Hydrogen-Positive Small Intestinal Bacterial Overgrowth (SIBO) in Japanese Patients With Chronic Intestinal Pseudo-Obstruction (CIPO): A Cross-Sectional Study
Takanori Igarashi, Kentaro Tominaga, Kunihiko Yokoyama, Takuya Wakabayashi, Yuichi Kojima, Yuzo Kawata, Naruhiro Kimura, Kazuya Takahashi, Akira Sakamaki, Shuji Terai

TL;DR
This study found that hydrogen-positive small intestinal bacterial overgrowth is common in Japanese patients with chronic intestinal pseudo-obstruction, but methane-producing bacteria are rare.
Contribution
First investigation of SIBO gas phenotypes in Japanese CIPO patients using glucose breath testing.
Findings
Hydrogen-positive SIBO was present in 50% of CIPO patients but none in controls.
No CIPO patients met criteria for intestinal methanogen overgrowth.
H₂-SIBO in CIPO was linked to lower BMI and more frequent diarrhea.
Abstract
Background: Evidence for small intestinal bacterial overgrowth (SIBO) in chronic intestinal pseudo‑obstruction (CIPO) remains limited in Asian populations and by gas phenotype. This study aimed to determine the prevalence and gas phenotype distribution (hydrogen-positive SIBO vs. intestinal methanogen overgrowth) in Japanese patients with CIPO using glucose breath testing and to describe associated clinical features. Methods: This single‑center cross‑sectional study was conducted at Niigata University, Niigata, Japan (April 2019-March 2022), and included 10 CIPO outpatients and 10 healthy controls. Participants fasted for 12 hours and avoided high-fiber foods for 24 hours before testing. Glucose breath testing (50 g, institutional SOP) measured hydrogen (H₂) and methane (CH₄); positivity followed North American Consensus criteria (ΔH₂ ≥20 ppm by 90 min; CH₄ ≥10 ppm). The primary…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
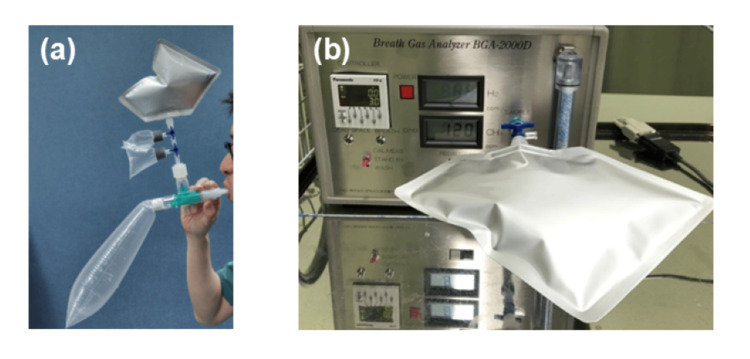 Figure 1
Figure 1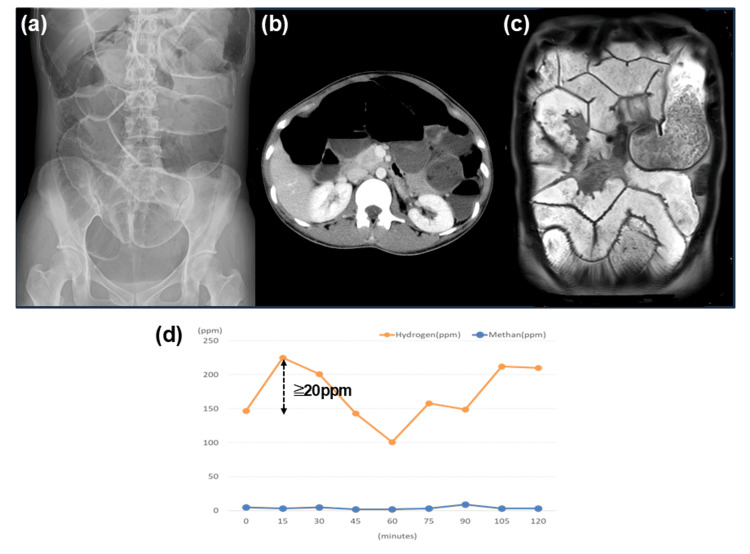 Figure 2
Figure 2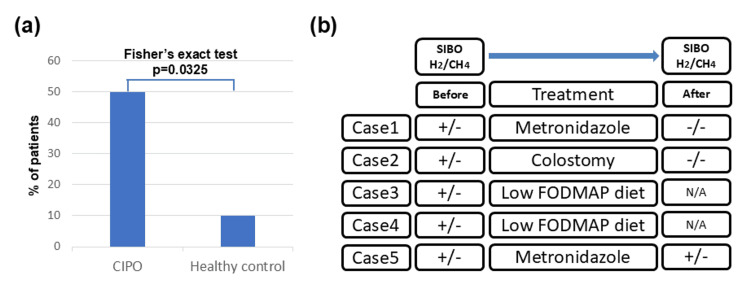 Figure 3
Figure 3| Case (No.) | Age (years) | Sex | BMI (kg/m2) | SIBO | ΔH2 (ppm) | CH4 peak value (ppm) | Primary complaint | Duration of illness (months) | CIPO | Affected area | Other diseases | Past abdominal surgery |
| 1 | 48 | F | 14.95 | + | 21.3 | 3 | Bloating, diarrhea, nausea | 10 | Secondary | Small intestine | Systemic sclerosis | None |
| 2 | 55 | F | 15.6 | + | 21 | 3 | Abdominal pain, bloating | 38 | Secondary | Colon | Familial Mediterranean fever | None |
