Hybrid side-by-side and stent-in-stent deployment of three slim multi-hole metallic stents for malignant hilar biliary obstruction
Soma Fukuda, Masato Endo, Yusuke Niisato, Yuya Hagiwara, Hirotaka Uno, Taku Sakamoto, Kiichiro Tsuchiya

Abstract
Click any figure to enlarge with its caption.
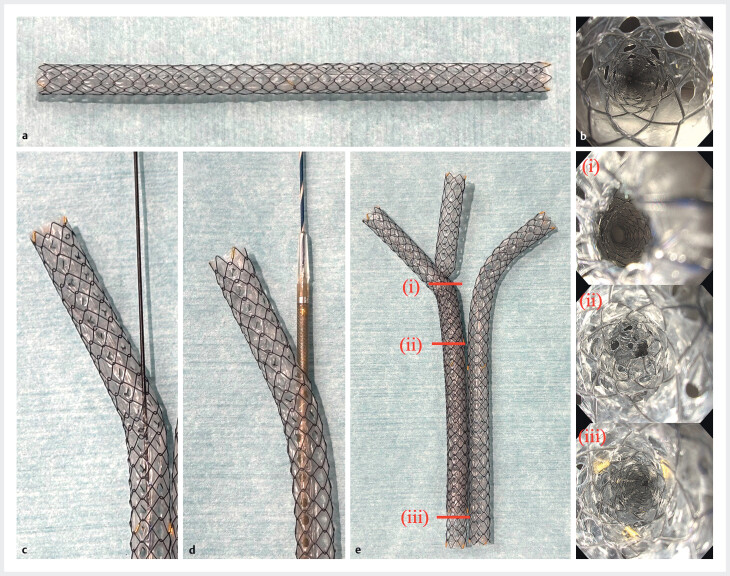 Fig. 1
Fig. 1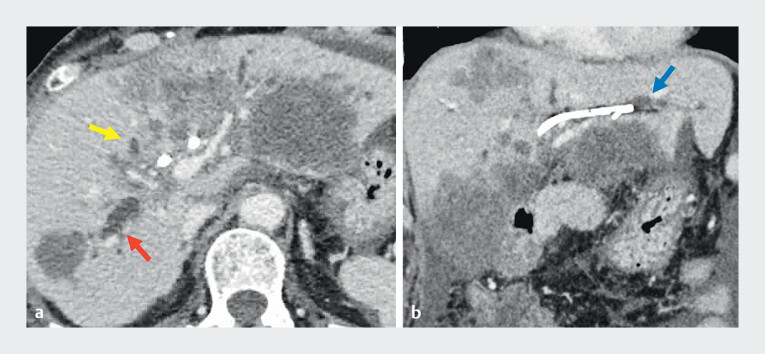 Fig. 2
Fig. 2 Fig. 3
Fig. 3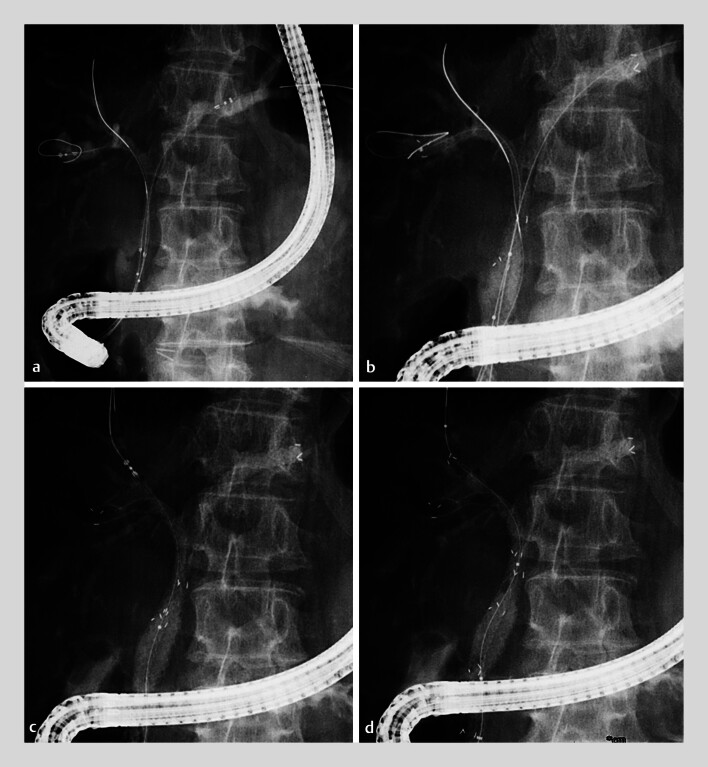 Fig. 4
Fig. 4 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Cholangiocarcinoma and Gallbladder Cancer Studies · Esophageal and GI Pathology
Malignant hilar biliary obstruction (MHBO), especially Bismuth types III and IV, often requires trisegment drainage. Triple uncovered self-expandable metal stent (UCSEMS) placement with the stent-in-stent (SIS) method has been reported but is technically demanding 1 . A hybrid side-by-side (SBS) plus SIS approach has also been described, yet tumor ingrowth remains problematic with UCSEMSs 2 3 . Recently, slim 6-mm multi-hole SEMSs (MHSEMSs) (HANAROSTENT Biliary Multi-Hole Benefit; M.I. Tech Co., Ltd., Pyeongtaek, South Korea) featuring 1.5-mm side holes along the circumference have been introduced ( Fig. 1 ). These stents have been applied for SBS and SIS 4 5 . However, trisegment drainage with MHSEMSs remains technically challenging. We present the first case of trisegment drainage using a hybrid method with three slim MHSEMSs.
