Approach to Diagnosis and Management of Polycystic Ovary Syndrome in Bangladesh: A Nationwide Cross-Sectional Survey of Physicians
Marufa Mustari, Ahmed Ifrad Bin Raunak, Samira Mahjabeen, Syed Azmal Mahmood, Faria Afsana, M Saifuddin, Tahniyah Haq, Sunjida Islam, Tanjina Hossain, S M Mohiuddin, Nazma Akter, Afsar Ahammed, Rezwana Sobhan, Shahin Ibn Rahman, Sourav Sarkar, Md. Faruque Pathan

TL;DR
This study examines how doctors in Bangladesh diagnose and treat PCOS, finding that most follow international guidelines but with inconsistencies in practice.
Contribution
The study provides insights into physician practices and adherence to guidelines for PCOS management in Bangladesh, highlighting the need for a unified national guideline.
Findings
Most physicians (89.1%) reported applying at least one recognized PCOS guideline.
Lifestyle modifications and metformin were the most common treatment strategies.
A majority of participants supported establishing a structured referral system for PCOS care.
Abstract
Background: Polycystic ovary syndrome (PCOS) is the most prevalent endocrine disorder among women of reproductive age. This nationwide cross-sectional study aimed to assess physicians' diagnostic and management practices for PCOS in Bangladesh, with a particular focus on adherence to established guidelines. Methods: This nationwide cross-sectional survey was conducted between April and October 2024 among general practitioners and specialists using a semi-structured questionnaire. Information on demographic characteristics, diagnostic and therapeutic practice patterns, and use of clinical guidelines was collected. Descriptive statistical methods were applied. Results: Among the 643 practicing physicians, 553 (86%) were specialists in Gynecology and Obstetrics, followed by general practitioners (7.8%), endocrinologists (4%), and others. The European Society for Human Reproduction and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
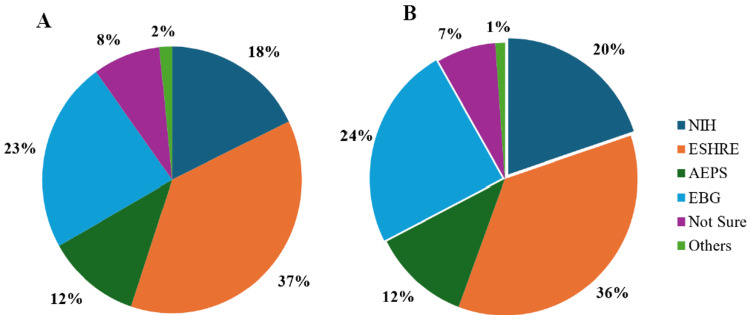 Figure 1
Figure 1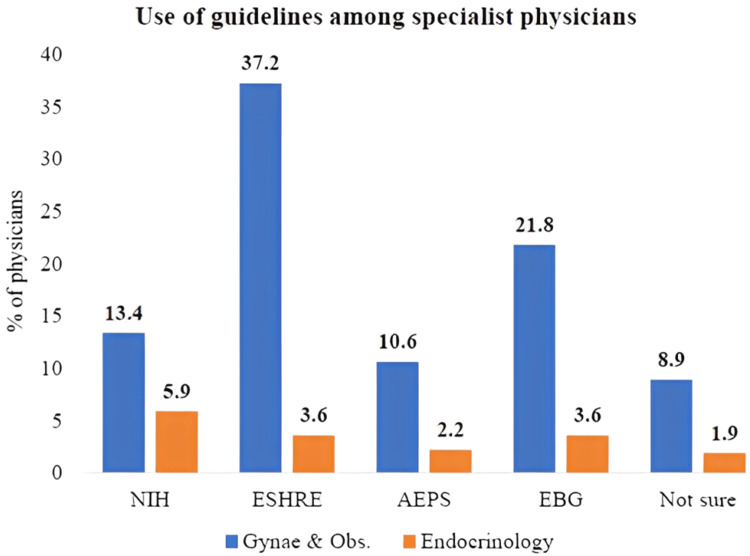 Figure 2
Figure 2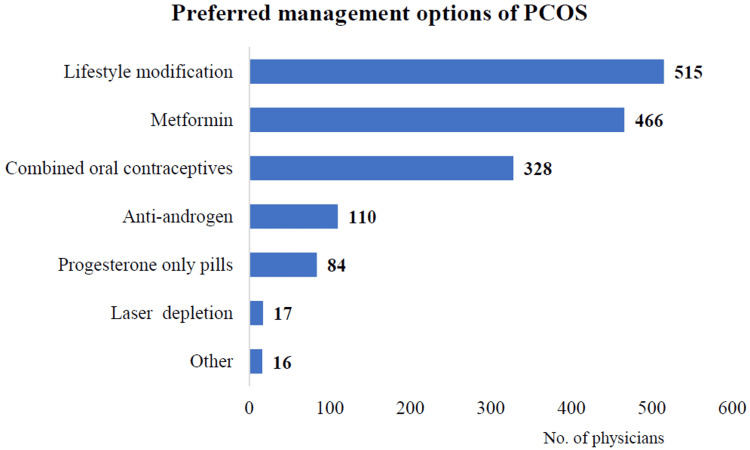 Figure 3
