Hyperhomocysteinemia: An Unusual Cause of Budd-Chiari Syndrome
Sai Samhitha Mogalapu, Swathika T M, Keerthana P, Namicharan Nabirajan, Roshan Raj, Sahasyaa Adalarasan

TL;DR
A 52-year-old man with Budd-Chiari syndrome was found to have hyperhomocysteinemia as the rare underlying cause, highlighting the importance of considering this condition in diagnosis.
Contribution
The paper presents a rare case linking hyperhomocysteinemia to Budd-Chiari syndrome, emphasizing its diagnostic significance.
Findings
Elevated homocysteine levels were identified as the cause of Budd-Chiari syndrome in the patient.
Imaging and lab studies confirmed hepatic venous thrombosis consistent with BCS.
Anticoagulation therapy improved the patient's condition, underscoring the importance of timely diagnosis.
Abstract
Budd-Chiari syndrome (BCS) is a rare disorder caused by hepatic venous outflow obstruction, with clinical presentation ranging from asymptomatic disease to acute liver failure. We report a case of secondary BCS due to hyperhomocysteinemia in a 52-year-old male patient with a history of alcohol use. He presented with jaundice, vomiting, and melena. Examination showed icterus and tender hepatomegaly, while laboratory investigations revealed elevated liver enzymes. Doppler ultrasound and contrast-enhanced CT of the abdomen demonstrated caudate lobe hypertrophy, intrahepatic IVC and portal vein thrombosis, and non-visualization of hepatic veins, consistent with BCS. A hypercoagulable workup revealed elevated homocysteine levels, with other parameters within the normal range, confirming hyperhomocysteinemia as the underlying etiology. The patient was managed with anticoagulation, initially…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1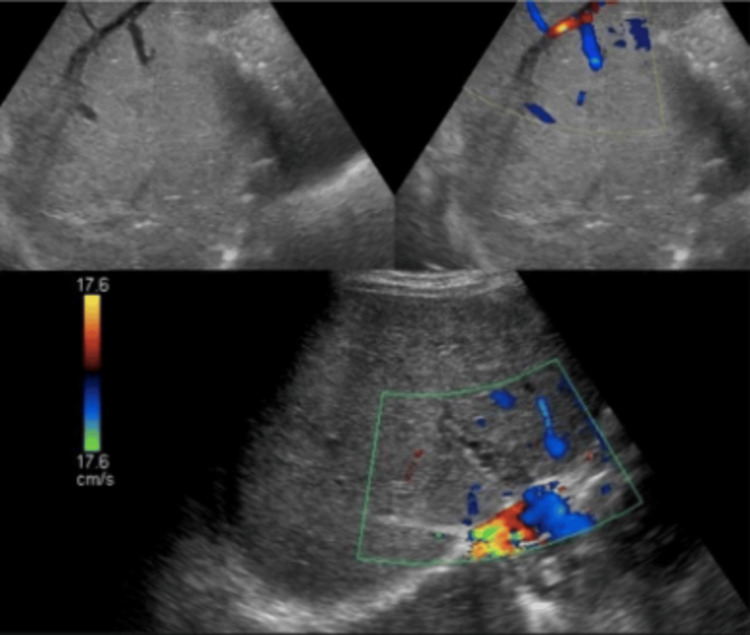 Figure 2
Figure 2| Lab Parameters | Values | Reference Range |
| Total leucocyte count | 8900 cells/mm3 | 4000 - 11000 |
| Red blood Cells | 3.4 million/ml | 4.5 - 6.5 |
| Hemoglobin | 8.5 g/dl | Dec-16 |
| Hematocrit | 32 | 40 - 46 |
| Platelets | 140,000/ml | 150,000 - 350,000 |
| MCV | 75.6 fL | 79 - 101 |
| MCH | 23 pg/cell | 27 - 33 |
| MCHC | 30 | 32 - 36 |
| Day | 1 | 3 | 5 | 6 | Reference Range |
| AST /ALT (IU/L) | 96/23 | 65/18 | 68/16 | 99/19 | 5-40/7-56 |
| ALP (IU/L) | 241 | 180 | 163 | 199 | 44-147 |
| TB/DB (mg/dL) | 9.6/4.2 | 12.5/11.0 | 10.0/7.1 | 13.2/11.6 | 0.3-1.2/0-0.3 |
| Total protein (g/dL) | 7.6 | 7.3 | 7.1 | 7.1 | 6-8.3 |
| Serum albumin (g/dL) | 3.1 | 2.9 | 2.3 | 3.0 | 3.5-5 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFolate and B Vitamins Research · Neurological Complications and Syndromes · Bone and Joint Diseases
Introduction
Budd-Chiari syndrome (BCS) has an incidence of 1 in 100000, making it a rare disorder [1]. It is caused by occlusion of the hepatic veins draining directly into the inferior vena cava. The obstruction of the venous architecture leads to venous hypertension. The most common lobe involved is the caudate due to its direct drainage into the inferior vena cava (IVC) [2]. The clinical features develop after the occlusion of two hepatic veins, which causes an increased interstitial fluid and liver congestion, resulting in hypoxic damage to the liver [3]. This results in the classic triad of jaundice, ascites, and tender hepatomegaly. The course can be acute or chronic and can be associated with portal hypertension. Portal vein thrombosis is observed in thrombophilic disorders [4]. The etiology is generally attributed to the myeloproliferative neoplasms, malignancy, infections, use of oral contraceptives, and hypercoagulable states secondary to inherited mutations in protein C, protein S, and factor V, antithrombin 3, which account for 80% of the cases; 20%, however, are idiopathic, and the cause is unidentified [2]. This is a case of hyperhomocysteinemia causing BCS, a rare often unidentified etiology.