| 3 | 72 | M | 13.3 | + | 105.7 | 3 | Abdominal pain, nausea | 113 | Secondary | Small intestine | Polymyositis | None |
| 4 | 62 | M | 16.3 | + | 96.4 | 1 | Abdominal pain, bloating | 18 | Secondary | Small intestine | Hashimoto disease | Appendectomy |
| 5 | 31 | F | 19.1 | + | 78 | 9 | Abdominal pain, bloating, diarrhea | 19 | Secondary | Small intestine | Pregnancy | None |
| 6 | 29 | M | 17.8 | - | 19 | 0 | Bloating, constipation | 6 | Primary | Small intestine | Autism spectrum disorder | None |
| 7 | 36 | F | 14.6 | - | -17 | 1 | Bloating | 21 | Primary | Colon | Pustular psoriasis | Colostomy (for CIPO) |
| 8 | 40 | F | 17.3 | - | -14 | 2 | Bloating, constipation | 88 | Secondary | Small intestine | Pregnancy | None |
| 9 | 61 | F | 17.7 | - | 2 | 0 | Bloating, constipation | 6 | Secondary | Small intestine | Schizophrenia | Colostomy (for cancer) |
| 10 | 47 | M | 22.4 | - | 8 | 1 | Bloating | 8 | Primary | Colon | Autism spectrum disorder | Colectomy (for CIPO) |
| Study (No.) | Authors | Study year | Country | Mode of diagnosis for SIBO | Measured gas type | Diagnostic criteria for SIBO | Patients with CIPO N | H2-SIBO in CIPO patients N (%) | CH4-SIBO in CIPO patients N (%) | Treatment /notes |
| 1 | Pérez et al. [ | 2014 | Chile | LBT | H2 | Original (described in the text) | 40 | 24 (60) | N/A | None |
| 2 | Lili et al. [ | 2017 | China | LBT | H2 | Rome Consensus | 9 | 7 (78) | N/A | FMT |
| 3 | Khan et al. [ | 2021 | USA | GBT | H2 and CH4 | North American Consensus | 38 | 9 (24) | 20 (53) | CH4 |
| 4 | Okubo et al. [ | 2024 | Japan | GBT | H2 | Rome Consensus | 12 | 8 (67) | N/A | RFX |
| 5 | Ours | 2025 | Japan | GBT | H2 and CH4 | North American Consensus | 10 | 5 (50) | 0 (0) | CH4, MNZ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal motility and disorders · Diet and metabolism studies · Gastroesophageal reflux and treatments
Introduction
Chronic intestinal pseudo‑obstruction (CIPO) is a rare, debilitating motility disorder first described by Dudley et al. in 1958 [1]. It is characterized by recurrent symptoms of intestinal obstruction without any mechanical cause. Although its pathophysiology remains incompletely understood, CIPO is increasingly recognized as a cause of chronic malabsorption and intestinal failure [2]. Severe impairment of gut motility predisposes to small intestinal bacterial overgrowth (SIBO), which can further exacerbate malnutrition and dysmotility [3,4].