Figure 3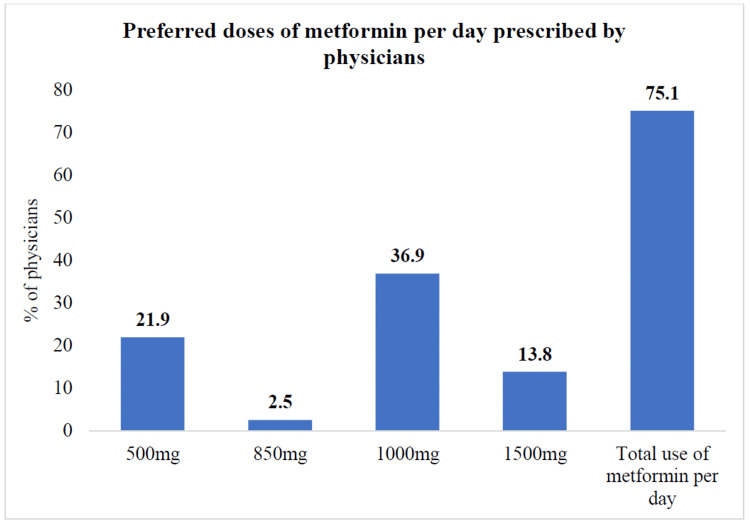 Figure 4
Figure 4| Characteristics | n | % |
| Location of practice | ||
| Inside Dhaka city | 295 | 45.9 |
| Outside Dhaka city | 294 | 45.7 |
| Not mentioned | 54 | 8.4 |
| Current discipline of practitioners | ||
| Endocrinology | 26 | 4 |
| Internal medicine | 6 | 0.9 |
| Gynecology & Obstetrics | 553 | 86 |
| Cardiology | 1 | 0.2 |
| Dermatology | 8 | 1.2 |
| Surgery | 1 | 0.2 |
| General practitioners | 50 | 7.8 |
| Experience of clinical practice (years) | ||
| <5 | 130 | 20.5 |
| 5-10 | 152 | 24.0 |
| 10-15 | 177 | 27.9 |
| >15 | 175 | 27.6 |
| Weekly number of total patients consulted | ||
| <50 | 268 | 41.7 |
| 50-100 | 100 | 16.7 |
| 100-500 | 223 | 34.7 |
| 500-1000 | 6 | 0.9 |
| >1000 | 3 | 0.5 |
| Weekly number of PCOS patients consulted | ||
| <10 | 383 | 59.6 |
| 10-20 | 183 | 28.5 |
| >20 | 70 | 10.9 |
| Physicians who prefer guidelines of PCOS | 573 | 89.1 |
| Physicians with no preferred guideline | 70 | 10.9 |
| Variables | n | % |
| Common reasons for the patients attending the clinic* | ||
| Hirsutism | 327 | 49.3 |
| Obesity | 284 | 44.2 |
| Menstrual disturbance | 524 | 81.5 |
| Metabolic disorders | 57 | 8.9 |
| Lack of fertility | 445 | 69.2 |
| Common laboratory tests prescribed* | ||
| Serum FSH | 184 | 28.6 |
| Serum LH | 316 | 49.1 |
| TSH | 429 | 66.7 |
| Prolactin | 297 | 26.2 |
| DHEA | 70 | 10.9 |
| Free testosterone | 209 | 32.5 |
| Fasting insulin | 137 | 21.3 |
| 17(OH) progesterone | 14 | 2.2 |
| OGTT | 292 | 44.4 |
| Fasting lipid profile | 118 | 18.4 |
| AMH | 154 | 24 |
| USG of the abdomen | 489 | 76 |
| Serum cortisol | 17 | 2.6 |
| Management plan of physicians* | ||
| Optimizing treatment | 422 | 31 |
| Counselling of the patients | 351 | 25 |
| Referred to respective specialist | 85 | 6 |
| Physicians feel that patients with PCOS should come for follow-up on the given date | 394 | 28 |
| Follow-up | 138 | 10 |
| Variables | n | % |
| Preferred follow-up schedule of the physicians for PCOS patients | ||
| In 4 weeks | 29 | 9 |
| In 6 weeks | 29 | 9 |
| In 8 weeks | 17 | 5 |
| In 12 weeks | 180 | 52 |
| In 24 weeks | 58 | 17 |
| Not sure | 31 | 9 |
