Unmasking the Hidden Risk of Systemic Toxicity from Topical Salicylates
Neelou Tabatabai, Swetaleena Dash, James A. Chenoweth, Timothy E. Albertson

TL;DR
This paper highlights the risk of systemic toxicity from topical salicylates and emphasizes the importance of early detection and patient education.
Contribution
A new case of topical salicylate toxicity is presented alongside a systematic review of historical cases to better understand the risks and clinical manifestations.
Findings
44 cases of topical salicylate toxicity were identified, with tachypnea and vomiting being the most common symptoms.
The new case involved an elderly male with altered mental status and elevated anion gap.
The study emphasizes the need for clinicians to consider salicylate toxicity in patients with unexplained metabolic or mental changes.
Abstract
Topical salicylates are commonly found in over-the-counter medications and are applied for pain relief or to treat dermatologic conditions. While generally considered safe, they can cause systemic toxicity under certain conditions. We conducted a systematic review of topical salicylate toxicity. This comprehensive review of previously reported cases highlights the risks, clinical presentations, and management considerations of systemic toxicity from topical salicylates. We present a new case of topical salicylate toxicity and conducted a comprehensive systematic literature search from 1952–2024 using PubMed, Google, and Google Scholar. Our search was supplemented by cross-referencing previous studies to identify cases and reviews of topical salicylate toxicity. We then performed a descriptive analysis of the cases, summarizing key information such as clinical presentation, blood…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
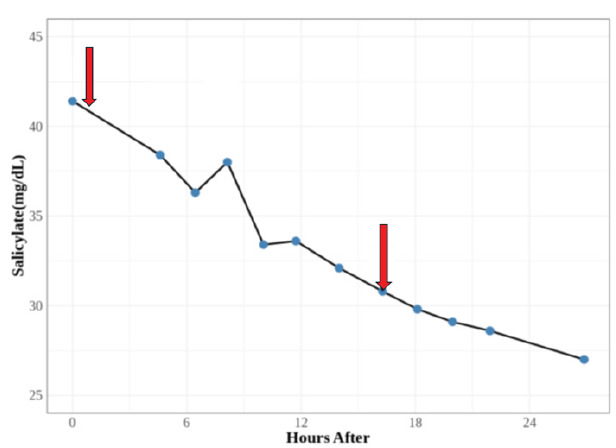 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsImmunotoxicology and immune responses · Advancements in Transdermal Drug Delivery · Cell Image Analysis Techniques
INTRODUCTION
Derived from willow bark (Salix alba), topical salicylates are used for both pain and dermatologic concerns. They are found in many common over-the-counter (OTC) products including aspirin, bismuth subsalicylate, and oil of wintergreen. When salicylates are applied to the skin, they work by acidifying the stratum corneum, promoting the desquamation of corneocytes, and reducing intercellular cohesion. This disruption weakens the skin’s barrier properties and facilitates topical absorption. Topical salicylates are available in a variety of formulations, including patches, gels, and creams, with concentrations ranging from 0.5% for cosmetic purposes to 50% for treating conditions such as warts.1 Many of these OTC products are heavily advertised by famous, former pro athletes without any risk discussion.
Despite their widespread use, topical salicylates can be absorbed enough to cause systemic toxicity particularly when a large dose of high concentration (milligrams per milliliter [mg/mL]) salicylates are applied to large body surface areas (amount applied) or with repeated applications (frequency). Individuals with risk factors such as decreased renal function or compromised skin integrity are at greater risk.2 However, toxicity can also occur in individuals without traditional risk factors highlighting the need for greater public education and clinical awareness about topical salicylate products. The condition of the skin, the concentration of the salicylate product, the vehicle/diluent used in the product, the frequency of application, and the surface area applied are all important variables that determine topical dosing and the potential for toxicity.