Emerging evidence suggests an association between CIPO and SIBO [5]. A study from Chile reported a 60% prevalence of hydrogen‑positive SIBO in patients with CIPO [6]; however, methane was not assessed. Recent advances in breath testing enable simultaneous measurement of hydrogen (H₂) and methane (CH₄), gases with contrasting effects on intestinal motility. Excessive methane production has been linked to delayed transit, leading to the adoption of the term “intestinal methanogen overgrowth” (IMO) [7]. Despite these developments, data on the prevalence and clinical characteristics of SIBO subtypes (H₂‑SIBO vs. IMO) in CIPO remain scarce, particularly in Asian populations [8]. Furthermore, most prior studies have not systematically compared gas phenotypes or explored their clinical correlates.
Given these gaps, we aimed to determine the prevalence and phenotype distribution of SIBO in Japanese patients with CIPO using glucose breath testing (GBT) in accordance with North American Consensus criteria. We also sought to describe associated clinical features and interpret our findings in the context of existing literature.
This article was previously posted to the Research Square preprint server on July 2, 2025 (Version 1; DOI: 10.21203/rs.3.rs-6928176/v1).
Materials and methods
Study design and participants
We conducted a single‑center cross‑sectional study at Niigata University, Niigata, Japan (April 2019-March 2022). The Institutional Review Board approved the study protocol (approval no. 2019‑0226), and all participants provided written informed consent. The inclusion criteria were age ≥18 years and a diagnosis of CIPO according to national criteria [9], including radiologic evidence of bowel dilatation without mechanical obstruction. CIPO was classified as primary (idiopathic) or secondary (e.g., systemic sclerosis, drug‑induced, and pregnancy‑related). Ten outpatients with CIPO and 10 healthy controls (asymptomatic, no major comorbidities or gastrointestinal surgery) were enrolled. The study adhered to the Declaration of Helsinki and Japanese ethical guidelines for medical research.
Breath testing protocol
In this study, a breath test was performed to diagnose SIBO. For accurate diagnosis, bread, pasta, and noodles, which increase hydrogen production, were not allowed for 24 hours before the breath test. In addition, oral intake of water or tea was not allowed for 12 hours before the test. Regular medications were administered two hours before the test, if necessary, and participants were advised to avoid drinking, exercising, and smoking during this period. Oral rinsing was performed to avoid the metabolism of sugar substrates by oral bacteria. Breath measurements (hydrogen and methane concentrations) were performed three times before sugar substrate loading, and the average score was used as the baseline. Subsequently, breath measurements were performed every 15 minutes after loading and up to 120 or 180 minutes. The sugar substrate used was 50 g of glucose. Exhaled hydrogen and methane concentrations were measured using a BGA2000D instrument (Laboratory for Expiration Biochemistry Nourishment Metabolism Co., Ltd., Nara, Japan) (Fig. 1a, 1b).
Glucose breath test procedure and equipment for SIBO diagnosisa Actual breath test measurement scene. b Equipment required for SIBO breath testing. SIBO: small intestinal bacterial overgrowth
Diagnostic criteria and outcomes
According to the North American consensus [10,11], the following two diagnostic criteria for SIBO were used: a rise of ≥ 20 ppm from baseline in hydrogen by 90 minutes and a level of ≥10 ppm in methane. We have previously used these criteria to report the association between patients with cirrhosis and SIBO [12-14]. ΔH2 in Table 1 refers to the increase in hydrogen concentration from the baseline, and the CH4 peak value represents the highest methane concentration. Furthermore, cases with elevated hydrogen levels were defined as H-SIBOs, while those with elevated methane levels were defined as IMO, as previously reported [15]. In this study, both hydrogen- and methane-positive cases were included in the positive group for each sub-analysis. Exclusion criteria included recent antibiotic or probiotic use within four weeks, prior intestinal surgery (except colostomy), and severe comorbidities. No blinding was applied during data interpretation.