| Physicians agreed to refer PCOS patients to specialists | 465 | 74.6 |
| Preferred specialists | ||
| Endocrinologist | 397 | 61.7 |
| Gynecologist | 203 | 31.6 |
| Medicine specialist | 7 | 1.1 |
| Dermatologist | 33 | 5.1 |
| Others | 2 | 0.4 |
| Physicians’ long-term concerns about PCOS | ||
| Type 2 diabetes | 360 | 56 |
| Infertility | 566 | 88 |
| Cardiovascular diseases | 145 | 22.6 |
| Obesity | 358 | 55.7 |
| Endometrial cancer | 158 | 24.6 |
| Psychological problems | 172 | 26.7 |
| Others | 3 | 0.5 |
| Variables | Adjusted OR (95% CI) | p-Value |
| Category of specialization of physicians managingPCOS patients | ||
| Endocrinologist | Ref | |
| Gynecology and Obstetrics | 2.133 (0.847-5.369) | 0.108 |
| Duration of experiences | ||
| <10 years | Ref | |
| ≥10 years | 1.267 (0.639-2.513) | 0.498 |
| Location of treatment of patients | ||
| Outside Dhaka | Ref | |
| Inside Dhaka | 2.495 (1.195-5.207) | 0.015 |
| Lifestyle modification as treatment | ||
| No | Ref | |
| Yes | 1.512 (0.679-3.367) | 0.312 |
| Preferred referral system to specialists of PCOS | ||
| No | Ref | |
| Yes | 0.310 (0.129-0.744) | 0.009 |
| Physician’s perspective on patient's follow-up visits | ||
| Does not come to follow-ups | Ref | |
| Comes to follow-ups | 1.557 (0.789-3.071) | 0.201 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOvarian function and disorders · Reproductive Biology and Fertility · Ovarian cancer diagnosis and treatment
Introduction
Polycystic ovary syndrome (PCOS) is a complex endocrine disorder characterized by menstrual irregularities, hyperandrogenism, and the presence of ovarian cysts. It is associated with serious comorbidities, including infertility, obesity, type 2 diabetes, cardiovascular disease, and psychiatric disorders such as anxiety and depression [1,2]. The disease has a significant public health impact affecting women of reproductive age, with an estimated global prevalence of approximately 16 million individuals [3,4]. In Bangladesh, the reported prevalence of PCOS varies widely, ranging from 6.11% among women attending gynecology outpatient departments to 92.16% among those consulting for hirsutism [5].