A recent case of an elderly male with altered mental status secondary to topical salicylate toxicity emphasizes that this remains a potential source of salicylate toxicity. The patient’s presentation demonstrates the potential for significant systemic absorption even in the absence of well-known risk factors such as damaged skin or significant renal impairment. Additionally, we review previously published case reports of topical salicylate toxicity to emphasize associated risks and the importance of early recognition, intervention, and prevention of misuse particularly in high-risk populations such as pediatric and elderly demographics. The dermal route of salicylates absorption, although rare, remains a clinical problem seen in the emergency department (ED).
CASE REPORT
A 78-year-old male with achalasia type II, advanced dementia, alcoholic cirrhosis complicated by gastric varices, chronic heart failure with preserved ejection fraction, traumatic brain injury, and paroxysmal atrial fibrillation presented to the ED because of altered mental status over the prior three days. His family was concerned that he was less communicative and had a loss of appetite. He denied any symptoms of dizziness, lightheadedness, tinnitus, nausea, or vomiting. His medications included 12.5 mg of trazodone at night and 15 mL of lactulose twice daily. After a review of the chart and interviewing the family, there were no oral medications containing any formulations of salicylate in the household.
Initial vital signs included a blood pressure of 107/64 millimeters of mercury (mm Hg), heart rate of 85 beats per minute, and respiratory rate of 18 breaths per minute with an oxygen saturation of 98% on room air. The oral temperature was recorded as 36.9°C. The skin exam did not reveal any signs of lotions, patches, acute trauma, rashes, or infection. A basic metabolic panel revealed a creatinine of 1.02 mg per deciliter (mg/dL) similar to his prior values. Other initial lab work was notable for an elevated anion gap of 16 (sodium 141 millimoles (mmol) per dL; chloride 103 mmol/dL; carbon dioxide 22 mmol/dL; and potassium 4.0 mmol/dL); and a slightly elevated venous serum pH of 7.45. A comprehensive blood panel included a white blood cell count of 3.8 thousand cells per microliter (cells/μL), hemoglobin of 11.0 grams per dL (g/dL) and platelet count of 140 thousand cells/μL. Urinalysis found moderate bacteria, trace leukocyte esterase and trace ketones. An arterial blood gas found a partial pressure of oxygen of 100 mm Hg, 94% saturated, a partial pressure of carbon dioxide of 31 mm Hg, and a pH of 7.54 consistent with a respiratory alkalosis/alkalemia with mild hyperventilation. Imaging results, including a computed tomography of the head without contrast and a chest radiograph, were both unremarkable for any acute findings.
In evaluating the cause of his change in mental status and elevated anion gap, a serum salicylate level was drawn. The serum salicylate level was elevated to 41.4 mg/dL. His ethanol and acetaminophen levels were undetectable. When the family was told about the elevated salicylate level, they remembered that he had applied a three-ounce tube of ICY HOT pain-relieving cream (30% methyl salicylate and 10% menthol) to his back (estimated body surface area 18%) within a two-day period, prior to presentation to the ED. It is not known whether he washed his hands after applications. No occlusive dressings were used. The use instructions for the cream are vague and suggest applying a thin layer to the affected area and massage until thoroughly absorbed into the skin no more than 3–4 times a day. Washing hands after application is also suggested. Throughout his stay in the ED, his vital signs remained stable.
A sodium bicarbonate infusion (3 amps of sodium bicarbonate in a liter of dextrose 5% in water after removing 100–150 mL, and infused at 100 mL per hour) with potassium chloride was started in the ED. The patient was admitted to the intensive care unit for close monitoring of symptoms, and frequent repeat serum salicylate levels, blood gases, and electrolyte values. Additional potassium was given to maintain the serum level ≥ 4 mmol/dL Although the patient denied symptoms of a urinary tract infection, given his urinalysis findings and altered mental state, he was empirically treated with antibiotics. The sodium bicarbonate infusion ran ≈ 12 hours and was stopped when the serum salicylate decreased below 30 mg/dL. The anion gap returned to normal. While the family was adamant that the only salicylates to which the patient had access were the topical products, we could not completely rule out additional oral or chronic poisoning. The patient was discharged after two days of hospitalization at his baseline mental status and with the last measured serum salicylate level of 27.0 mg/dL. Figure 1 summarizes the serum salicylate levels in this patient.