Statistical analysis
For data presented as proportions, 95% confidence intervals (CIs) were computed using the Clopper-Pearson exact method. The risk difference (RD) and its 95% CI were estimated using the Newcombe method (based on the Wilson score intervals). Risk ratios (RRs) were analyzed used the Katz log method; for zero cells, the Haldane-Anscombe continuity correction (0.5) was applied. Odds ratios (ORs) and 95% CIs used exact (Baptista-Pike) methods. Continuous variables are presented as the mean ± standard error, and categorical variables are expressed as counts and percentages. Given the small sample size (n = 10 per group) and zero cells, Fisher’s exact tests (two‑sided) were used for categorical comparisons, and Haldane-Anscombe continuity‑corrected odds ratios were calculated for zero‑cell tables. Mann-Whitney U tests were applied for exploratory comparisons of continuous variables, and U statistics with exact two-sided p-values are reported in the Results section. Statistical significance was set at p<0.05; however, results are interpreted cautiously due to limited power. Statistical analyses were performed using IBM SPSS Statistics for Windows, version 24.0 (IBM Corp., Armonk, N.Y., USA). An anonymized dataset and analysis templates are openly available to facilitate replication (DOI: 10.5281/zenodo.16910802).
Results
The study included 10 patients with CIPO, comprising four males and six females, with a mean age of 48.1 ± 13.6 years and a mean duration of illness of 32.7 ± 35.5 months. The mean body mass index (BMI) of patients with CIPO was 16.9 ± 2.5 kg/m², and eight of the 10 individuals were underweight (BMI < 18.5), according to the Japan Society for the Study of Obesity (Table 1). Conversely, the mean age and BMI of the healthy controls were 31.6 ± 4.2 years and 22.6 ± 2.5 kg/m², respectively. The characteristics of CIPO were secondary and primary in seven and three cases, respectively. The underlying diseases associated with secondary CIPO included systemic sclerosis (one case), familial Mediterranean fever (one case), polymyositis (one case), Hashimoto’s disease (one case), pregnancy (two cases), and schizophrenia (Clozapine drug-induced) (one case). The affected sites were the small and large intestines in seven and three cases, respectively.
Representative case
Abdominal radiographs, computed tomography, cine-magnetic resonance imaging (MRI), and breath test results for a representative case of CIPO are shown in Figure 2. This is a case of secondary intestinal pseudo-obstruction that developed in a 31-year-old woman after pregnancy and childbirth (case 5). The symptoms included abdominal pain, bloating, and diarrhea. Abdominal radiography revealed significant gaseous distension, predominantly in the small intestine. Abdominal radiographs and computed tomography demonstrated markedly dilated intestinal loops with air-fluid levels (Fig. 2a, 2b). Cine-MRI revealed small bowel dilatation and reduced peristalsis (Fig. 2c). A breath test confirmed the diagnosis of hydrogen-type SIBO, according to the North American Consensus (Fig. 2d).
Radiologic and functional imaging findings in CIPO with hydrogen-positive SIBO (case 5)a Abdominal radiograph: marked distension of the intestine by intestinal gas is observed. Small intestinal gas occupies the largest part. b Abdominal CT: markedly dilated intestinal loops and air-fluid levels are seen. c Cine-MRI: small bowel dilatation and reduced peristalsis are seen. d: A breath test confirmed the diagnosis of hydrogen-type SIBO according to the North American Consensus.SIBO: small intestinal bacterial overgrowth; CIPO: chronic intestinal pseudo-obstruction; CT: computed tomography; MRI: magnetic resonance imaging
In our study, hydrogen/methane breath testing showed that five of the 10 cases were SIBO-positive using the North American Consensus (six of the 10 using the Rome Consensus9), and all cases were associated with SIBO-phenotype hydrogen type. By contrast, when SIBO was measured in 10 healthy controls (male-to-female ratio 8:2, average age 31.6 ± 4.22 years, average BMI 22.7 ± 2.46, no symptoms, and no history of underlying diseases or surgery), only one case was diagnosed as having IMO, and no participant was diagnosed with hydrogen SIBO.