Over the past two decades, substantial progress has been made in understanding the epidemiology, phenotypes, evaluation, management, genetics, and long-term complications of PCOS. Various medical societies, including the National Institutes of Health (NIH), the Androgen Excess-PCOS (AE-PCOS) Society, and the Rotterdam consensus group, have published guidelines to aid in the diagnosis, treatment, and management of PCOS [6,7]. While these guidelines emphasize reproductive health aspects, PCOS impacts metabolic health and psychological well-being, necessitating a holistic approach to care. Diagnosing PCOS remains challenging due to multiple diagnostic criteria, inconsistent definitions of clinical and biochemical hyperandrogenism, varying phenotypes, and differences in presentation by age and ethnicity. Management typically focuses on symptom relief and prevention of long-term complications [8]. Early diagnosis is critical for regulating the menstrual cycle, controlling hyperandrogenism, and mitigating insulin resistance to reduce the risk of type 2 diabetes and cardiovascular disease. Early intervention also supports lifestyle changes and medical management to address obesity, improve fertility, alleviate psychological distress, and enhance overall quality of life [2,9]. Despite the availability of international guidelines, there is often a gap between evidence-based recommendations and clinical practice [10-12].
Globally, suboptimal diagnostic experiences and insufficient information provision for PCOS highlight the need for improved care [13,14]. A 2017 survey in the USrevealed that only 41% of practicing obstetricians and gynecologists and 68% of reproductive endocrinologists and infertility specialists were aware of the Rotterdam criteria for diagnosing PCOS [3]. In Europe, approximately three-quarters of obstetrician-gynecologists and endocrinologists use the Rotterdam criteria, while in North America, roughly half prefer the NIH criteria [12]. A recent international survey of gynecology and reproductive endocrinology practitioners reported similar findings [15].
In Bangladesh, PCOS is increasingly prevalent among adolescents and women of reproductive age [16], although approximately 64% of symptomatic women remain undiagnosed [17]. In the absence of a standardized referral system, patients often seek clinical consultations from diverse specialties and centers such as medical college hospitals, local hospitals, or even local drug vendors [18,19]. The absence of coordinated care pathways means that patients often receive fragmented care. For instance, women with acne or hirsutism might initially consult dermatologists, who may incidentally diagnose PCOS. Those experiencing menstrual irregularities commonly consult gynecologists or obstetricians. Patients with metabolic abnormalities, such as insulin resistance, might be diagnosed by endocrinologists or even cardiologists. This lack of streamlined referral processes can result in inconsistent diagnoses and hinder timely, comprehensive management. Moreover, the diversity of specialists involved, often without coordinated communication, can lead to suboptimal care for these patients.
As multiple international guidelines exist, notable differences are seen in diagnostic methods, knowledge, and treatment practices between different specialists. In a recent meta-analysis, the prevalence of PCOS in adolescents based on the Rotterdam criteria was 11.04%; based on the NIH criteria, it was 3.39%; and based on the Androgen Excess and Polycystic Ovary Syndrome Society, it was 8.03% [20]. However, due to the absence of a referral system and specific strategies regarding the management of PCOS in a low-resource setting like Bangladesh, there is a dearth of information available regarding the adherence to guidelines among physicians in Bangladesh. This limits understanding of local diagnostic patterns, adherence to international guidelines, and referral practices, which are essential for adapting context-specific interventions. This study aims to investigate the diagnostic and management practices for PCOS among physicians in Bangladesh. Understanding current practices is essential for identifying areas for improvement and implementing evidence-based guidelines effectively in clinical settings.
Materials and methods
Study design and participant selection
This nationwide cross-sectional study was conducted among general practitioners and specialists working in public and private hospitals across Bangladesh. Physicians were contacted through the professional networks of the principal investigator and her team, with efforts to include participants from all divisions. The study period was between April 2024 and October 2024. Physicians from various specialties were included along with the general practitioners.The study includes specialists from the following disciplines: 1) Endocrinology, 2) Gynecology & Obstetrics, 3) Internal Medicine, 4) Cardiology, 5) Psychiatry, 6) Dermatology, and 7) Surgery.
