Warm Autoimmune Haemolytic Anaemia Management in Asia‐Pacific: A Delphi Panel Expert Consensus and Systematic Literature Review
Phil Choi, Alberta Hoi, Rong Fu, Jun‐ho Jang, Yok Lam Kwong, Yoshitaka Miyakawa, Chi‐Chiu Mok, Hiroaki Niiro, Yasutaka Ueda, Robert Bagnall, Petya Kodjamanova, Da Eun Ahn, Nakul Saxena, Bryan Wahking, Shin‐Seok Lee

TL;DR
This study reviews the management of warm autoimmune haemolytic anaemia in the Asia-Pacific region and provides expert consensus on diagnosis and treatment.
Contribution
The paper presents a Delphi panel consensus and systematic review tailored to the Asia-Pacific region's unique challenges in wAIHA management.
Findings
Corticosteroids are used in over 80% of wAIHA patients with response rates of 81%–96%.
Restricted access to rituximab and gaps in physician awareness are key challenges in the APAC region.
Expert consensus recommends routine screening for underlying conditions and early interventions.
Abstract
This study aimed to assess the burden of warm autoimmune haemolytic anaemia (wAIHA) and treatment practices in the Asia‐Pacific (APAC) region. A systematic literature review (SLR) of observational studies in adult patients with wAIHA was conducted. Based on these findings, a Delphi panel was convened to develop consensus recommendations on diagnosis, treatment goals and algorithms by subtypes, unmet needs and research priorities. The SLR included 37 publications. Clinical guidelines consistently recommend direct antiglobulin testing for diagnosis and corticosteroids as first‐line treatment. Real‐world data showed corticosteroid use in over 80% of patients, with response rates of 81%–96%, and relapse rates of 18%–45%. The Delphi panel recommended routine screening for underlying conditions and early therapeutic interventions. Key challenges identified included restricted access to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
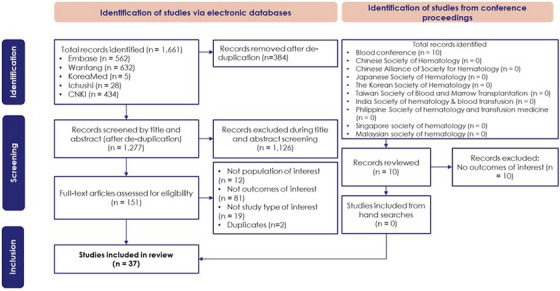 FIGURE 1
FIGURE 1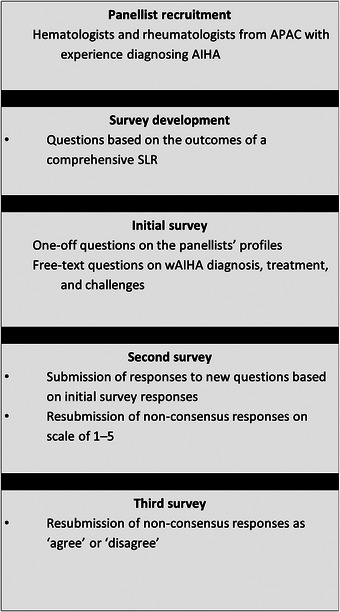 FIGURE 2
FIGURE 2| Criteria | Description |
|---|---|
| Population |
Adult patients with wAIHA. Subgroups of interest included, but were not limited to: Patients with primary wAIHA Patients with secondary wAIHA Patients with underlying conditions Patients with different disease severity |
| Interventions and comparators | No restriction (but precedence was given to pharmacological treatments) |
| Outcomes |
Data on the prevalence and incidence of wAIHA and subgroups of interest was targeted. However, where this was not available, the prevalence and incidence of AIHA was sought, and if possible/available, the proportion of patients with AIHA who were classified as wAIHA was noted. Data on the mortality outcomes of patients with w/AIHA was also targeted.