METHODS
We performed a systematic and comprehensive review of cases of topical salicylate toxicity. A literature search using PubMed, Google, and Google Scholar identified relevant publications from 1952–2024. The search strategy employed the following combinations of terms: “topical salicylate toxicity,” “poisoning,” “salicylate,” “methyl salicylate,” and “case reports.” The search resulted in all available publications and specifically targeted peer-reviewed case reports, case series, conference abstracts, reviews, and letters to the editor. It also included texts found in Dutch, English, French, German, Italian, Polish, and Turkish. We used two previous literature reviews on topical salicylate toxicity published prior to our study to ensure all the papers were included. The first, by Brubacher and Hoffman in 1996, reviewed 17 cases.3 A subsequent review by Madan and Levitt in 2014 expanded the dataset to include 25 cases but did not include all the cases in the first review.2 The case data extractions were done by all the authors.
Some published literature was available only in abstract form. In those cases, we extracted all relevant information provided, such as the highest plasma salicylate concentrations and patient symptoms. However, if critical details such as patient outcomes were missing, this limitation was noted as “not available.” If no specific information about the salicylate poisoning could be obtained from an article or from the prior reviews, we excluded the article from our review. We also excluded five case reports due to lack of availability of the paper or incomplete details such as salicylate blood levels and case data.4–8 From each case report, we recorded the year of publication, patient age, sex, concentration of topical salicylate/vehicle, peak reported salicylate concentration (mg/dL), day of peak plasma levels, underlying diseases, case outcome, and physical exam findings. If available, we noted body weight, salicylate concentration, diluent, estimated surface exposure, length of exposure, and timing of administration. All salicylate units were converted into mg/dL for consistency. Intact skin was defined as having no compromised skin integrity secondary to underlying dermatological conditions.
RESULTS
We found an additional 12 new cases of topical salicylate toxicity from published literature not included in the previous reviews. This expanded the total reported cases to 44, including the current case presented here (Table 1). The first review published in 1996 reviewed 17 cases.3 The 2014 review expanded the number of cases found to 25 but did not include all the cases in the first review.2 Seven were abstracts only.9–15 Of the 43 previously published case reports, eight were published in languages other than English.9–11,16–21
The cases reviewed included a wide age range; the youngest cases involved three newborns (< one month of age), and the oldest were two 80-year-olds.3,26,29,32,34 Demographic data showed that 67.4% (29/43) of cases occurred in males, 30.2% (13/43) in females, and one case (1/43) of no specified gender. Most cases occurred in patients > 40 years of age (18 cases). Children under one accounted for seven cases, while there were only four cases in children between 1–10 years of age. Two cases had no reported ages.
The lowest plasma concentration reported was 14.0 mg/dL, and the highest was 223.0 mg/dL.21,33 Two cases did not have recorded plasma concentrations, and one was sampled postmortem.26,40 The most common symptoms of salicylate poisoning noted included tachypnea (32.5%), vomiting (25.5%), nausea (21.0%), and tinnitus (21.0%). Of the 43 previously reported cases, the most common underlying medical conditions associated with topical toxicity were 17 patients with psoriasis, (35.5%) and 10 (23.2%) with ichthyosis. Seven cases involved toxicities with intact skin.17,22,24,26,27,33,44 Death occurred in five cases (11.6%). Death was observed in patients with psoriasis and tinea imbricata, and there was one isolated death reported in a patient with intact skin.9,26,40 The final outcome of seven cases was not available.10,11,36,37,42,43
DISCUSSION
Our case report exemplifies the rare but important instance of systemic salicylate toxicity resulting from topical application of methyl salicylate over a large surface area in an elderly patient with multiple comorbidities. Because he applied the topical salicylates on himself, the amount that he may have ingested intentionally or accidentally is unknown. Since the last published reviews on topical salicylate poisonings, 13 cases have been added with 12 new cases reported from the literature and one case reported here.2,3 Despite reduced use of topical salicylate in dermatology, cases of topical salicylate toxicity continue to be reported. When informed of the blood salicylate levels, the family disclosed that the patient had recently been using a popular, aggressively marketed, methyl salicylate-containing cream with multiple applications to about 18% of his body surface area within a two-day period. Notably, despite intact skin and near-normal renal function, the patient had significant absorption of salicylate and a prolonged salicylate half-life resulting in toxicity.
