A novel closure technique for a mucosal defect after endoscopic submucosal dissection: “closure on traction using a rotatable clip with a line loop”
Yorinari Ochiai, Minoru Oda, Junji Tanaka, Yusuke Kawai, Hiroshi Yamato, Yugo Suzuki, Shu Hoteya

Abstract
Click any figure to enlarge with its caption.
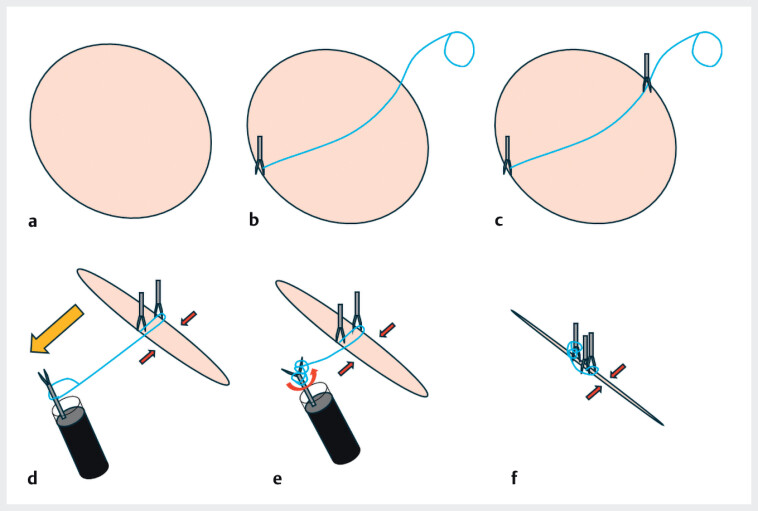 Fig. 1
Fig. 1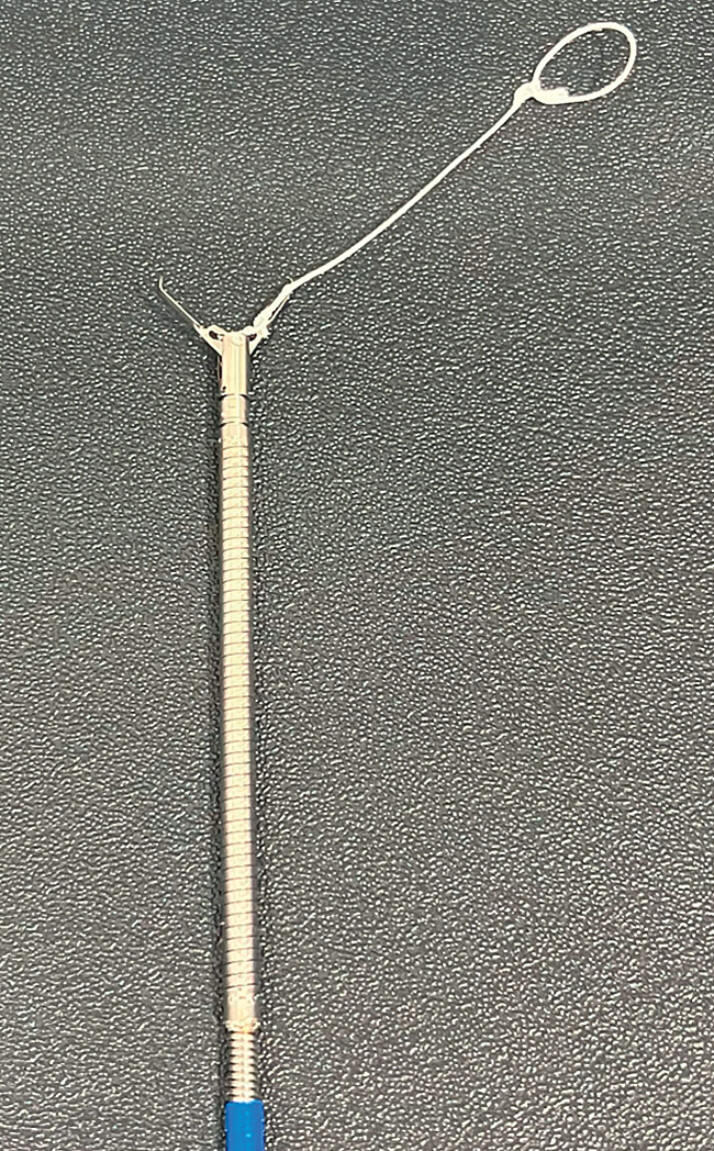 Fig. 2
Fig. 2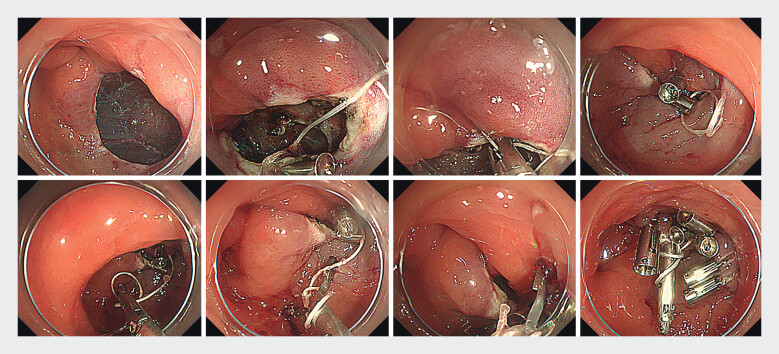 Fig. 3
Fig. 3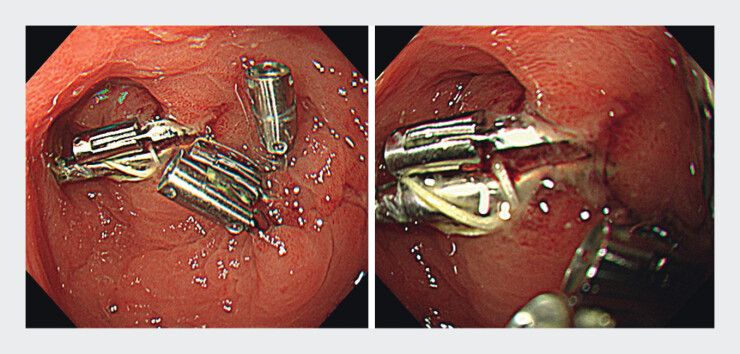 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Esophageal Cancer Research and Treatment · Esophageal and GI Pathology
Endoscopic submucosal dissection (ESD) is widely performed for early gastrointestinal tumors; however, delayed bleeding is a major complication, reported in 5–10% of cases 1 . Various closure methods after ESD may reduce delayed bleeding 2 3 .