The burden of symptoms experienced by patients with wAIHA, the proportion of patients who were dependent on RBC transfusions, the morbidity experienced by patients and the risk factors associated with the development of wAIHA.
Patient burden as demonstrated via EQ‐5D, SF‐36, WHOQOL‐BREF, VAS, other relevant/identified scales or any other way of reporting patient burden.
The direct, including total, inpatient, outpatient and other direct costs, and indirect, including productivity losses, absenteeism and other indirect costs, costs and resource use associated with wAIHA and its management. |
| Study type | Observational studies, reviewsa (case reports, letters, and news articles were not included) |
| Language | Mandarin, English, Japanese, Korean |
| Publication date | Studies published since 2012 |
| Important screening tests aside from DAT | Proportion of panellists agreed |
|---|---|
| Assessment for possible underlying diseases (e.g., CLL, cancer, SLE, infection, drug use, other autoimmune diseases) | 89% |
| Blood smear with spherocytes | 89% |
| Rheumatoid factor test in patients who might have rheumatoid arthritis | 90% |
| Short‐term treatment goals for patients with wAIHA | Proportion of panellists agreed (%) |
|---|---|
| Improvement in blood count and increase Hb | 100% |
| Improve anaemic symptoms and tiredness | 100% |
| Stabilise Hb levels | 80% |
| Remission | 90% |
| The current challenges to diagnose wAIHA | Proportion of panellists agreed (%) |
|---|---|
| Steroid complications | 100% |
| Differential diagnosis in AIHA (wAIHA, CAD or mixed AIHA) is sometimes challenging, and Coombs‐negative wAIHA is often difficult to diagnose | 90% |
| Low disease awareness of physicians and patients. As some wAIHA patients have low antibody titres, more sensitive diagnostic tests are needed | 80% |
| Heterogeneity of disease manifestations | 80% |
| Lack of standardised guidelines | 100% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBlood groups and transfusion · Iron Metabolism and Disorders · Complement system in diseases
Introduction
1
Autoimmune haemolytic anaemia (AIHA), a rare disorder characterised by the destruction of erythrocytes due to autoantibodies, is typically diagnosed by the presence of haemolytic anaemia and a positive direct antiglobulin test (DAT). Using global data, the estimated incidence and prevalence of AIHA are 0.8–3 per 100,000 persons annually and 6–21 per 100,000 persons, respectively [1]. AIHA can be classified as either primary (idiopathic) or secondary to underlying malignancies, immunological disorders, infections or medications [2, 3, 4]. Uncontrolled AIHA is life‐threatening due to thromboembolisms, infections and other related causes [5]. The presentation and severity of AIHA depend primarily on patient comorbidities, functional status and immune system integrity, as well as underlying diseases [1, 6]. International guidelines recommend corticosteroids as the first‐line treatment for AIHA, and other immunosuppressive therapies and biologics, such as rituximab, as subsequent options [4].
Warm AIHA (wAIHA) is the most common AIHA subtype, accounting for 60%–80% of cases [2, 3]. It is characterised by the presence of immunoglobulin G (IgG) autoantibodies that are optimally active at 37°C. The condition predominantly affects females, has a median age of onset of 68.7 years, and is secondary in approximately 50% of cases [7], most often due to systemic lupus erythematosus (SLE) and other subtypes of connective tissue disease (CTD).
Despite its clinical importance, information on wAIHA in the Asia‐Pacific (APAC) region is limited. To address this, we conducted a systematic literature review (SLR) to evaluate the burden across epidemiological, clinical and economic dimensions, followed by a Delphi panel of APAC experts to build consensus on diagnosis, treatment and research priorities for the region.
Methods
2
Systematic Literature Review Methodology
2.1
The reporting of this SLR was guided by the Preferred Reporting Items for Systematic Review and Meta‐Analysis (PRISMA) [8].
