Enterobius vermicularis as an Intraoperative Surprise in a Child With Suspected Appendicitis and Normal Laboratory Findings
Younis Al-Mufargi, Khadija Al Musalhi, Moayed Khalil, Mostafa Hamad, Abdulmalik Al-Atar

TL;DR
A child with suspected appendicitis had a parasitic infection instead, showing normal lab results and highlighting the need to consider parasites in diagnosis.
Contribution
This case report highlights the diagnostic challenge of Enterobius vermicularis mimicking appendicitis in children with normal inflammatory markers.
Findings
A child with suspected appendicitis had Enterobius vermicularis worms found during surgery.
Histopathology confirmed the presence of E. vermicularis without acute inflammation.
The patient recovered after antihelminthic treatment with albendazole.
Abstract
Acute appendicitis is a common surgical emergency in children, typically associated with elevated inflammatory markers and classical clinical presentation. However, parasitic infections such as Enterobius vermicularis can occasionally mimic appendicitis and represent a diagnostic challenge. Herein, we report a case of a nine-year-old female child who presented with right iliac fossa (RIP) abdominal pain and vomiting with normal white blood cell count and C-reactive protein (CRP) levels. Ultrasound imaging suggested early appendicitis, and therefore, a laparoscopic appendectomy was performed. Intraoperatively, multiple E. vermicularis worms were found within the appendiceal stump. Histopathological examination revealed no acute inflammation, but confirmed the presence of the E. vermicularis in the lumen. The patient recovered uneventfully and received antihelminthic therapy with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