Primary outcome
Hydrogen-positive SIBO (H₂-SIBO) was observed in 5/10 patients with CIPO and 0/10 controls (Fisher’s exact test, two-sided p = 0.0325; continuity-corrected OR = 21, 95% CI: 1.8-243.8) (Fig. 3a). The risk difference was 50.0% (95% CI 11.7-76.3%), with an exact OR of 20.0 (95% CI 0.90-443.50) and an RR (Haldane-Anscombe adjusted) of 11.0 (95% CI 0.69-175.87). For overall SIBO (H₂ or CH₄), the prevalence was 5/10 vs. 1/10 (p=0.1409), with a risk difference of 40.0% (95% CI −0.24-67.59%), exact OR 9.0 (95% CI 0.81-100.14), and RR 5.0 (95% CI 0.70-35.50).
Prevalence of SIBO in CIPO and treatment flow for SIBO-positive patientsa Prevalence of overall SIBO (H₂ or CH₄) in patients with CIPO and healthy controls (Fisher’s exact test for H₂-SIBO; CIPO n = 10, controls n = 10). b Flowchart before and after treatment for SIBO-positive patients.SIBO: small intestinal bacterial overgrowth; CIPO: chronic intestinal pseudo-obstruction; FODMAP: fermentable oligosaccharides, disaccharides, monosaccharides, and polyols
Secondary outcomes
Overall SIBO (H₂ or CH₄ positive) occurred in 5/10 CIPO vs. 1/10 controls (p = 0.1409). No patient with CIPO met IMO criteria; one control was methane-positive. Baseline H₂/CH₄ values and full time-course data are provided in Zenodo (DOI: 10.5281/zenodo.16910802).
Among patients with CIPO, those with H₂-SIBO tended to have lower BMI (15.6 kg/m² vs. 18.0 kg/m²) and more frequent diarrhea (40% vs. 0%) than SIBO-negative patients, although these differences were not statistically significant; other symptoms (abdominal pain, bloating, nausea) were common in both groups.
Exploratory comparisons using exact Mann-Whitney U tests showed that ΔH₂ by 90 min tended to be higher in CIPO than in controls (median 20.0 ppm (IQR 3.5-63.8) vs 4.0 (2.3-4.8); U = 70.5, p = 0.130), whereas CH₄ peak did not differ significantly (1.5 (1.0-3.0) vs 1.0 (0.0-1.0); U = 68.5, p = 0.153). Within the CIPO cohort, H₂‑SIBO-positive patients had markedly higher ΔH₂ by 90 min (78.0 (21.3-96.4) vs 2.0 (-14.0-8.0); U = 25.0, p = 0.008) and higher CH₄ peak (3.0 (3.0-3.0) vs 1.0 (0.0-1.0); U = 23.0, p = 0.032), whereas age and BMI differences were not significant.
Treatment observations
These observations are anecdotal and interpreted cautiously. Of the five SIBO-positive patients, case 2 underwent colostomy, and cases 1 and 5 were treated with metronidazole, which improved their symptoms (Fig. 3b). After treatment, SIBO was measured, and two (cases 1 and 2) of the three patients tested negative. Cases 3 and 4 were treated with a low fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAP) diet; however, SIBO testing was not performed after treatment due to patient preference.
Discussion
To date, limited reports have examined the relationship between CIPO and SIBO (Table 2).
In 2014, Pérez et al. reported a 60% prevalence of SIBO in 40 patients with CIPO using the lactulose hydrogen breath test (LBT), although methane was not assessed and diagnostic criteria differed from current standards [6]. Lili et al. later reported a 78% prevalence using Rome Consensus thresholds [16,17]. However, the LBT has been criticized for overdiagnosis due to rapid colonic fermentation, and the North American Consensus currently recommends GBT with defined cutoffs (ΔH₂ ≥ 20 ppm by 90 min; CH₄ ≥ 10 ppm) [10,18].