Search Strategy
2.1.1
China National Knowledge Infrastructure (CNKI), MEDLINE, MEDLINE‐IN‐PROCESS, EMBASE, ICHUSHI, KOREAMED and WANFANG databases were searched for studies published from database inception to 12 October 2022 (the search date) using MeSH/EMTREE and free‐text terms (Tables S1–S5). The proceedings of relevant congresses (Table S6) and Google Scholar were searched for relevant abstracts and studies. The searches included combinations of: ‘waiha OR warm autoimmune haemolytic anaemia,’ ‘epidemiology,’ ‘socioeconomics,' and ’quality adjusted life year.
Study Selection
2.1.2
Duplicate records were removed using Zotero (Corporation for Digital Scholarship). Two reviewers independently screened titles and abstracts against pre‐defined eligibility criteria for inclusion (below). Full‐text articles assessed as potentially relevant during title and abstract screening were screened by two reviewers. At each screening step, differences were resolved by discussion with a third reviewer. A list of excluded studies with the reason for exclusion is presented in Table S7.
Pre‐defined study selection criteria are summarised in Table 1 according to the PICOS (Population, Intervention, Comparator, Outcome and Study type) framework [9]. Observational studies on the epidemiology or clinical, patient or economic burden of adult patients with AIHA or wAIHA in APAC countries published in Chinese, Japanese, Korean or English since 2012 were included. Reviews and clinical practice guidelines were also included for cross‐referencing.
Data Extraction
2.1.3
Data were extracted using a pre‐designed Microsoft Excel tabular summary, capturing publication details, study design, patient characteristics and outcomes related to epidemiology and clinical, patient and economic burden. Twenty percent of arbitrarily selected articles were reviewed by a third reviewer. Results from the SLR were analysed descriptively without statistical testing.
Delphi Panel Methodology
2.2
Rheumatologists and haematologists from APAC experienced in wAIHA management and proficient in English were recruited to participate in the Delphi panel. Candidate panellists were contacted sequentially in order from most to fewest peer‐reviewed publications until ten experts were enrolled. Panellists completed three rounds of anonymised electronic questionnaires (Appendix S2). Consensus for each question, predefined as ≥ 80% agreement, was assessed after each round [10].
Results
3
Systematic Literature Review
3.1
Characteristics of Identified Studies
3.1.1
The electronic search yielded 1661 records, of which 1277 were screened after removing duplicates. Following full‐text review of 151 articles, 37 studies were included (Figure 1). Most studies meeting the inclusion criteria were conducted in China (n = 26), with others performed in Japan (n = 4), India (n = 3), South Korea (n = 2), Thailand (n = 1) and Taiwan (n = 1) (Table S8). Clinical outcomes were most frequently reported (n = 25), followed by epidemiology (n = 13) and economic burden (n = 1); no studies addressed quality of life. Study designs included retrospective (n = 22), prospective (n = 10) and cross‐sectional (n = 1), and four studies with other designs.
PRISMA diagram.
AIHA Epidemiology and Mortality in APAC
3.1.2
Two studies reported population‐wide incidence/prevalence. In Japan, AIHA incidence is 1–5 per million and prevalence 3–10 per 1 million [11]. In Taiwan, incidence was 23.76 per 100,000 person‐years among people living with human immunodeficiency virus and 0.84 per 100,000 person‐years among age‐ and sex‐matched controls [12]. Most patients with AIHA were female (60%–79%) [13, 14, 15, 16, 17, 18, 19]. Predominantly, AIHA cases were classified as wAIHA (47%–95%) [11, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24] and were secondary (56%–90%) [16, 18, 21, 24, 25, 26], most commonly to cancer, infections, medications and autoimmune diseases [4, 25, 26, 27, 28, 29, 30, 31, 32]. Survival was generally good (70% 10‐year survival in Japan; 84% 5‐year survival in Taiwan) [31, 33], but worse in secondary AIHA and patients with DAT‐negative or IgA‐mediated AIHA [23, 31, 34]. Malignancies were the main cause of death among patients with secondary AIHA (55%) [31].
