Wound closure after endoscopic submucosal dissection of the colon using a novel detachable traction device: a rubber ring with a figure-of-eight sliding knot
Jinpo Wang, Yunxin Chen, Miao Liu, Xiaoxiong Guo, Mingkai Zhuang, Zihan Chen, Fenglin Chen

Abstract
Click any figure to enlarge with its caption.
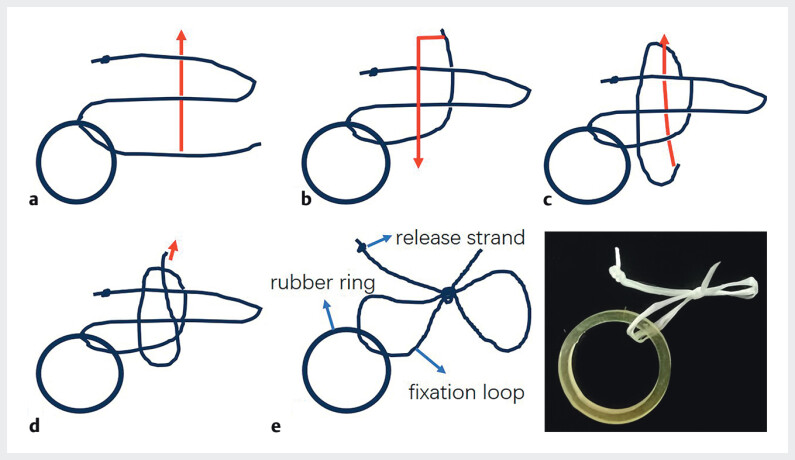 Fig. 1
Fig. 1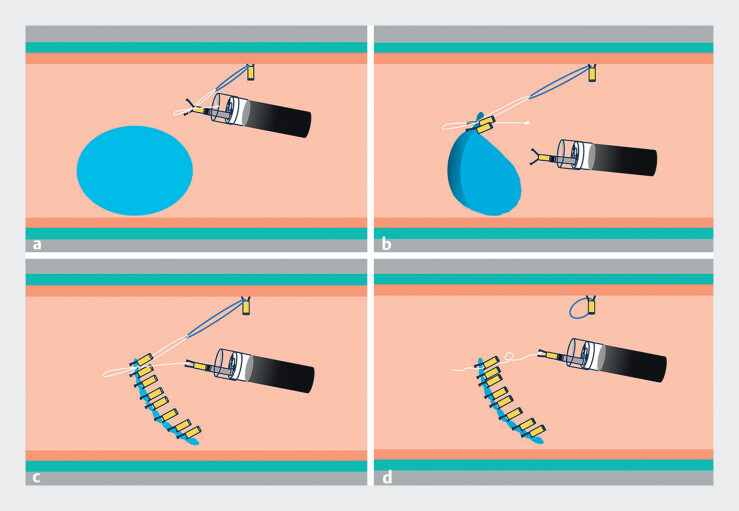 Fig. 2
Fig. 2- —National Key Clinical Specialty Construction Projects of Fujian Province, China
- —Fujian Clinical Research Center for Digestive System Tumors and Upper Gastrointestinal Diseases
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Esophageal and GI Pathology · Enhanced Recovery After Surgery
Closure of post-endoscopic submucosal dissection (ESD) defects in the intestine remains challenging, often being time-consuming and incomplete. Previous studies reported a complete closure rate of only 76% following colorectal ESD 1 , with a pooled mean suturing time of 31.11 minutes 2 . Therefore, improved techniques for intestinal ESD wound closure are still being actively explored. Our team previously introduced the pre-placement sharp angle traction (PPSAT) method to assist ESD for colorectal laterally spreading tumors (LSTs) 3 . Building on this technique, we developed a novel device named SureLoop ( Fig. 1 ), which combines a rubber ring and a figure-of-eight sliding knot to facilitate both resection and wound closure ( Video 1 ).
How to tie a “SureLoop” with floss and a rubber ring. a Create a loop by passing the end of the thread through from the back down. b Move it from the front to the lower left. c Pass it through the top left loop from the back. d Finally, tighten the thread at the end and the top of the lower left loop. e . Completed.
The novel SureLoop traction device was utilized to facilitate traction-assisted dissection and subsequent wound closure.Video 1
An LST measuring approximately 20 mm × 25 mm was identified in the rectum. After submucosal injection and circumferential incision, the SureLoop was anchored at an optimal position opposite to the lesion. The rubber ring was fixed on the anal side of the lesion using a clip, enabling effective traction via PPSAT technique to facilitate en bloc resection ( Fig. 2 a ). The fixation loop of the figure-of-eight knot was then clipped to one edge of the wound and pulled diagonally toward the opposite side, achieving sequential button-type closure ( Fig. 2 b ). After successful closure, the release strand of the knot was pulled with a clip or forceps to loosen and remove the knot ( Fig. 2 c, d ). Notably, a single rubber ring can accommodate two or more figure-of-eight knots if needed.
Schematic description of the strategy. a The SureLoop's rubber band is anchored at an appropriate distance and direction diagonally opposite to the lesion. An additional clip is used to secure the fixation knot of the figure-of-eight ligature on one side of the wound. b The wound edge is grasped and pulled toward the diagonally opposite side, facilitating easier, more precise, and rapid wound closure. c After complete wound closure, the release strand of the figure-of-eight ligature is engaged and gently pulled using a clip or forceps to undo the knot. d Successful wound closure is achieved. And the clip that loosens the knot can be repurposed to strengthen the wound.
During colorectal ESD, parallel alignment between the endoscope and the colon wall often complicates clip placement. The SureLoop device facilitates effective traction toward the anal side, reorienting the wound to face the endoscope directly, thereby simplifying the closure process, improving accuracy, and reducing both procedure time and number of clips required. We believe this device holds significant clinical promise, though prospective studies are warranted to validate its efficacy.
Endoscopy_UCTN_Code_TTT_1AQ_2AB
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nomura S Shimura T Katano TA multicenter, single-blind randomized controlled trial of endoscopic clipping closure for preventing coagulation syndrome after colorectal endoscopic submucosal dissection Gastrointest Endosc 202091859867010.1016/j.gie.2019.11.03031785275 · doi ↗ · pubmed ↗
- 2Niu C Zhang J Farooq U Endoscopic suturing for mucosal defect closure following endoscopic submucosal dissection: Systematic review and meta-analysis Endosc Int Open 202412 E 1150 E 115910.1055/a-2411-872439398447 PMC 11469170 · doi ↗ · pubmed ↗
- 3Wang J Chen Y Liu M Pre-placement sharp angle traction-assisted endoscopic submucosal dissection for the treatment of laterally spreading tumors of the colon Endoscopy 202557 E 927E 92810.1055/a-2667-737740834892 PMC 12367407 · doi ↗ · pubmed ↗