Recent studies using GBT have yielded variable results. Khan et al. (USA) found IMO in 53% of patients with CIPO, whereas H₂‑SIBO was not significantly different from controls [8]. In contrast, Okubo et al. (Japan) reported a 67% prevalence of H₂‑SIBO using the Rome criteria but did not measure methane [9]. Our re‑analysis adds to this literature using North American Consensus criteria and exact statistics in a Japanese cohort. We observed that H₂‑SIBO was more frequent in CIPO (50%) than in controls (0%), while IMO was uncommon, contrasting with the US study where IMO predominated. These discrepancies may reflect methodological differences (substrate, cutoffs), constipation phenotypes, and cultural or dietary factors, as methane production has been linked to slow transit and constipation [19-21]. The single methane‑positive control in our study had recently returned from the UK, suggesting environmental influences.
Clinically, H₂‑SIBO‑positive patients tended to have lower BMI and more frequent diarrhea, consistent with the physiological effects of hydrogen‑producing flora. However, these associations are descriptive and hypothesis‑generating. Treatment observations (metronidazole response in two cases and dietary modification in others) are anecdotal and not generalizable; randomized trials are needed to define optimal therapy [22-24].
Limitations include the small sample size, single‑center design, and lack of blinding, which may limit generalizability. The glucose breath test may underestimate distal small bowel overgrowth. Age/BMI mismatch between groups and reliance on breath testing as an indirect measure also constrain interpretation. Nevertheless, this study provides the first combined assessment of hydrogen and methane in Asian patients with CIPO using consensus‑based GBT.
Conclusions
The findings of the present study suggest an association between CIPO and H₂‑SIBO in a Japanese cohort, while IMO was rare. However, these findings should be interpreted with caution given the small sample size, single-center design, and potential under-detection of distal overgrowth with glucose substrate. Further multicenter studies with larger cohorts and standardized protocols are warranted to confirm these observations. An anonymized dataset and analysis templates are openly provided to facilitate replication.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Intestinal pseudo-obstruction J R Coll Surg Edinb Dudley HA Sinclair IS Mc Laren IF Mc Nair TJ Newsam JE 20621731958 https://europepmc.org/article/MED/1351474413514744 · pubmed ↗
- 2Chronic intestinal pseudo-obstruction World J Gastroenterol Antonucci A Fronzoni L Cogliandro L 295329611420081849404210.3748/wjg.14.2953 PMC 2712158 · doi ↗ · pubmed ↗
- 3Advancement in the clinical management of intestinal pseudo-obstruction Expert Rev Gastroenterol Hepatol Lauro A De Giorgio R Pinna AD 197208920152502000610.1586/17474124.2014.940317 · doi ↗ · pubmed ↗
- 4Small intestinal bacterial overgrowth in patients with refractory functional gastrointestinal disorders J Neurogastroenterol Motil Shimura S Ishimura N Mikami H 60682220162655491610.5056/jnm 15116 PMC 4699722 · doi ↗ · pubmed ↗
- 5Gut microbial dysbiosis in the pathogenesis of gastrointestinal dysmotility and metabolic disorders J Neurogastroenterol Motil Singh R Zogg H Wei L Bartlett A Ghoshal UC Rajender S Ro S 19342720213316693910.5056/jnm 20149 PMC 7786094 · doi ↗ · pubmed ↗
- 6Sobrecrecimiento bacteriano intestinal y pseudoobstrucción intestinal crónica: una relación poco conocida Rev Chil Nutr Pérez de Arce OE Defilippi CC Madrid SA 257263412014 https://pesquisa.bvsalud.org/portal/resource/pt/lil-766592
- 7Methanogens, methane and gastrointestinal motility J Neurogastroenterol Motil Triantafyllou K Chang C Pimentel M 31402020142446644310.5056/jnm.2014.20.1.31PMC 3895606 · doi ↗ · pubmed ↗
- 8Chronic intestinal pseudo-obstruction is associated with intestinal methanogen overgrowth Dig Dis Sci Khan MZ Lyu R Mc Michael J Gabbard S 483448406720223500124110.1007/s 10620-021-07343-1 · doi ↗ · pubmed ↗