Diagnostic Testing
3.1.3
Our search strategy identified clinical practice guidelines from China, Japan and South Korea offering AIHA and wAIHA diagnostic recommendations [33, 35, 36]. Guidelines recommend diagnosing AIHA based on haemolytic anaemia and a positive DAT. Diagnostic indicators include low haemoglobin (Hb) and high reticulocyte count, bilirubin and lactate dehydrogenase (LDH). Guidance in China and Japan also includes low haptoglobin [33], and South Korea includes spherocytosis [36]. DAT is the primary recommended diagnostic test, with additional subtype‐specific tests including indirect antiglobulin test (IAT), cold agglutinin and Donath–Landsteiner (D‐L). In addition, guidelines in South Korea recommend enhanced DAT techniques to avoid false negatives [36].
Treatment Recommendations
3.1.4
Clinical practice guidelines from China, Japan and South Korea recommend corticosteroids as frontline AIHA and wAIHA treatment [33, 35, 36]. All guidelines provide splenectomy and immunosuppressive drugs (e.g., cyclophosphamide, azathioprine [AZA], vinblastine, danazol, cyclosporine A or mycophenolate mofetil [MMF]) as second‐line treatments. Guidelines from China and South Korea note rituximab as a second‐line option, while guidelines from Japan provide no specific recommendations for its use. Guidance from China notes that blood transfusions should only be given to patients with acute haemolytic anaemia and to patients with chronic anaemia with Hb < 50 g/L.
Treatment Patterns and Outcomes
3.1.5
Across the APAC region, frontline AIHA and wAIHA treatment has relied on corticosteroids. Almost all patients (> 80%) received corticosteroids, typically in the first line of treatment [16, 19, 25, 28, 31, 37], with 81%–96% initial response rates [17, 19, 31]. However, 18%–45% relapsed within a year [17, 31]. Second‐line treatments included immunosuppressants, rituximab, IVIG and occasionally splenectomy or plasmapheresis [16, 19, 25, 31, 37, 38]. Three studies reported that rituximab improved clinical outcomes versus corticosteroids, even at low doses [39, 40, 41]. Blood transfusions were commonly used (28%–60% in AIHA [16, 28, 42], 47.7–67.5% in wAIHA) [27, 29, 43], and were generally effective. Transfusions relieved anaemia with minimal adverse events [27, 44].
Clinical Burden
3.1.6
About 40% of patients with wAIHA had severe haemolysis, often due to delayed diagnosis. Most patients experienced fatigue, pallor, dyspnoea and dark urine [41, 45]. In another study, over half of the patients (55.1%) were transfusion‐dependent and some developed infections [39]. In the most recent study conducted in China, corticosteroid‐non‐responding patients with SLE‐AIHA receiving whole blood exchange alone had a shorter hospital stay (12.86 days) and lower costs (8147.77) [46]. Another study in China found that 16.7% (2/12) of patients with wAIHA experienced thrombosis and 50% (6/12) developed infections [37]. Thrombotic events are more common in AIHA due to factors such as free Hb from haemolysis, endothelial activation, inflammation and procoagulant microparticles [47, 48, 49]. Corticosteroids may further increase thrombotic risk, compounding the underlying prothrombotic state [50].
Delphi Panel
3.2
Ten experts (three rheumatologists and seven haematologists) from Japan (n = 3), Australia (n = 2), Hong Kong (n = 2), South Korea (n = 2) and China (n = 1) participated in the Delphi panel (Figure 2). Nine panellists completed the first two rounds, while all ten panellists participated in round three. All panellists had experience diagnosing AIHA, primarily in adult patients. Responses are summarised in Tables S11–S25, with consensus statements summarised in Tables 2, 3, 4. Statements for which consensus was not reached are summarised in Table S9, and statements where there was a consensus disagreement are summarised in Table S10.
Summary of Delphi process.
