RCC based on imaging criteria is of utmost importance at this age where RCC is rare. Diagnostic imaging revealed calcifications, cystic mass, and enlarged paraaortic nodes. RCC was more likely than Wilms tumor based on imaging characteristics of our index child.
Performing a needle biopsy can clear the diagnostic dilemma, but it comes with the attendant risk of needle tract seedling. This might be of little consequence in Wilms tumor where multimodal treatment would negate the risks of upstaging. This is more so in a case like ours with a large cystic component that can disseminate widely along the biopsy tract. Biopsy also has complications. Vujanic et al. (8) performed a biopsy for all pediatric renal tumors. Serious complications were reported in 182 patients (punch canal metastasis, massive bleeding, and death from tumor rupture).
Given the above considerations, we elected not to perform a biopsy and proceeded with radical nephrectomy with a presumptive diagnosis of RCC. Biopsy and histopathological confirmation is mandated for all patients with metastatic RCC before initiation of systemic therapy. This approach aligns with the treatment strategy for Wilms tumor, where biopsy and preoperative chemotherapy followed by delayed nephrectomy is often a justifiable and standard approach. Postoperative Histopathology was suggestive of translocation-associated RCC.
Renal cell carcinoma is different in adults and children. Clear cell carcinoma is the most common in adults. In the pediatric population, translocation-associated RCC is the commonest (35–50%) (9) followed by papillary RCC, clear cell RCC, and medullary RCC (1). Translocation-associated RCCs typically involve the microphthalmia-associated transcription factor (MiT) family. The most commonly observed fusion partners include transcription factor E3 (TFE3) and transcription factor EB (TFEB), with the corresponding genes located on chromosomes Xp11.2 and 6p21, respectively (1). Nonmetastatic RCC is treated through surgical resection. Light microscopy and IHC characteristics of different types of RCC are summarized in Table 2 (1, 9).
The tumor stage appears to be the most important factor for survival (10). The overall survival of pediatric RCC is about 63%, with survival rates for Stages I–IV at 92.4, 84.6, 72.7, and 13.9%, respectively (11). Little is known about the outcome or the optimal treatment of the different subtypes of childhood RCC (9). Translocation RCC is associated with a risk of lymph nodal metastasis at diagnosis. Studies have reported variable outcomes, with some showing good prognosis despite lymph node metastasis while others showing poor outcomes regardless of the stage (9). Papillary RCC is associated with a disease limited to the kidney in a majority of cases (9). Renal medullary carcinomas typically present with distant metastasis at diagnosis, and survival seldom exceeds a year regardless of adjuvant therapy (12). Most recurrences and deaths in pediatric RCC usually occur within the first 2 years after diagnosis, although late recurrences are frequent (4).
Conclusion
Pediatric renal tumors are not always Wilms tumor. Distinguishing clinical and radiological features enables an appropriate differential diagnosis and influences proper treatment. Pretreatment biopsy can be avoided in RCC based on imaging characteristics. Complete resection of localized disease improves survival. Strict long-term follow-up is required.
Data sharing
The data that support the findings of this study are available from the corresponding author upon reasonable request.
All procedures performed in studies involving human participants were per the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from the participant included in the study.
This research was exempt from the Institutional Review Board or Ethics Committee as it is an isolated case report and patient consent has been obtained.
The participant was informed about the purpose of the study, the procedures involved, and their right to withdraw at any time without any consequences.
The confidentiality and anonymity of the participant were ensured throughout the study.
Author Contributions
Anand Chetan Shah: Conceptualization, Writing and editing; Prasanth Srinivasan: Conceptualization, Writing and editing; Shalini Shree Krishnamurthy: Conceptualization; Shirley Sunder Singh: Resources and Supervision; Venkatraman Radhakrishnan: Resources and Supervision; Anand Raja: Resources and Supervision, Final approval.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chung EM, Lattin GE Jr, Fagen KE, Kim AM, Pavio MA, Fehringer AJ. Renal tumors of childhood: Radiologic–pathologic correlation Part 2. The 2nd Decade 1. 10.1148/rg.2017160189 PMC 562172928898190 · doi ↗ · pubmed ↗
- 2Eble JN, Sauter G, Epstein JI, Sesterhenn IA. World Health Organization classification of tumours; Pathology and genetics of tumours of the urinary system and male genital organs. Lyon: IARC Press; 2004.
- 3Kontak JA, Campbell SC. Prognostic factors in renal cell carcinoma. Urol Clin North Am. 2003;30:467–80. 10.1016/S 0094-0143(03)00020-X 12953749 · doi ↗ · pubmed ↗
- 4Indolfi P, Terenziani M, Casale F, Carli M, Bisogno G, Schiavetti A, et al. Renal cell carcinoma in children: A clinicopathologic study. J Clin Oncol. 2003;21(3):530–5. 10.1200/JCO.2003.02.07212560445 · doi ↗ · pubmed ↗
- 5Uchiyama M, Iwafuchi M, Yagi M, Iinuma Y, Ohtaki M, Tomita Y, et al. Treatment of childhood renal cell carcinoma with lymph node metastasis: Two cases and a review of literature. J Surg Oncol. 2000;75(4):266–9. 10.1002/1096-9098(200012)75:4<266::aid-jso 8>3.0.co;2-h 11135269 · doi ↗ · pubmed ↗
- 6Lowe LH, Isuani BH, Heller RM, Stein SM, Johnson JE, Navarro OM, et al. Pediatric renal masses: Wilms tumor and beyond. 2000;20(6):1585–603. 10.1148/radiographics.20.6.g 00nv 05158511112813 · doi ↗ · pubmed ↗
- 7Geller JI, Dome JS. Local lymph node involvement does not predict poor outcome in pediatric renal cell carcinoma. Cancer. 2004;101(7):1575–83. 10.1002/cncr.2054815378495 · doi ↗ · pubmed ↗
- 8Vujanic GM, Kelsey A, Mitchell C, Shannon RS, Gornall P. The role of biopsy in the diagnosis of renal tumors of childhood: Results of the UKCCSG Wilms tumor study 3. Med Pediatr Oncol. 2003;40:18–22. 10.1002/mpo.1021612426681 · doi ↗ · pubmed ↗