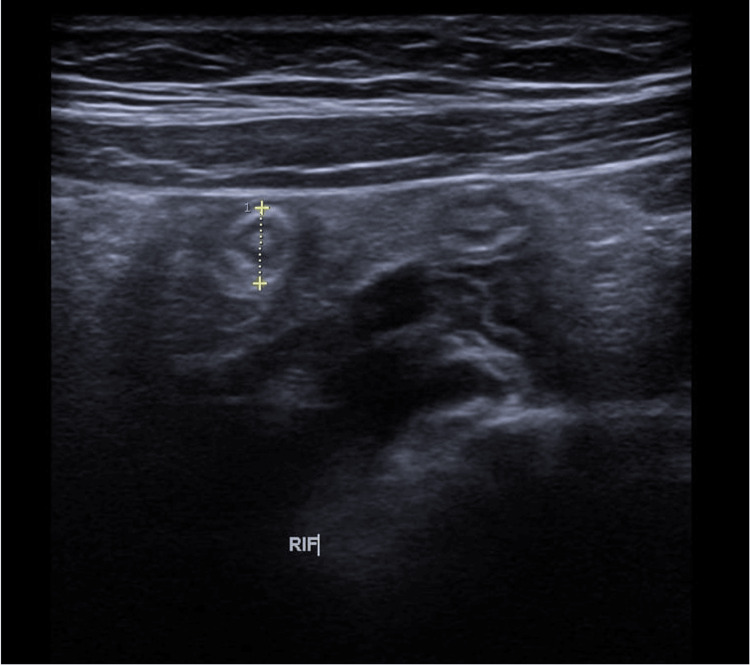 Figure 1
Figure 1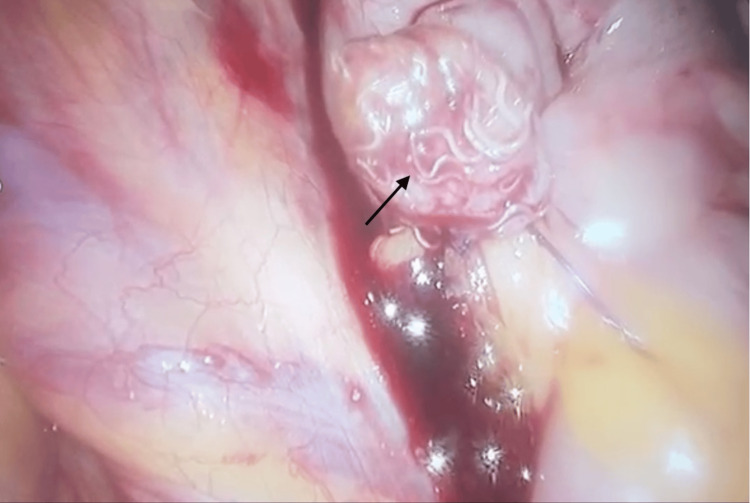 Figure 2
Figure 2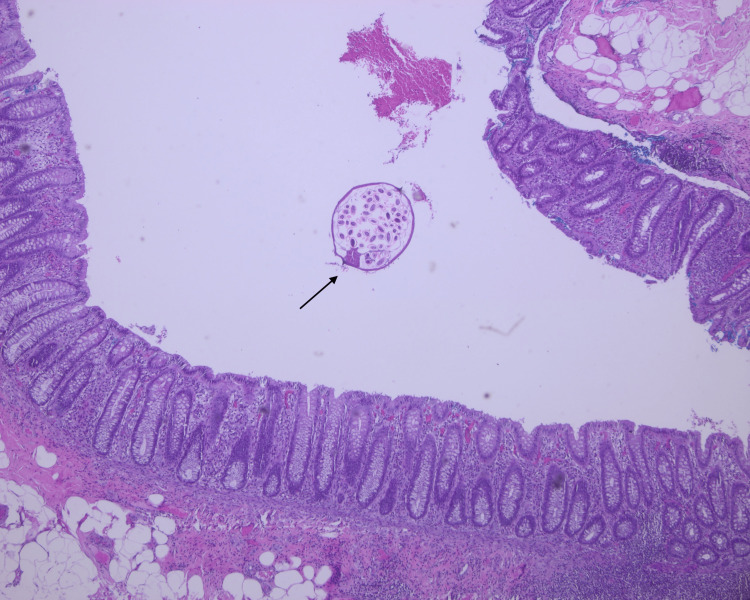 Figure 3
Figure 3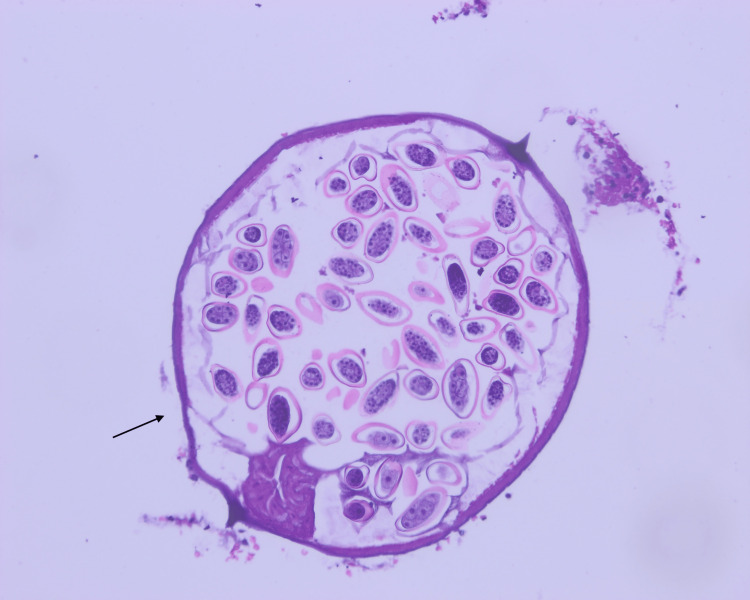 Figure 4
Figure 4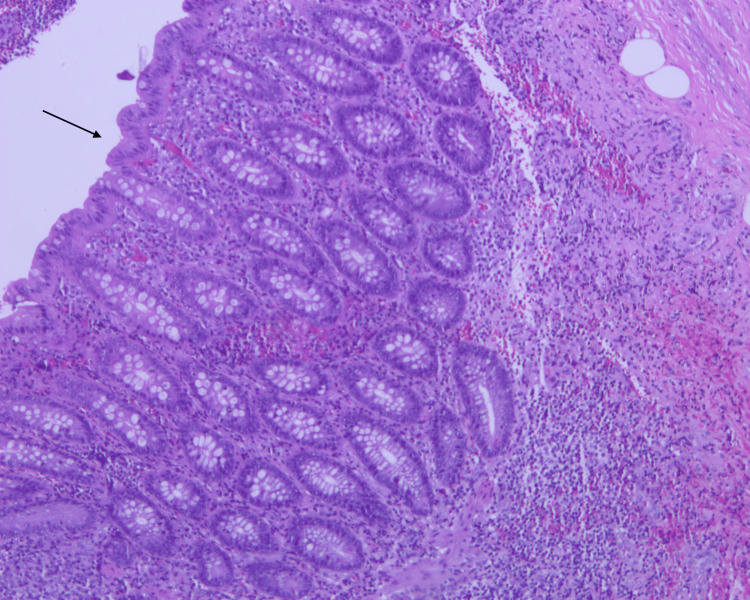 Figure 5
Figure 5| Laboratory test | Patient’s value | Normal range |
| CRP serum | 1.5 | 0.0-5.0 mg/L |
| WBC count | 4.44 | (4.50-14.50)×10⁹/L |
| Red blood cells | 5.89 | (3.90-5.30)×1012/L |
| Hemoglobin | 12.2 | 11.5-15.5 g/dL |
| Platelet count | 372 | (150-450)×10⁹/L |
| Neutrophils | 1.6 | (1.4-9.0)×10⁹/L |
| Lymphocytes | 1.9 | (1.9-9.8)×10⁹/L |
| Monocytes | 0.3 | (0.1-1.0)×10⁹/L |
| Eosinophils | 0.4 | (0.1-0.8)×10⁹/L |
| Basophils | 0.0 | (0.0-0.2)×10⁹/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAppendicitis Diagnosis and Management · Intraperitoneal and Appendiceal Malignancies · Intestinal Malrotation and Obstruction Disorders
Introduction
Acute appendicitis is a common surgical emergency, often caused by luminal obstruction due to fecaliths, lymphoid hyperplasia, or foreign bodies [1]. However, parasitic infections, particularly those caused by Enterobius vermicularis, commonly known as pinworms, represent an uncommon yet noteworthy etiology of appendiceal inflammation [2].
Among parasitic infections, E. vermicularis is the most widespread helminthic infection worldwide, especially prevalent among children aged five to 14 years [3]. The parasite is transmitted via the fecal-oral route, with female worms depositing eggs around the perianal region, typically resulting in nocturnal anal pruritus. While pinworm infection usually presents with benign and localized symptoms, its presence in the appendix has been associated with appendiceal pathology, although the precise pathogenic role remains controversial [4,5].