Sample size estimation
The sample size was calculated using the formula for a 95% confidence level (z = 1.96), with an assumed prevalence of 0.5 (p) and a margin of error of 0.05 (d). Given the study's multicenter design, a design effect of 1.5, a 90% response rate, and a 10% non-response rate were factored in, resulting in a required sample size of 698 participants. This study employed a convenience purposive sampling method, including only registered physicians actively involved in patient care. Recruitment was initiated through the investigators' networks, with participants encouraged to share the questionnaire with their colleagues. After excluding 55 incomplete responses, 643 physicians were included in the final analysis.
Study procedure
A semi-structured questionnaire was designed to collect information in two main sections: Sociodemographic characteristics: Specialty, years of clinical experience, practice setting, and patient volume. PCOS-specific practices: Number of PCOS patients treated weekly, common clinical presentations, diagnostic approaches, treatment strategies, follow-up schedules, adherence to clinical guidelines, referral practices, and long-term management concerns.
The questionnaire comprised 23 questions and was designed to be completed within 10 to 20 minutes. It was developed through an extensive literature review and consultations with academic faculty. The questionnaire, provided in English, included both open-ended and closed-ended questions. A pilot test involving 10 physicians from Bangabandhu Sheikh Mujib Medical University (BSMMU) was conducted to ensure clarity and reliability. Participation was voluntary, with responses anonymized to protect confidentiality. Participants were instructed to complete the survey only once, and no question was mandatory. Further details are provided in the Appendix.
Ethical considerations
Ethical approval was obtained from the Institutional Review Board (IRB) of Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh, and written informed consent was secured from all participants. The study adhered to the ethical principles outlined in the Declaration of Helsinki and its subsequent amendments.
Statistical analysis
Following data collection, the dataset was cleaned and organized using Microsoft Excel (Microsoft, Redmond, WA). Statistical analysis was performed using SPSS version 26.0 (IBM Corp., Armonk, NY). Summary statistics were employed, with categorical variables presented as frequencies and percentages and continuous variables as means with standard deviations (SDs).
Results
Physician characteristics and practice information
A total of 643 physicians participated voluntarily, recruited through professional networks. Some specific demographic details, like age and gender of the physicians, were excluded to focus on clinical practices regarding PCOS. The study aimed to identify physician specialty groups involved in PCOS care, assess their diagnostic and treatment approaches, and explore referral practices.
Among the participating physicians, 46% were from Dhaka, with the rest practicing across other cities and towns. Most were specialists in Gynecology and Obstetrics, followed by other specialties and physicians as general practitioners. Over half of these participants had more than 10 years of experience, and a majority (41.7%) of physicians managed less than 50 patients weekly. Among the physicians, only 10.9% managed PCOS patients during a week, where the majority (59.6%) had less than 10 PCOS patients per week. A majority of these physicians followed clinical guidelines, mainly the European Society of Human Reproduction and Embryology (ESHRE), but 10.9% were unsure which guidelines to use, revealing potential gaps in knowledge or access to standard care protocols. About 89.1% (95% CI: 86.7%-91.5%) of physicians followed clinical guidelines, mainly the ESHRE, where almost 10.9% were unsure which guidelines to use (Table 1). However, confidence intervals were not mentioned in the table.
Preferred guidelines for PCOS
A majority of the participating physicians reported adherence to the Rotterdam/ESHRE2023 guidelines for both the screening and management of PCOS, followed by other known guidelines. However, about 7% to 9% of participants did not follow any specific guidelines for PCOS screening or management. Furthermore, a small proportion of physicians (1.7% for screening and 1.2% for management) reported relying on other recommendations for PCOS screening and treatment (Figure 1). These findings highlight variability in the application of guidelines, emphasizing the need for uniformity in clinical practice to ensure standardized patient care.
A. Preferred guidelines for screening PCOS; B. preferred guidelines for PCOS managementPCOS, polycystic ovary syndrome; NIH, National Institutes of Health; ESHRE, European Society for Human Reproduction and Embryology; AEPS, Androgen Excess and PCOS Society; EBG,Evidence-Based Guidelines.