Diagnosis and Screening Practices
3.2.1
Panellists agreed that key tests for wAIHA diagnosis, supplemental to DAT, include screening for underlying diseases (e.g., cancer, including chronic lymphocytic leukaemia [CLL], infections, drug/medication use or autoimmune disorders, including SLE), spherocytes and rheumatoid factor to exclude rheumatoid arthritis (Table 2).
Persistent lymphadenopathy (> 1 cm), splenomegaly, cytopenia or monoclonal gammopathy should prompt evaluation for lymphoproliferative disease.
Interventions
3.2.2
Panellists agreed that intervention is warranted in cases with Hb < 10 mg/dL, severe anaemia symptoms or underlying wAIHA‐associated diseases (Table 3). Short‐term goals include stabilising Hb, improving anaemia symptoms and inducing remission. Long‐term goals span treatment cessation, quality of life improvement, symptom control, relapse prevention, reduced steroid burden and avoiding complications like infections or thrombosis.
Consensus was reached on the use of corticosteroids as first‐line wAIHA treatment, including 1 mg/kg prednisone daily for 3 weeks or 250–1000 mg IV methylprednisolone daily for 1–3 days. Panellists agreed that 40 mg dexamethasone for 4 days every 4 weeks should not be used as first‐line therapy. The most effective first‐line therapy in patients with wAIHA secondary to CTD is corticosteroids, steroids and MMF, while prioritising the treatment of the underlying CTD.
Second‐line treatments following corticosteroid failure are immunosuppressants, including cyclosporine at 2–5 mg/kg per day divided into two doses; AZA at 1–2 mg/kg/day divided into multiple doses; and rituximab at 375 mg/m^2^ once a week for 4 weeks or 1000 mg given twice, 2 weeks apart, with or without corticosteroids. Panellists agreed that second‐line treatments after relapse are the same as after failure, but enrolment in a clinical trial would be appropriate. Panellists agreed that third‐line options following treatment failure or relapse include splenectomy, immunosuppressants (MMF, cyclophosphamide and rituximab) and clinical trial enrolment. There was also agreement for the treatment options for later lines were rituximab, immunosuppressants, calcineurin inhibitors (CNIs), steroid pulses, a combination of corticosteroids and rituximab, and MMF. Panellists unanimously rejected the use of TNF‐α inhibitors in later lines.
Follow‐Up and Monitoring
3.2.3
Panellists reached consensus on several clinical indicators that could be used to ensure appropriate follow‐up and monitoring of patients with wAIHA: Hb, haptoglobin and LDH levels, and reticulocyte count (Table 3). Panellists also agreed that blood transfusion should be considered for patients with Hb < 7 g/dL or < 9 g/dL with comorbid ischaemic heart disease, severe symptomatic anaemia (e.g. Hb < 5–6 g/dL), severe anaemia refractory to corticosteroids, life‐threatening conditions, planned surgeries or severe complications. The need for transfusion may also vary depending on age and comorbidities, such as chronic heart failure.
Treatment Modifications
3.2.4
Clinicians should switch or enhance wAIHA therapy when patients do not respond, relapse, experience recurrence or complications, or would prefer to switch therapies (Table 3). Consensus indicators for a lack of response are transfusion dependence, no change in haematological parameters (Hb, LDH, reticulocyte count, etc.) over 4 weeks, and persistent symptoms of anaemia.
Comorbidities and Complications
3.2.5
Panellists reached consensus on several key strategies for managing the primary concerns related to comorbidities and potential complications associated with wAIHA (Table 3). Attending physicians should manage all complications appropriately, minimise steroid toxicities, reduce steroid use and consider early combination therapy with MMF or AZA. Panellists agreed that increasing Hb levels is important for heart failure management. Anti‐platelet medications may be prescribed to patients with thrombotic events such as brain infarction or ischaemic heart disease. Furthermore, attention should be given to adverse effects from glucocorticoids and immunosuppressants.