Diagnosing appendicitis secondary to* E. vermicularis* poses a clinical challenge. The clinical picture often mimics that of classical acute appendicitis, but inflammatory markers such as leukocyte count and C-reactive protein (CRP) may remain within normal limits [6]. Imaging modalities are often inconclusive, and in most cases, the definitive diagnosis is made intraoperatively or during histopathological examination of the resected appendix [7]. In some cases, the parasite is considered an incidental finding; in others, it is implicated as a causative agent in the inflammatory process [8]. While previous studies have debated the pathogenic role of* E. vermicularis*, few reports focus on cases where laboratory and imaging findings are inconclusive, underscoring the diagnostic uncertainty in such presentations. This report highlights an uncommon presentation of E. vermicularis in the appendix of a child with normal inflammatory markers, contributing to the ongoing debate about its role in appendiceal pathology.
Case presentation
A nine-year-old female with no significant past medical or surgical history presented to the Emergency Department (ED) in our hospital with a three-day history of progressively worsening abdominal pain. The pain was described as dull, initially periumbilical, and radiating to the lower abdomen, with increased severity at night and exacerbated by movement. The abdominal pain was associated with nausea, anorexia, and multiple episodes of non-bilious vomiting (three to four times on the day prior to admission). She also reported a single episode of diarrhea on the morning of presentation. There were no urinary symptoms.