Guideline usage by specialty
Figure 2 illustrates the distribution of guideline adherence among physicians managing PCOS, with percentages categorized by medical specialty. The ESHRE guidelines emerged as the most widely followed among Gynecology & Obstetrics physicians, whereas Evidence-Based Guidelines (EBG) were adhered to mostly by endocrinologists.
Comparison of the use of guidelines among gynecologists, endocrinologists, and other specialists (n = 643)PCOS, polycystic ovary syndrome; NIH, National Institutes of Health; ESHRE, European Society for Human Reproduction and Embryology; AEPS, Androgen Excess and PCOS Society; EBG,Evidence-Based Guidelines.
Diagnostic approaches for PCOS by physicians
In this study, most physicians diagnosed PCOS in patients presenting with menstrual disturbances, infertility, hirsutism, and obesity. For initial diagnosis and treatment, they frequently recommended abdominal ultrasound (76%), thyroid-stimulating hormone (TSH) testing (66.7%), serum luteinizing hormone (LH) (49.1%), and oral glucose tolerance tests (OGTT) (44.4%). A majority (65.6%) prioritized optimizing treatment, followed by counseling on lifestyle modifications and regular follow-ups, reflecting a comprehensive approach that addresses both reproductive and metabolic health(Table 2).
Management of PCOS by physicians
Lifestyle modifications (80.1%, 95% CI: 77%-83.2%) were the most frequently recommended approach, followed by metformin, combined oral contraceptives, anti-androgens, and progesterone-only pills. Also, the less frequently chosen approaches include anti-androgens, progesterone-only pills, laser depletion for hair reduction, and other unspecified treatments. The data highlightlifestyle interventions and pharmacological strategies like metformin or contraceptives as primary management options for PCOS (Figure 3). However, the confidence interval is not shown in the figure.
Management options preferred by physicians for PCOS patients (n = 643)PCOS, polycystic ovary syndrome.
Metformin appeared as the most commonly preferred treatment for PCOS, with 75.1% of physicians selecting it as their primary choice. The initial prescribed dose was typically 500 mg per day, gradually increasing based on patient response. The majority of physicians favored a daily dose of 1000 mg, administered in divided doses for optimal efficacy and tolerability. A higher dose of 1500 mg per day was less commonly prescribed, with only 13.8% of physicians choosing this regimen (Figure 4).
Dose of metformin per day preferred by physicians for management of PCOS (n = 643)PCOS, polycystic ovary syndrome.
Follow-up of patients with PCOS
A majority of the participants reported scheduling follow-up visits for their PCOS patients, with 52% preferring a 12-week follow-up interval. The study also highlighted referral practices, with 74.6% of physicians referring patients to specialists, mainly endocrinologists, followed by gynecologists, dermatologists, and medicine specialists (Table 3).
Infertility was the most common long-term concern for PCOS patients, mentioned by 88% of doctors. Other major concerns included diabetes (56%), obesity (55.7%), mental health issues (26.7%), uterine cancer (24.6%), and heart problems (22.6%). Only 0.5% of doctors mentioned concerns outside these areas.
In multivariate analysis, physicians practicing inside Dhaka were significantly more likely to adhere to PCOS guidelines (adjusted odds ratio [AOR] = 2.50, 95% CI: 1.20-5.21, p = 0.015). In contrast, those who preferred referring patients to specialists had lower odds of adherence (AOR = 0.31, 95% CI: 0.13-0.74, p = 0.009). No significant associations were observed for physician specialization, duration of experience, use of lifestyle modification, or follow-up perspectives (Table 4).
Discussion
The study provides critical insights into the practices of physicians in Bangladesh regarding the diagnosis and management of PCOS. A total of 643 physicians participated, with the majority specializing in gynecology and clustered in Dhaka. Most adhered to established guidelines, particularly the Rotterdam/ESHRE criteria for diagnosing PCOS. Physicians frequently encountered symptoms such as irregular menstrual cycles, infertility, and weight gain, relying on diagnostic tools like ultrasounds and hormonal assays. Nearly two-thirds of the management strategies emphasized lifestyle modifications, complemented by metformin and combined oral contraceptives, reflecting global best practices. However, gaps in knowledge and adherence to guidelines persist, as some physicians expressed uncertainty about which guidelines to follow. Long-term concerns, including infertility, metabolic disorders, and cardiovascular risks, underscore the need for comprehensive, evidence-based care and an effective referral system [10,11].