Diagnostic Challenges
3.2.6
Consensus was reached on current barriers to diagnosing patients with wAIHA, including low disease awareness of physicians and patients, heterogeneity of disease manifestations and lack of standardised guidelines (Table 4). While symptomatic anaemia is well‐recognised, differential diagnosis of AIHA subtypes, such as wAIHA, cold agglutinin disease (CAD) or mixed AIHA, can be challenging. DAT‐negative wAIHA is also often difficult to diagnose. Finally, more sensitive diagnostic tests are needed to diagnose wAIHA in those with low antibody titres.
Unmet Needs
3.2.7
Panellists reached consensus on three wAIHA treatment gaps that need to be addressed with currently available medications, including off‐label treatments: (i) approval for rituximab across the region, (ii) improved affordability of rituximab and (iii) formalisation of a wAIHA treatment algorithm based on high‐quality clinical trials. It was noted that the use of rituximab as an earlier line of treatment might reduce relapse rates, with rituximab being the only effective biological treatment available, highlighting a need for improved access to this therapy.
Challenges in the overall management of patients with wAIHA include the perception that steroids are the only effective treatment option and a lack of awareness among physicians about the side effects of prednisone and other steroids. Panellists also noted additional challenges, including drug reimbursement, uncertainty of the duration of maintenance immunosuppression, the unpredictability of relapse and the involvement of multiple teams in patient management leading to confusion. Overall, panellists agreed on the need for new therapeutic options, due to patients continuing to experience chronic fatigue and anaemia leading to low quality of life.
Research Priorities
3.2.8
Panellists agreed on the necessity for increasing awareness about wAIHA among healthcare professionals through the establishment of patient advocacy groups, medical advisory boards and scientific meetings. They also highlighted the importance of comparing guidelines with real‐world practice across countries, registering patients and utilising national insurance databases. Consensus was reached on key research priorities to address evidence gaps in the APAC region:
Optimisation of treatment strategies:
- Clinical trials comparing first‐ and second‐line therapies;
- Development of steroid‐sparing treatments and novel biologics to reduce reliance on splenectomy;
Long‐term outcomes and epidemiology:
- Studies on incidence and outcomes post rituximab;
- Research into poor prognostic factors, including comorbidities such as thrombosis and malignancy;
Patient‐centred outcomes
- Evaluating quality of life in patients with wAIHA.
Discussion
4
This study aimed to summarise the existing literature on wAIHA in the APAC region and to establish expert consensus on its diagnosis, treatment and management through a Delphi panel. The SLR identified 37 studies, most focusing on the clinical burden of AIHA and wAIHA, with limited and often outdated data on epidemiology and economic burden, suggesting that more population‐based studies are needed. Notably, no studies reported on quality of life, highlighting a significant gap in understanding the magnitude of the humanistic burden of wAIHA.
The SLR confirmed that wAIHA was the most common subtype of AIHA in the APAC region, with varying proportions of secondary AIHA. High mortality rates were reported, particularly among patients with secondary AIHA and those with underlying malignancies. Treatment guidelines from China, Japan and South Korea recommended corticosteroids as the first‐line treatment, with immunosuppressants and rituximab as second‐line options. Reported treatment patterns confirmed that these were the preferred treatments. However, the studies also showed that there were still differences in treatment for wAIHA, so there is a need for an evidence‐based prioritisation strategy that accounts for each patient's clinical status as well as the practical factors of drug availability, including approval status and reimbursement policy.
Though first‐line use of corticosteroids is initially effective at controlling wAIHA‐associated pathologies and is the approach recommended by clinical expert panellists, they are associated with severe side effects, including osteoporosis, diabetes, cardiovascular complications and increased susceptibility to infections [51, 52, 53]. Not only do these side effects reduce patient quality of life, they also contribute to overall morbidity and mortality [54]. Given these documented adverse effects, continued reliance on corticosteroids indicates an urgent need for new effective therapeutic options for wAIHA treatment.