We have developed and used a novel closure technique named “closure on traction using a rotatable clip with a line loop (CONTROLL)” to treat a mucosal defect after ESD ( Fig. 1 ), using only rotatable clips and a line loop completed in the lumen, without scope reinsertion.
Schematic of the closure on traction using a rotatable clip with a line loop (CONTROLL) technique. a A post-endoscopic submucosal dissection ulcer defect. b First rotatable clip with a line loop placed at one side of the ulcer edge. c Second rotatable clip placed on the other side of the ulcer, including the line. d The third clip passed through the loop and moved to the first clip side for traction. e The opened third clip rotated to wrap the line around the clip. f By rotating the third clip, the line was shortened, resulting in a mucosa–mucosa traction, and the third clip was placed easily near the first and second clips.
A 71-year-old man underwent ESD for an early gastric cancer on the posterior side of the greater curvature of the antrum. Mucosal defect closure for an approximately 25-mm post-ESD ulcer was performed using CONTROLL. Before the procedure, a clip with a line with a 5–10-mm loop was set to a length approximately of 5-10 mm longer than the ulcer size ( Fig. 2 ). The first clip (SureClip; Micro-Tech Co., Ltd, Nanjing, China) with a line loop (polyester suture; Shirakawa Co., Ltd, Tokyo, Japan) was placed on one edge of the ulcer, including the muscular layer. A second clip (SureClip) grasping a line was deployed on the other side, including the muscular layer. A closed third clip (MANTIS Clip; Boston Scientific Corporation, Marlborough, MA, USA) was passed through the loop and moved to the side of the first clip. The third clip was opened and rotated to wrap a line around it. The edges of the ulcer simultaneously came close to the traction by shortening the line, and the third clip was placed near the first and second clips ( Fig. 3 and Video 1 ). Additional clips reinforced the defects. A follow-up endoscopy performed 3 days after the procedure showed no ulcer dehiscence ( Fig. 4 ).
First clip with a line loop. Making a 5–10-mm loop and setting the length of the line as approximately 5-10 mm longer than the ulcer size. We used SureClip; (Micro-Tech Co., Ltd, Nanjing, China) and polyester suture (Shirakawa Co.,Ltd, Tokyo, Japan) in this case.
Endoscopic images of closure on traction using a rotatable clip with a line loop (CONTROLL) technique for endoscopic submucosal dissection ulcer defect.
A case of closure on traction using a rotatable clip with a line loop (CONTROLL) technique for a post-endoscopic submucosal dissection ulcer defect.Video 1
Endoscopic images 3 days after closure on traction using a rotatable clip with a line loop (CONTROLL) technique.
CONTROLL enabled firm closure. The clip–line and clip–clip connections become stronger by rotating the clip and shortening the line.
Endoscopy_UCTN_Code_TTT_1AQ_2AB
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pimentel-Nunes P Libânio D Bastiaansen BAJ Endoscopic submucosal dissection for superficial gastrointestinal lesions: European Society of Gastrointestinal Endoscopy (ESGE) Guideline – Update 2022 Endoscopy 20225459162210.1055/a-1811-702535523224 · doi ↗ · pubmed ↗
- 2Gong R Wang S Song J Closure methods for large defects after gastrointestinal endoscopic submucosal dissection J Gastroenterol Hepatol 2024392511252110.1111/jgh.1672239175260 PMC 11660212 · doi ↗ · pubmed ↗
- 3Sugimoto S Nomura T Temma T Closure of gastric mucosal defects using the reopenable-clip over-the-line method to decrease the risk of bleeding after endoscopic submucosal dissection: a multicenter propensity score-matched case-control study (with video)Gastrointestinal Endoscopy 2025102374639542223 10.1016/j.gie.2024.11.015 · doi ↗ · pubmed ↗