This study included physicians from diverse regions of the country, revealing that most followed at least one established guideline for PCOS management. The most commonly cited guidelines were those from the NIH, the Rotterdam/ESHRE criteria, the Endocrine Society, and the AE-PCOS Society. Gynecologists and obstetricians predominantly followed the ESHRE guidelines, while other specialists varied in their preferences. Dokras et al. reported that similar patterns have been observed with around 70% of physicians followed ESHRE guidelines [3].Consistent with global patterns, the Rotterdam/ESHRE criteria, introduced in 2003, were widely utilized, requiring two of three key features for diagnosis: irregular or absent ovulation, signs of hyperandrogenism, and polycystic ovaries on ultrasound, excluding other conditions with similar symptoms. As PCOS presents in many different ways, the NIH workshop stressed the importance of identifying and studying specific PCOS types to better understand their impact, severity, and long-term effects across different patient groups [7,21].
The study ensured balanced geographic representation, with nearly equal participation from physicians practicing outside Dhaka. Over half of the respondents had more than a decade of clinical experience, reflecting a high level of expertise. The predominance of gynecologists and obstetricians aligns with the study’s reproductive health focus, corroborated by earlier research that identified gynecologists as the preferred specialists for referral [22]. Diagnostic practices frequently included ultrasound and hormonal assays, reflecting global trends. However, a notable emphasis on thyroid function tests, such as serum TSH, was observed, diverging from Western practices that prioritize metabolic markers and insulin resistance [23].
Physicians in the study managed approximately 500 patients per week, including 20 PCOS cases, underscoring the condition’s prevalence. In the United States and Europe, lifestyle modifications, particularly weight loss, are considered the first-line treatment for PCOS, with metformin and oral contraceptives commonly prescribed in these regions [14,24]. Aerobic exercise, in particular, has been shown to improve reproductive function in women with PCOS by normalizing menstrual cyclicity and ovulation rates. Improvements in insulin sensitivity through exercise are associated with increased menstrual regularity and ovulation in approximately 50% of women with PCOS [9]. Research suggests that lifestyle interventions, such as aerobic exercise, improve reproductive outcomes by normalizing menstrual cycles and enhancing insulin sensitivity. Metformin, commonly prescribed for PCOS-related infertility, is administered following standard protocols of gradual dose titration [12,25,26].
Most physicians schedule follow-ups every four to 12 weeks, using tests such as serum TSH levels and abdominal ultrasound to monitor treatment efficacy and complications. This follow-up frequency aligns with global recommendations, emphasizing the importance of long-term management and screening for diabetes and cardiovascular disease [27,28]. The primary long-term concerns for PCOS patients include infertility, obesity, type 2 diabetes, psychological issues, endometrial cancer, and cardiovascular disease. Suggestions for improving PCOS care included educational materials, webinars, and professional development resources, underscoring the need for enhanced support for healthcare providers [29].
Moreover, this study assessed some important factors influencing physician adherence to PCOS guidelines. Physicians practicing within Dhaka were significantly more likely to adhere to guideline-based management compared to those outside Dhaka. This may reflect better access to continuing medical education, academic networks, and exposure to updated clinical resources in urban centers, which are often limited in peripheral regions. Similar urban-rural disparities were found in other studies on various topics, underscoring the need to strengthen training opportunities and resource availability in rural settings here [30,31]. Interestingly, physicians who preferred referring PCOS patients to specialists had lower odds of adhering to guidelines. This could indicate limited confidence in managing PCOS cases themselves or an overreliance on referral pathways. While referral is appropriate for complex cases, excessive referral may delay the timely initiation of evidence-based care. Interventions aimed at empowering non-specialist physicians through targeted training and decision-support tools could enhance guideline adherence in such contexts.