In a voluntary study involving human subjects, the half-life after complete absorption of dermal salicylate was obtained from plasma concentrations. Subjects wore from 2–8 adhesive patches impregnated with methyl salicylate. The harmonic mean terminal half-life of methyl salicylate was determined to be 3.0 ± 1.2 hours.4 The half-life of methyl salicylate in our case report was prolonged and suggests continued absorption, additional oral exposure, or chronic salicylate exposure.
In cases where data were available, as in the case presented here, toxicities typically manifested within a few days of topical salicylate use. Severe toxicities, including seizures, severe metabolic acidosis, cerebral edema, acute respiratory distress syndrome, hypoglycemia, hypoglycorrhachia, ketosis, and death, were most often linked to applications of high-concentration salicylate products involving large body surface areas over extended periods. Elevated and toxic doses of salicylate typically occur with blood levels above 20–30 mg/dL, and can disrupt key physiological processes, leading to a wide range of harmful effects. Elevated toxic salicylate levels can impair oxidative phosphorylation, resulting in adenosine triphosphate production failure while also increasing oxygen consumption, metabolic acidosis, and heat generation.
Clinical manifestations in early toxicity often occur from stimulation of the brain’s respiratory center causing initial tachypnea and respiratory alkalosis, as seen in this case. The inhibition of Krebs cycle enzymes reduces glucose availability systemically and in the brain. This promotes organic acid accumulation, which leads to metabolic acidosis. Resultant significant fluid and electrolyte losses lead to dehydration, sodium and potassium depletion, and reduced buffering capacity. Once absorbed, salicylic acid is metabolized by the liver to more water-soluble byproducts.5 In considering topical dosing, the surface area treated, the concentration of salicylate used should not be excessive; the use of occlusive dressings, the frequency of application, and the patient’s underlying volume- and renal-status must be considered.6 A study with patients with active psoriasis found that after 10 hours with occlusive dressing over the topical salicylates, 60% of the salicylate was absorbed.6
The priority in treating any poisoned patient is assessing the airway, oxygenation, and maintaining perfusion of organs. Once toxicity is identified, it is critical to lower the salicylate levels. Resuscitation should begin with thorough skin decontamination with soap and water to remove any remaining drug and fluids, and dextrose 5% with 3 ampules of sodium bicarbonate to buffer the metabolic acidosis; added potassium chloride increases renal excretion and helps to prevent brain absorption by ion trapping of the salicylate. Potassium chloride is often added to prevent hypokalemia, the presence of which will inhibit alkalinization of the urine. Hemodialysis is indicated for severe acidosis, acute respiratory distress syndrome, severe altered mental status, seizures, kidney failure, refractory hypotension, and salicylate levels greater than 100 mg/dL for acute exposures and potentially lower levels for chronic exposure.7 The Extracorporeal Treatments in Poisoning workgroup recommendations and indications for salicylate poisoning are very useful.45
In addition to the concentration and surface area of application, different formulations of topical salicylic acid have different levels of systemic absorption. A study by Morra et al found that the methyl salicylate used in the current case demonstrated higher absorption compared to other formulations such as trolamine salicylate.8 Methyl salicylate reached detectable serum salicylate levels within one hour of application with cumulative absorption increasing after repeated applications. In contrast, trolamine salicylate showed minimal skin absorption, with serum salicylate levels often undetectable and significantly lower recovery in urine.8 Our review of 43 previous cases plus the current case of topical salicylate toxicity corroborates this observation.