Case presentation
A 52-year-old man presented with features of vomiting for four weeks associated with food particles and blood streaks in the vomitus, yellowish discoloration of the eyes for 10 days, and dark colored urine for 10 days with melena for two days. He is a known alcoholic, consumes about three drinks per week, and has been a smoker for over 20 years. On examination, the patient was icteric. Vitals were normal with a pulse rate of 82/ min, BP of 115/80mm Hg, afebrile status, and O2 saturation at 98% in room air. On examination, tender hepatomegaly with the liver edge felt 7 cm below the right costal margin moves with respiration, tender, and firm in consistency. There was no free fluid in the abdomen. Bowel sounds were present.
Investigations revealed microcytic hypochromic anemia with reduced platelet count (Table 1). Liver function tests showed elevated direct and indirect bilirubin (Table 2).
Stool occult blood was positive with negative viral markers, stool ova cyst negative, and normal serum AFP. Ultrasound abdomen with portal venous Doppler revealed grade 1 fatty liver with splenomegaly, hepatomegaly with coarse echos and caudate lobe hypertrophy; the intrahepatic branches of the portal vein showed evidence of thrombosis with the development of multiple intrahepatic collaterals (Figure 1). The CECT abdomen triple phase showed thrombosis at the intrahepatic portion of the IVC, with thrombosis of the portal vein, superior mesenteric vein, with caudate lobe hypertrophy (Figure 2).
Triple-phase CT of abdomen showing non-visualization of the hepatic veins in the portal venous phase
Ultrasound portal venous Doppler shows no color flow within the right and middle hepatic veins with a patent left hepatic vein. Turbulent flow noted within the intrahepatic IVC probably due to intrahepatic IVC thrombosis with features suggestive of Budd-Chiari syndromeIVC: Inferior vena cava
Esophagogastroduodenoscopy revealed the presence of portal hypertensive gastropathy. A diagnosis of BCS was hence made after ruling out other causes. The patient was further worked up for hypercoagulability. Serum homocysteine was found to be elevated. Serum vitamin B12 and methylmalonic acid levels were normal.
The patient was started on prophylactic antibiotics (1 g/day i.v. ceftriaxone for seven days). The patient was also started on 5000 IU (given twice daily) of heparin intravenously for seven days. The patient was instructed accordingly and discharged from the hospital.
Discussion
The etiology and presentation of BCS are varied [5]. The etiology for the same is quite varied and unpredictable; some rare causes that have been reported include COVID-19, polycythemia, pregnancy, etc. The presentation of BCS is different in adults and children. Primary BCS is most commonly seen in children, and secondary BCS is seen in adults. The most common presentation in children includes jaundice with hepatomegaly [6], while ascites occurs in adults [7]. The causes of secondary BCS include a malignant infiltration of the vein, compression of the vein by abscess, cyst, APLA, and the inflammation following this can also cause a procoagulant state, which leads to thrombosis. The causes of primary BCS are most commonly due to inherited thrombophilias [5,7]. The common causes of BCS secondary to thrombosis of the portal vein include protein S, protein C, and antithrombin 3 deficiency [5].