PCOS remains a prevalent global health issue, presenting reproductive, metabolic, and psychological challenges. Early diagnosis and consistent management are vital for improving patient outcomes. This study, one of the largest in Bangladesh, offers a comprehensive analysis of nationwide physician practices and highlights opportunities to address gaps in knowledge and guideline adherence. The findings emphasize the need for educational initiatives aligned with evidence-based guidelines and suggest that future research should focus on patient-centered care models to enhance satisfaction and outcomes.
This study has several limitations. The predominance of gynecologists among respondents may have introduced sampling bias, emphasizing reproductive aspects over metabolic or psychological dimensions. Reliance on self-reported practices and the absence of patient outcome data further limit the validity of the findings. The exclusion of patient perspectives restricts understanding of care experiences and satisfaction. Moreover, the use of convenience sampling means that results may not be generalizable beyond the study respondents or to other healthcare settings. Future studies should adopt mixed-methods approaches incorporating both physician and patient perspectives to better capture practice patterns, care gaps, and contextual barriers. At the policy level, promoting adherence to clinical guidelines through targeted training, structured referral systems, and wider dissemination of international recommendations alongside emphasis on lifestyle interventions, potentially supported by mindfulness techniques, may help improve patient outcomes.
Conclusions
In summary, this nationwide survey offers valuable insights into current PCOS management practices among Bangladeshi physicians, particularly regarding their use of established international guidelines. Most respondents reported familiarity with at least one evidence-based recommendation; however, uniform adherence to a single guideline tailored to the Bangladeshi context is lacking. Variability in follow-up and referral practices further highlights the urgent need for structured referral pathways and a standardized care model for PCOS diagnosis and management among physicians. Moreover, implementing targeted training modules, strengthening the dissemination of international guidelines, and introducing system-level interventions could enhance practice consistency and ultimately improve patient outcomes. Beyond its national relevance, this study makes an important global contribution by offering rare insights from a South Asian LMIC (low- and middle-income countries) context, which may enable scopes of future cross-country comparisons on physician practices and inform strategies to improve consistency of PCOS care in resource-constrained settings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Polycystic ovary syndrome: An updated overview foregrounding impacts of ethnicities and geographic variations Life (Basel) Yasmin A Roychoudhury S Paul Choudhury A 19741220223655634010.3390/life 12121974 PMC 9785838 · doi ↗ · pubmed ↗
- 2Polycystic ovary syndrome: Etiology, current management, and future therapeutics J Clin Med Singh S Pal N Shubham S Sarma DK Verma V Marotta F Kumar M 14541220233683598910.3390/jcm 12041454 PMC 9964744 · doi ↗ · pubmed ↗
- 3Gaps in knowledge among physicians regarding diagnostic criteria and management of polycystic ovary syndrome Fertil Steril Dokras A Saini S Gibson-Helm M Schulkin J Cooney L Teede H 1380138610720172848350310.1016/j.fertnstert.2017.04.011 · doi ↗ · pubmed ↗
- 4An epidemiological survey: Effect of predisposing factors for PCOS in Indian urban and rural population Middle East Fertil Soc J Vidya Bharathi R Swetha S Neerajaa J 313316222017
- 5Prevalence and characteristics of women with polycystic ovary syndrome in Bangladesh - A narrative review Bangladesh J Endocrinol Metab Kamrul-Hasan AM Aalpona FZ Mustari M Selim S 202822023
- 6The Androgen Excess and PCOS Society criteria for the polycystic ovary syndrome: The complete task force report Fertil Steril Azziz R Carmina E Dewailly D 4564889120091895075910.1016/j.fertnstert.2008.06.035 · doi ↗ · pubmed ↗
- 7Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS)Hum Reprod Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group 41471920041468815410.1093/humrep/deh 098 · doi ↗ · pubmed ↗
- 8Awareness of lifestyle modifications in the management of polycystic ovarian syndrome: A hospital-based descriptive cross-sectional study Cureus Kaundal A Renjhen P Kumari R 015202310.7759/cureus.36889 PMC 1015110537139281 · doi ↗ · pubmed ↗