Endoscopic ultrasound-guided coil embolization combined with cyanoacrylate injection into perforating vein for gastric varices
Jun Li, Yingqun Zhou, Junshan Wang, Jiao Feng, Feng Liu

Abstract
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1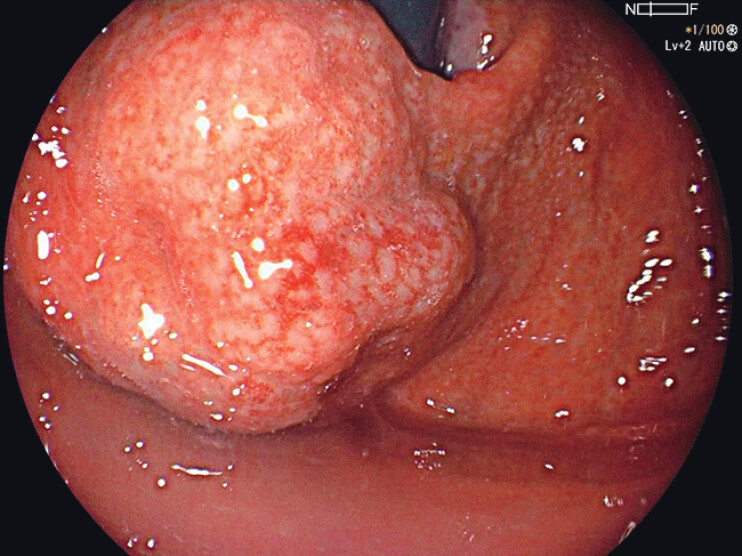 Fig. 2
Fig. 2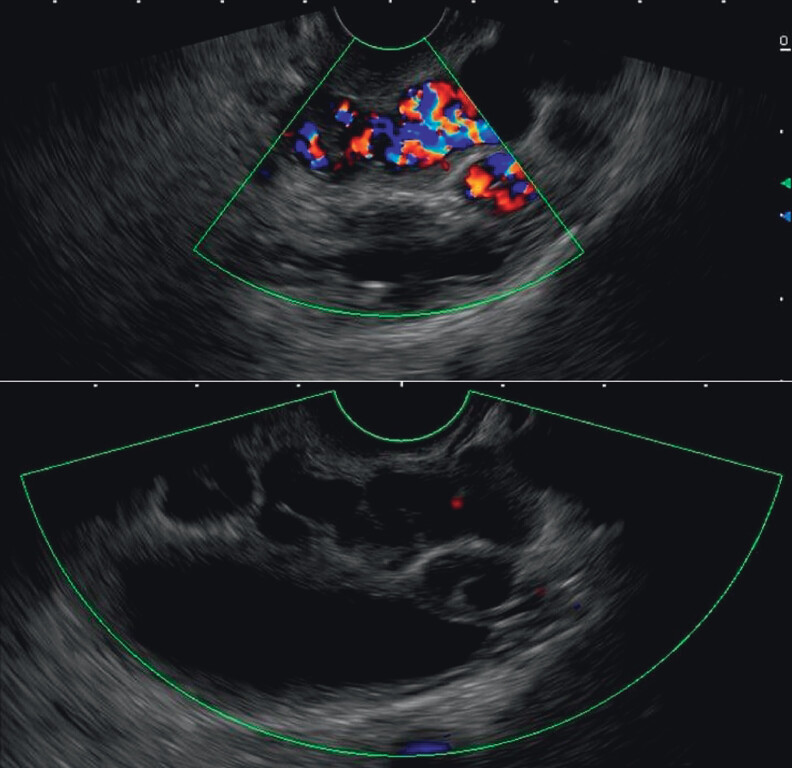 Fig. 3
Fig. 3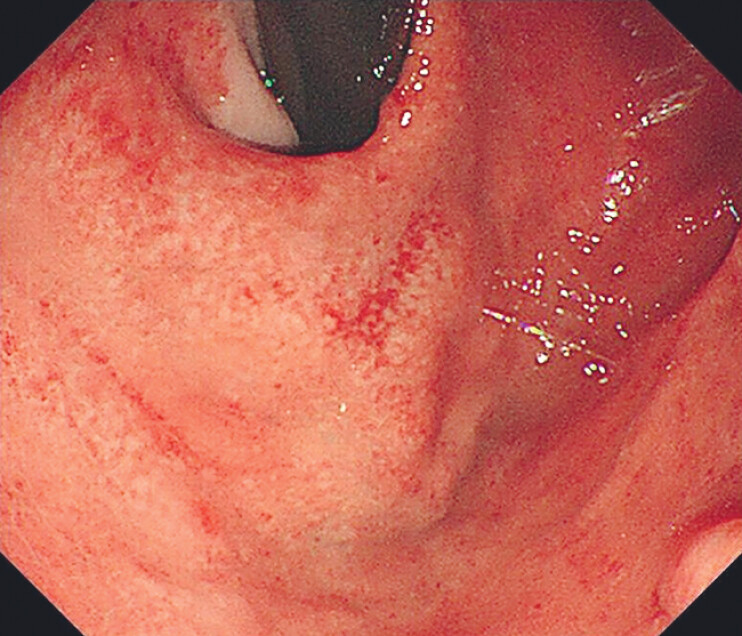 Fig. 4
Fig. 4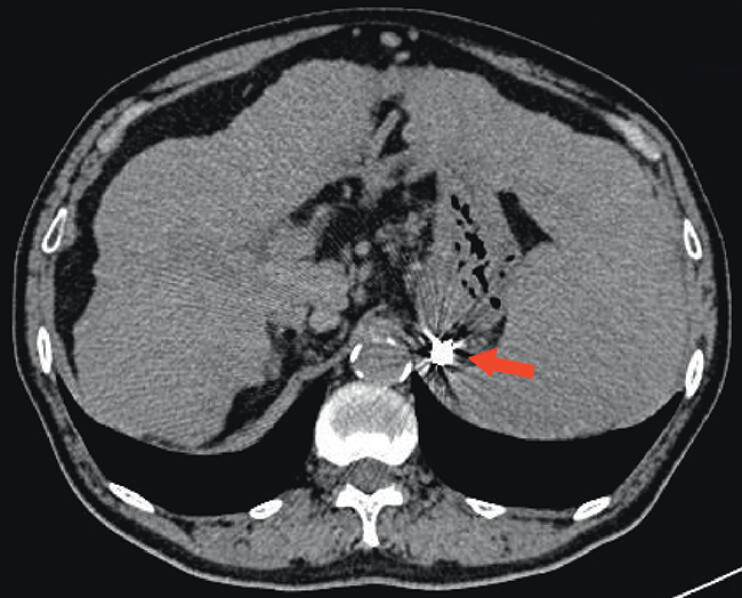 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLiver Disease and Transplantation · Gastrointestinal Bleeding Diagnosis and Treatment · Diagnosis and Treatment of Venous Diseases
Gastric varices (GVs) secondary to portal hypertension pose a significant risk of life-threatening hemorrhage. While endoscopic cyanoacrylate (CYA) injection is widely used, it carries risks of embolization, rebleeding, and local complications. Endoscopic ultrasound (EUS) offers precise visualization of variceal architecture, including feeding perforating veins, enabling targeted therapy. EUS-guided interventions could minimize glue volume and reduce adverse events by directly occluding perforators.
A 62-year-old man with a history of alcohol-related cirrhosis, splenomegaly, and portal hypertension was found to have gastroesophageal varices along with portosystemic collateral vessels, as demonstrated on CT angiography ( Fig. 1 ). Endoscopy showed significantly bulged GVs in the gastric fundus measuring about 3.0 cm in diameter ( Fig. 2 ). Under general anesthesia, a linear EUS scope identified perforating veins supplying the varices ( Video 1 ). Under real-time EUS guidance, a 22-G needle punctured the perforator, deploying a 10 cm × 30 mm coil followed by 1 mL CYA injection. Real-time Doppler confirmed complete blood flow cessation ( Fig. 3 , Video 1 ). Postprocedure endoscopy showed marked varix collapse ( Fig. 4 ). An abdominal CT performed 24 hours after the procedure showed that the coils and CYA glue remained in situ ( Fig. 5 ). The patient was discharged after 48 hours without complications and remained stable at follow-ups.