In the ED, the patient received intravenous analgesia and antiemetics, which resulted in symptomatic relief. On physical examination, the abdomen was soft, with localized tenderness in the right iliac fossa (RIF) and suprapubic region. Rebound tenderness was present in the RIF. However, Rovsing’s sign was negative. Bowel sounds were audible, and both respiratory and cardiovascular examinations were unremarkable.
The patient was afebrile and hemodynamically within normal on arrival. Vital signs were as follows: temperature, 36.8°C; heart rate, 100 bpm; and blood pressure, 100/70 mmHg. Laboratory tests were within normal limits, including white blood cell count and serum CRP level, as shown in Table 1. Liver function tests, urea, and electrolytes were within normal limits.
Despite the clinical suspicion of appendicitis, laboratory findings, including normal CRP and borderline low WBC, did not support significant systemic inflammation, complicating the preoperative diagnosis.
Abdominal ultrasonography revealed a non-compressible and dilated appendix located in the RIF, anterior to the right iliac vessels (Figure 1). The appendix measured 6 mm at the base and 5 mm at the tip, with mild probe tenderness and adjacent free fluid findings consistent with early acute appendicitis.
Abdominal ultrasonography demonstrating a non-compressible, dilated appendix (6 mm diameter) located in the RIF, consistent with early acute appendicitisRIF: right iliac fossa
The patient underwent a laparoscopic appendicectomy. Intraoperatively, an inflamed appendix was identified. Following application of an endoloop and excision of the appendix, multiple parasitic worms were observed within the appendiceal lumen and stump (Figure 2). Suction and irrigation were performed to remove all visible worms. Additionally, an incidental left inguinal hernia was noted but did not require surgical intervention at this time.
Intraoperative view showing multiple Enterobius vermicularis (pinworms) emerging from the appendiceal stump following laparoscopic appendectomy, confirming the parasitic etiology
The patient made an uneventful recovery postoperatively and was discharged in stable condition. Empiric antihelminthic treatment with albendazole was initiated, which was administered in two doses, one week apart, as first-line therapy for suspected E. vermicularis (pinworm) infection. Family members received prophylactic treatment with the same antihelminthic agent.
Histopathology examination of the specimen (Figures 3, 4, 5) shows the appendiceal wall with relatively intact mucosa. The lamina propria was mildly expanded by increased lymphoid follicles and reactive germinal centers. The lumen contained E. vermicularis. There was no acute inflammation and no evidence of granuloma, dysplasia, or malignancy.
Histopathological examination of the appendix showing E. vermicularis infestationLow-power histopathological image of the appendix lumen containing multiple cross-sections of E. vermicularis (H&E, ×40), confirming parasitic infestation.
Histopathological examination of the appendix showing E. vermicularis infestationHigh-power histological view showing the characteristic morphology of E. vermicularis, including a thin eosinophilic cuticle and distinctive lateral alae (H&E, ×200).
Histopathological examination of the appendix showing E. vermicularis infestationMid-power histology reveals intact mucosa and mildly expanded lamina propria with reactive lymphoid follicles. No signs of acute inflammation or mucosal ulceration are seen (H&E, ×100).
The patient was followed up at one and four weeks postoperatively as an outpatient in pediatric surgery. At one week, a stool analysis was performed, which was normal following the second dose of albendazole. At four weeks postoperatively, there were no complications related to the surgical procedure.
Discussion
Appendectomy remains one of the most commonly performed surgical procedures in both pediatric and adult populations. The leading indication for this surgery is acute appendicitis, which typically arises from luminal obstruction due to fecaliths, appendicoliths, or lymphoid hyperplasia [9]. In a retrospective study conducted in Oman among pediatric and adolescent patients undergoing appendectomy for suspected acute appendicitis, parasites were found in 5.5% of cases. Among these, E. vermicularis accounted for 51.1%, followed by Schistosoma (9.1%), Ascaris lumbricoides (26.1%), Trichuris trichiura (8%), and* Taenia* saginata (5.7%) [10]. Parasitic infections as a cause of appendicitis are rare, with E. vermicularis (pinworm) being the most common cause in such cases.