a The 6-mm slim multi-hole SEMS (MHSEMS), which is covered and equipped with multiple 1.5-mm side holes arranged along the circumference. b Endoscopic view of the stent lumen. c A guidewire passing through a side hole of the stent. d A 5.9-Fr delivery sheath advanced through a side hole. e Hybrid method (side-by-side and stent-in-stent) using three slim MHSEMSs. (i–iii) Endoscopic views of the stent lumen after stent-in-stent deployment.
A 65-year-old woman with cecal cancer and liver metastasis developed cholangitis after plastic stents had been placed in the left hepatic duct and right anterior branch. Imaging showed disease progression with occlusion of these stents and new dilatation of the isolated right posterior branch ( Fig. 2 ). Because trisegment drainage was required, endoscopic drainage with three 6-mm MHSEMSs was performed.
Contrast-enhanced CT showing progression of liver metastases with intrahepatic bile duct dilatation (yellow arrow, right anterior branch; red arrow, right posterior branch; blue arrow, left hepatic duct). a Axial view. b Coronal view.
After stent removal, guidewires were placed in the left, right anterior, and right posterior ducts ( Fig. 3 ). Two MHSEMSs were deployed simultaneously in the left and right posterior ducts using the SBS technique. A guidewire was successfully advanced into the right anterior branch through a small side hole, enabling SIS placement of the third MHSEMS ( Fig. 4 , Video 1 ). Final cholangiography confirmed successful trisegment drainage without adverse events ( Fig. 5 ).
ERCP demonstrating a Bismuth type IV hilar stricture with isolated left hepatic duct, right anterior, and right posterior branches.
Hybrid deployment procedure. a Two delivery systems positioned in the left hepatic duct and right posterior branch. b Simultaneous deployment of two MHSEMSs using the side-by-side (SBS) technique. c Positioning of the third MHSEMS delivery system through a side hole of the posterior stent. d Deployment of the third MHSEMS using the stent-in-stent (SIS) technique.
Hybrid side-by-side plus stent-in-stent deployment of three slim multi-hole SEMSs demonstrates an effective option for malignant hilar obstruction requiring trisegment drainage.Video 1
Completion of hybrid SBS and SIS deployment of three slim MHSEMSs with good contrast drainage.
This case highlights successful trisegment drainage using a hybrid method with three slim MHSEMSs. The multi-hole design allowed guidewire passage and branch drainage, while the slim delivery system enabled simultaneous SBS deployment. Compared with plastic stents, longer patency is expected, and UCSEMS-related ingrowth risk may be reduced. This hybrid approach offers a technically easier and effective option for malignant hilar obstruction requiring trisegment drainage.
Endoscopy_UCTN_Code_TTT_1AR_2AZ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Takeshita K Hijioka S Ikezawa K Uncovered Self-Expandable Metallic Stent with an Ultra-Thin Delivery Sheath in Unresectable Malignant Hilar Biliary Obstruction: A Multicenter Prospective Observational Study Dig Dis Sci 2025701560157239971830 10.1007/s 10620-025-08898-z PMC 11972213 · doi ↗ · pubmed ↗
- 2Ogura T Yamada M Ueno S Hybrid placement technique for hepatic hilar obstruction using a new uncovered self-expandable metal stent Endosc Int Open 20197 E 1288 E 129210.1055/a-0998-784731579711 PMC 6773583 · doi ↗ · pubmed ↗
- 3Maruki Y Hijioka S Wu SYS Novel endoscopic technique for trisegment drainage in patients with unresectable hilar malignant biliary strictures (with video)Gastrointest Endosc 20209276376932169434 10.1016/j.gie.2020.03.003 · doi ↗ · pubmed ↗
- 4Takahashi S Fujisawa T Takasaki Y Side-by-side placement of a novel slim 6-mm multi-hole covered self-expandable metallic stent for malignant hilar biliary obstruction Endoscopy 202557 E 312E 31310.1055/a-2569-758240233932 PMC 12020676 · doi ↗ · pubmed ↗
- 5Ogura T Uba Y Kanadani T Stent-in-stent deployment for malignant hilar obstruction using multi-hole stent can prevent tumor ingrowth during 6-month cholangioscopic follow-up Endoscopy 202557 E 99E 10039909411 10.1055/a-2518-5430 PMC 11798663 · doi ↗ · pubmed ↗