As summarized in Table 1, symptoms of topical salicylate toxicity are broad and generally develop within a few days of use, particularly when applied over large body surface areas, compromised skin, or with repeated applications. While the most common findings in the literature review were metabolic abnormalities, altered mental status, tachypnea, vomiting, nausea, and tinnitus, the current patient had altered mental status, metabolic acidosis with elevated anion gap, and tachypnea (with respiratory alkalemia) but only reported tinnitus after he regained his baseline mental status and the salicylate levels had fallen. This suggests that older patients or those with comorbid conditions like dementia can be a challenge to diagnose and demonstrates the need for heightened clinical suspicion when presented with a limited history and symptoms.
This case report and descriptive analysis of similar historical cases emphasizes the need for further patient education about the potential toxicity of OTC topical salicylates and their use to improve their safety among the general population and particularly in vulnerable populations such as children, renal-compromised patients, and patients with baseline altered mental status. This report reinforces the need for clinicians to suspect and inquire about topical salicylate use in patients with an elevated anion gap and altered mental status given its widespread use and availability.
LIMITATIONS
Retrospective literature research has several limitations. Some older publications, particularly those predating digital archiving, may have been excluded in the search due to their limited availability and not being included in the electronic databases searched. A few publications were not available. If available, abstracts were used, but some provided limited data such as patient outcomes, sex, age, and symptoms. Publication bias clearly favors publication of toxic cases but considering the limited number of cases found over 72 years, the incidence of topical salicylate toxicity must be low. Case reports have significant limitations. This case report also has limitations in terms of history and potential chronic or oral dosing of salicylates that was denied by the family but still could have happened.
CONCLUSION
Topical salicylates have the potential for systemic toxicity particularly when large doses of methyl salicylate are applied in high concentrations in vulnerable populations such as patients with compromised renal function, and in pediatric patients with a large surface-to-body ratio. The inappropriate use of methyl salicylate products in particular, especially in high concentrations over large body surface areas, on compromised skin, and with repeated applications can pose significant health risks. Clinicians should maintain a high index of suspicion for salicylate toxicity in patients presenting with non-specific symptoms such as altered mental status, or unexplained metabolic acidosis or tachypnea especially in those with a history of topical salicylate use. Although salicylate toxicity is not common, early recognition and intervention are essential to prevent or reduce clinical toxicity and ensure rapid resolution. Widespread patient education about the toxicological risk of these heavily advertised topical salicylate products is also needed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yeoh SC Goh CF Topical delivery of salicylates Drug Deliv Transl Res 202212598110013390798610.1007/s 13346-021-00988-5 · doi ↗ · pubmed ↗
- 2Madan RK Levitt JA review of toxicity from topical salicylic acid preparations J Am Acad Dermatol 2014704788922447242910.1016/j.jaad.2013.12.005 · doi ↗ · pubmed ↗
- 3Brubacher JR Hoffman RS Salicylism from topical salicylates: review of the literature J Toxicol Clin Toxicol 19963444316869955810.3109/15563659609013814 · doi ↗ · pubmed ↗
- 4Martin D Valdez J Boren J Dermal absorption of camphor, menthol, and methyl salicylate in humans J Clin Pharmacol 20044410115171534261610.1177/0091270004268409 · doi ↗ · pubmed ↗
- 5Temple AR Pathophysiology of aspirin overdosage toxicity, with implications for management Pediatrics 1978625 Pt 2 Suppl 8736364398 · pubmed ↗
- 6Taylor JR Halprin KM Percutaneous absorption of salicylic acid Arch Dermatol 1975111674031094962 · pubmed ↗
- 7Runde TJ Nappe TM Salicylates toxicity Okocha Shumway Stat Pearls Treasure Island (FL)Stat Pearls Publishing 202329763054 · pubmed ↗
- 8Morra P Bartle WR Walker SE Serum concentrations of salicylic acid following topically applied salicylate derivatives Ann Pharmacother 199630993540887685010.1177/106002809603000903 · doi ↗ · pubmed ↗