The typical manifestation of pinworm infection is perianal pruritus, which occurs as gravid females migrate to the anal region at night to deposit eggs. While existing literature acknowledges the involvement of E. vermicularis in appendiceal inflammation, some patients exhibit clinical signs of acute appendicitis despite the absence of histological findings, which is known as "appendiceal colic" [11]. Our patient reflected a clinical presentation and imaging findings consistent with early acute appendicitis, yet histopathology revealed no acute inflammation. This underscores the complexity of establishing a causal relationship between *E. vermicularis *and true appendicitis. Nonetheless, E. vermicularis can still lead to varying degrees of appendiceal inflammation, ranging from uninflamed appendices to gangrenous or even perforated appendicitis [12]. In our case, despite the absence of raised inflammatory markers, including CRP, neutrophils, and eosinophils, clinical suspicion warranted surgical intervention. The diagnosis was ultimately confirmed intraoperatively when pinworms were visualized emerging from the appendiceal stump after excision. This finding supports the view that parasitic appendicitis cannot be reliably differentiated from other causes of appendicitis preoperatively [13].
Definitive diagnosis of E. vermicularis is typically made via the "cellophane tape" test, which detects characteristic eggs in the perianal region. In cases of high parasite burden, stool analysis may also reveal eggs or worms. Once diagnosed, treatment involves administration of anthelmintic agents such as mebendazole, albendazole, or pyrantel embonate. Our patient was treated successfully with albendazole and remained symptom-free following therapy [14].
Conclusions
E. vermicularis can mimic acute appendicitis in children, even in the absence of abnormal laboratory parameters or histological inflammation. In such cases, diagnosis is often confirmed only intraoperatively or through histopathological analysis. This case adds to the limited reports highlighting the diagnostic uncertainty caused by parasitic infections mimicking surgical emergencies. Clinicians should consider E. vermicularis in the differential diagnosis of pediatric RIF pain with atypical features. Early surgical intervention and appropriate antiparasitic therapy remain essential for definitive management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The global incidence of appendicitis: a systematic review of population-based studies Ann Surg Ferris M Quan S Kaplan BS 23724126620172828806010.1097/SLA.0000000000002188 · doi ↗ · pubmed ↗
- 2Enterobius vermicularis causing acute appendicitis, a case report with literature review Int J Surg Case Rep Hammood ZD Salih AM Mohammed SH 1531566320193158689210.1016/j.ijscr.2019.09.025PMC 6796714 · doi ↗ · pubmed ↗
- 3Enterobius vermicularis infection Gut Cook GC 11591162351994795921810.1136/gut.35.9.1159 PMC 1375686 · doi ↗ · pubmed ↗
- 4Appendicitis and Enterobius vermicularis Scand J Gastroenterol Wiebe BM 336338261991185315710.3109/00365529109025051 · doi ↗ · pubmed ↗
- 5Enterobius vermicularis infection among appendectomy specimens in Qom Province, central Iran: a retrospective study Comp Clin Pathol Mardani A Feizi F Fakhar M Beyranvand HB Farrokhi M Abbasi M Asfaram S 12131219262017
- 6Clinical manifestations of appendiceal pinworms in children: an institutional experience and a review of the literature Pediatr Surg Int Arca MJ Gates RL Groner JI Hammond S Caniano DA 3723752020041514132010.1007/s 00383-004-1151-5 · doi ↗ · pubmed ↗
- 7Enterobius vermicularis and its role in paediatric appendicitis: protection or predisposition?ANZ J Surg Lala S Upadhyay V 7177198620162699037510.1111/ans.13464 · doi ↗ · pubmed ↗
- 8The neglected role of Enterobius vermicularis in appendicitis: a systematic review and meta-analysis P Lo S One Taghipour A Olfatifar M Javanmard E Norouzi M Mirjalali H Zali MR 015202010.1371/journal.pone.0232143 PMC 717985632324817 · doi ↗ · pubmed ↗