Several established and novel agents are being investigated for their efficacy in treating wAIHA [55, 56, 57, 58]. Plasma cell‐targeting therapies that have recently undergone or are undergoing clinical trials in patients with wAIHA include parsaclisib, ibrutinib, rilzabrutnib, bortezomib, daratumumab, isatuximab, ianalumab, obexelimab and povetacicept. These agents could help control wAIHA by reducing the production of pathogenic autoantibodies. Beyond B‐cell–targeted therapies, the spleen tyrosine kinase (Syk) inhibitors fostamatinib and sovleplenib offer a strategy to disrupt signalling downstream of the Fc receptor, thereby limiting phagocytosis of antibody‐coated red blood cells. Similarly, blockade of the neonatal Fc receptor (FcRn) with nipocalimab, orilanolimab or batoclimab reduces recycling of pathogenic IgG autoantibodies, leading to decreased serum levels. Complement inhibition is also being actively explored, with agents such as the C3 inhibitor pegcetacoplan showing promise in preventing activation of the complement cascade and subsequent haemolysis. Collectively, these novel targeted therapies have the potential to shift the treatment paradigm in wAIHA by offering more precise, effective and safer alternatives to corticosteroids.
Rituximab has emerged as an effective second‐line treatment option for wAIHA, particularly in cases where corticosteroids fail or are not tolerated. Several studies included in the SLR demonstrated the efficacy of rituximab in improving clinical outcomes for patients with wAIHA. Despite its effectiveness, access to rituximab remains a challenge in some APAC countries due to high costs and a lack of approval. However, its use is associated with significant immunosuppressive effects, including an increased risk of infections, hypogammaglobulinemia and delayed immune reconstitution [59]. These concerns necessitate careful patient selection and monitoring when prescribing rituximab.
Strengths and Limitations
4.1
The strengths of the study include a comprehensive literature review that has identified key gaps in the existing research and an expert Delphi panel providing practical recommendations for wAIHA management. Although representatives from the most populous APAC regions were included, not all countries were represented, so the consensus statements might not fully apply to all countries based on differences in healthcare systems, diagnostic criteria and treatment availability.
Conclusion
4.2
This study highlights the need for evidence‐based, prioritised treatment guidelines that align with real‐world constraints. The SLR and Delphi panel have shown significant gaps in both the evidence base and current clinical practice, particularly concerning epidemiology, treatment outcomes and quality of life for patients with wAIHA. The resulting consensus recommendations provide a framework to improve diagnosis, treatment and overall disease management. Future research priorities include conducting large‐scale epidemiological studies, quality‐of‐life assessments, comparative clinical trials and the development of new treatment options to address these identified gaps and improve patient outcomes.
Author Contributions
B.W., N.S. and P.T. conceived the study. R.B., P.K. and D.A. developed the methodology and analysed the results. P.K. drafted the manuscript. All authors critically reviewed drafts and approved the final manuscript. The experts listed as authors on this manuscript provided input and support throughout the development of the Delphi panel process and contributed to the interpretation and contextualisation of the findings.
Funding
This study was sponsored and funded by Johnson & Johnson Innovative Medicine.
Ethics Statement
This work used previously published materials and did not involve human or animal participants; therefore, no ethics approval was required.
Conflicts of Interest
B.W., N.S. and P.T. are employees of Johnson & Johnson Innovative Medicine. P.K., R.B. and D.A. are employees of Amaris Consulting, which received funding from Johnson & Johnson Innovative Medicine for the study.
