Endoscopic resection of a giant duodenal lipoma: a case report
Ângela Domingues, Ricardo Araújo, Gonçalo Silva, Rita Sousa, Carlos Saraiva, Nuno Dias, Américo Silva

Abstract
Click any figure to enlarge with its caption.
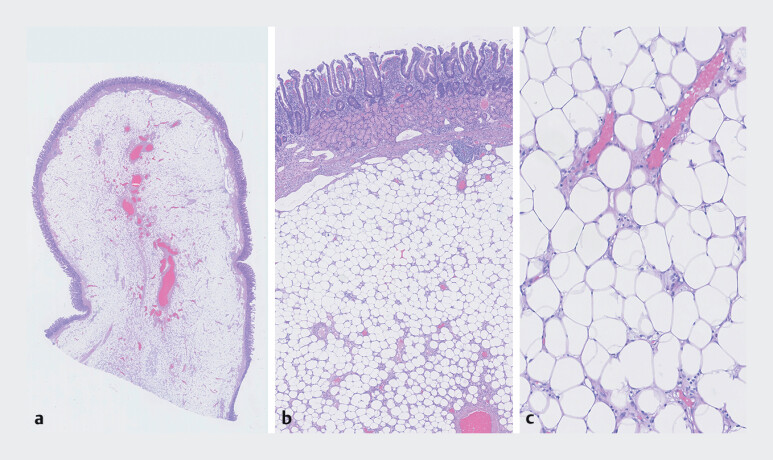 Fig. 1
Fig. 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Gastrointestinal Tumor Research and Treatment · Tumors and Oncological Cases
59-year-old male patient underwent a screening endoscopy requested by his primary care physician, during which a duodenal lesion was identified.
The patient reported pain in the left upper quadrant.
Upper gastrointestinal endoscopy revealed a thick, finger-like polypoid lesion, originating from the proximal second portion of the duodenum (D2) and extending into the third portion (D3), with an approximate length of 10 cm.
EUS identified a duodenal lesion involving mucosa and submucosa, with retraction of the muscular layer in the proximal 2 cm.
Axial contrast-enhanced CT images showing an endophytic polypoid lesion in the second portion of the duodenum, with a central adipose and vascular component, extending toward the ligament of Treitz ( Video 1 ). Endoscopic ressection was performed, as demonstrated in the main video. Pathological examination reveald a duodenal lipoma ( Fig. 1 ).
Axial contrast-enhanced CT images showing an endophytic polypoid lesion in the second portion of the duodenum, with a central adipose and vascular component, extending toward the ligament of Treitz.Video 1
Duodenal mucosal and submucosal specimen without evidence of epithelial dysplasia, containing a submucosal lesion histologically consistent with a LIPOMA. a Polypoid submucosal lesion, low magnification. b Adipocytic proliferation in the duodenal submucosa (small intestinal mucosa with Brunner’s glands). c Mature unilocular adipocytes without easily identifiable lipoblasts or atypical stromal cells.
Lipomatous lesions of the gastrointestinal tract are rare and those of the duodenum are extremely unusual.
The majority is found incidentally, however, large duodenal lipomas may present with clinical symptoms such as abdominal pain, dyspepsia, intussusception and rarely, GI haemorrhage and iron deficiency anaemia.
The current recommendation is endoscopic excision, unless this is technically difficult and warrants surgical excision.
We present a rare case of giant lipomatous duodenal lesion, successfully treated with endoscopy.
Endoscopy_UCTN_Code_TTT_1AO_2AC
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Strnisa L Plut S Golob S Endoscopic resection of a large symptomatic duodenal lipoma Gastroenterol Hepatol 20244738438610.1016/j.gastrohep.2023.03.00436965578 · doi ↗ · pubmed ↗
- 2Thorlacius H, Weiber H., Ljungberg O. Endoscopic diagnosis and treatment of a giant duodenal lipoma presenting with gastrointestinal bleeding Endoscopy 20134538538610.1055/s-0033-134482524285061 · doi ↗ · pubmed ↗
- 3Lee KJ., Kim G.H., Park do Y. Endoscopic resection of gastrointestinal lipomas: a single-center experience Surg Endosc 20142818519210.1007/s 00464-013-3151-923996333 · doi ↗ · pubmed ↗