CT angiography showed cirrhosis, splenomegaly, and portal hypertension with gastroesophageal varices and portosystemic collateral vessels.
Gastroscopy showed bulged gastric varices along the greater curvature of the fundus.
EUS-guided coil embolization combined with cyanoacrylate injection into perforating vein for gastric varices.Video 1
Real-time Doppler showed blood flow signals before (upper) and after (lower) the procedure.
Gastroscopy after the procedure showed a significantly collapsed varix.
Postprocedure CT showed the coils and cyanoacrylate glue remained in situ.
This is the first reported case of EUS-guided coil embolization combined with CYA injection into a perforating vein for GV treatment. Unlike prior studies describing EUS-guided CYA alone 1 2 3 , this combined approach leverages coils as a scaffold to retain glue, minimizing migration risk and reducing required CYA volume. EUS-guided coil and CYA injection into perforating veins represents a promising, accurate technique for GV obliteration, potentially optimizing outcomes by enhancing precision and reducing glue-related risks.
Endoscopy_UCTN_Code_TTT_1AS_2AB Endoscopy_UCTN_Code_TTT_1AO_2AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Romero-Castro R Pellicer-Bautista FJ Jimenez-Saenz MEUS-guided injection of cyanoacrylate in perforating feeding veins in gastric varices: results in 5 cases Gastrointest Endosc 20076640240710.1016/j.gie.2007.03.00817643723 · doi ↗ · pubmed ↗
- 2Sabry F Seif S Eldesoky AEUS-guided cyanoacrylate injection into the perforating vein versus direct endoscopic injection in the treatment of gastric varices Endosc Int Open 202311 E 202E 21036845270 10.1055/a-1984-7070 PMC 9949986 · doi ↗ · pubmed ↗
- 3Altonbary AY Sabry F Hakim H Endoscopic ultrasound-guided cyanoacrylate injection into the perforating vein for high-risk gastric varices Endoscopy 202456 E 516E 51738866061 10.1055/a-2333-9436 PMC 11168792 · doi ↗ · pubmed ↗