The investigation paved the way to narrow down the diagnosis, as the ultrasound investigation revealed a grade 1 fatty liver with splenomegaly with otherwise normal liver contour. To further investigate the presence of liver secondaries and gastrointestinal malignancies, a CECT abdomen was done, which revealed the thrombosis of the intrahepatic portion of the inferior vena cava with superior mesenteric vein thrombosis, along with caudate lobe hypertrophy. The diagnosis of Budd-Chiari syndrome was made, but the etiology had to be delineated. The absence of a mass obstructing the venous drainage was ruled out in the CECT. Based on the features in the imaging, one could come to the conclusion that the duration of the illness is subacute in nature due to the caudate lobe hypertrophy, presence of nodularity of the liver, non-visualization of the hepatic veins, and the development of intrahepatic collaterals [8]. The nodularity of the liver is attributed to the hemorrhagic necrosis of the parenchyma and compensatory volume expansion.
Furthermore, the presence of thrombosis gave direction towards the elevated procoagulant factors. The levels of ANA, beta 2 glycoprotein, anti-cardiolipin antibody (IgG/IgM), protein C, protein S, antithrombin 3, Factor V leiden, and serum homocysteine levels were evaluated. The values were normal for factors except serum homocysteine, which was elevated. In a study conducted to analyze the cause of BCS among West and China, the most common cause among the thrombophilic etiology was hyperhomocysteinemia, followed by cardiolipin antibodies [9]. High homocysteine levels are associated with an increased prothrombotic action because they enhance platelet activation, increase thrombin generation, argument factor V, and impair fibrinolytic activity. This is also associated with vascular injury and endothelial dysfunction [10].
The treatment of this disease can be surgical or medical management, depending on the etiology. The surgical options include shunting using mesocaval or mesoatrial shunts, orthotopic liver transplantation, and radiological shunting. The outcome of the patients varied depending on the treatment. In this case, the coagulation pathway dysfunction was hence managed by heparin 5000 IU intravenous and later bridged with warfarin from day 3 with a target INR range of 2-3. Serial INR was monitored weekly until stable values were reached, and then monthly INR monitoring was done.
Conclusions
BCS can present across all age groups with variable manifestations and carries a significant risk of mortality. It should therefore be considered as a differential diagnosis in patients presenting with abdominal pain, ascites, jaundice, or hepatomegaly. Early recognition and identification of the underlying cause of hypercoagulability are crucial for improving patient outcomes. In this case, timely diagnosis enabled effective management and a favorable clinical course.
Hyperhomocysteinemia, though uncommon, is an important and potentially overlooked etiology of secondary BCS. Incorporating homocysteine level assessment into the hypercoagulable workup is recommended. The patient discussed in the present case study highlights that prompt diagnosis through laboratory investigations and imaging modalities not only facilitates appropriate management but also significantly improves prognosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The diagnosis and management of the Budd-Chiari syndrome: consensus and controversies Hepatology Valla DC 7938033820031451286510.1053/jhep.2003.50415 · doi ↗ · pubmed ↗
- 2Budd-Chiari syndrome Stat Pearls [Internet] Hitawala AA Gupta V: Treasure Island (FL)Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 558941/32644367 · pubmed ↗
- 3Centrilobular and perisinusoidal fibrosis in experimental congestive liver in the rat J Hepatol Akiyoshi H Terada T 4334393019991019072610.1016/s 0168-8278(99)80102-0 · doi ↗ · pubmed ↗
- 4Oxidative stress produced by suprahepatic occlusion and reperfusion Hepatology Gonzalez-Flecha B Reides C Cutrin JC Llesuy SF Boveris A 881889181993840636410.1002/hep.1840180421 · doi ↗ · pubmed ↗
- 5The role of natural anticoagulant deficiencies and factor V Leiden in the development of idiopathic portal vein thrombosis J Clin Gastroenterol Egesel T Büyükasik Y Dündar SV Gürgey A Kirazli S Bayraktar Y 66713020001063621410.1097/00004836-200001000-00013 · doi ↗ · pubmed ↗
- 6Budd-Chiari syndrome in young Chinese: clinical characteristics, etiology and outcome of recanalization from a single center Cardiovasc Intervent Radiol Zhou WJ Cui YF Zu MH Zhang QQ Xu H 5575653920162681108810.1007/s 00270-016-1295-4 · doi ↗ · pubmed ↗
- 7Budd-Chiari syndrome in children: challenges and outcome World J Hepatol Samanta A Sen Sarma M Yadav R 117411871520233807500610.4254/wjh.v 15.i 11.1174 PMC 10698347 · doi ↗ · pubmed ↗
- 8Budd-Chiari syndrome: imaging review Br J Radiol Bansal V Gupta P Sinha S 201804419120183000480510.1259/bjr.20180441 PMC 6319835 · doi ↗ · pubmed ↗