Supporting information
Table S1: Search terms for EMBASE and MEDLINE via www.embase.com on 12 October 2022. Table S2: Search terms for Wanfang via www.wanfangdata.com.cn on 12 October 2022. Table S3: Search terms for CNKI via www.kns.cnki.net on 12 October 2022. Table S4: Search terms for KoreaMed via www.koreamed.org on 12 October 2022. Table S5: Search terms for Ichushi via www.jamas.or.jp on 12 October 2022. Table S6: List of conference proceedings. Table S7: List of excluded citations. Table S8: Characteristics of included studies (n = 37). Table S8: Characteristics of included studies (n = 37). Table S9: Statements not reaching consensus. Table S10: Statements with consensus disagreement. Table S11: Summary of Delphi survey responses of part 1.1 Q1: what are the most important supplementary tests to consider during screening of patients, in addition to main test (direct antiglobulin test [DAT or Coombs test] to detect IgG + C3d or IgG) in current clinical guidelines? Table S12: Summary of Delphi survey responses of part 1.1 Q2: what are the optimal strategies for evaluating and addressing the underlying diseases that cause secondary wAIHA? Table S13: Summary of Delphi survey responses of part 1.2 Q1: how you determine when intervention is needed versus “watch and wait” (i.e. what factors should be considered for treatment initiation in wAIHA)? Table S14: Summary of Delphi survey responses of part 1.2 Q2: what are some of the preferrable treatment options in later lines (e.g., second line, third line, or after steroids) of therapy in patients with primary wAIHA? (Please specify dosing, frequency, and duration for each treatment)? Table S15: Summary of Delphi survey responses of part 1.2 Q3: what are the short‐term and long‐term treatment goals in patients with wAIHA? Table S16: Summary of Delphi survey responses of part 1.2 Q4: what are the most relevant clinical indicators that could be used to ensure appropriate follow‐up and monitoring of patients with wAIHA? Table S17: Summary of Delphi survey responses of part 1.2 Q5: in what cases should blood transfusion be considered for management in wAIHA, considering the potential challenges associated with alloimmunisation and delay of haemolytic reaction? Table S18: Summary of Delphi survey responses of part 1.2 Q6: treatment options and preferences in wAIHA per treatment line and after failure or relapse. Table S19: Summary of Delphi survey responses of part 1.2 Q7: regarding will the treatment options be affected by the underlying disease in cases of secondary wAIHA? What are the most effective treatment options in first line of therapy in patients with wAIHA secondary to connective tissue diseases (CTD)? What are the most effective treatment options in later lines of therapy in patients with wAIHA secondary to connective tissue diseases (CTD)? Table S20: Summary of Delphi survey responses of part 1.2 Q8: when to consider treatment switch or add‐on for patients with wAIHA? Table S21: Summary of Delphi survey responses of part 1.2 Q9: how do you manage the primary concerns in the management of comorbidities and potential complications associated with wAIHA, such as haemolysis‐related organ dysfunction or thrombotic events? Table S22: Summary of Delphi survey responses of part 2 Q1: what are the current challenges to diagnose wAIHA patients? Table S23: Summary of Delphi survey responses of part 2 Q2: what are the current gaps in the treatment of wAIHA that need to be addressed with current available options, including off‐label treatments (e.g., immunosuppressants, immunoglobulins, rituximab, etc.) in your country? Table S24: Summary of Delphi survey responses of part 2 Q3: what are the current challenges in or barriers to overall management of wAIHA patients? Table S25: Summary of Delphi survey responses of part 2 Q4: what potential further research and evidence generation approaches should be considered to address the evidence gaps in the published literature for wAIHA, specifically in the APAC region?
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1“Warm Autoimmune Hemolytic Anemia,” National Organization for Rare Disorders, last modified 30 July, 2024, https://rarediseases.org/rare‐diseases/warm‐autoimmune‐hemolytic‐anemia/.
- 2W. Barcellini and B. Fattizzo , “How I Treat Warm Autoimmune Hemolytic Anemia,” Blood 137, no. 10 (2021): 1283–1294.33512406 10.1182/blood.2019003808 · doi ↗ · pubmed ↗
- 3M. Michel , “Classification and Therapeutic Approaches in Autoimmune Hemolytic Anemia: An Update,” Expert Review of Hematology 4, no. 6 (2011): 607–618.22077525 10.1586/ehm.11.60 · doi ↗ · pubmed ↗
- 4U. Jäger , W. Barcellini , C. M. Broome , et al., “Diagnosis and Treatment of Autoimmune Hemolytic Anemia in Adults: Recommendations From the First International Consensus Meeting,” Blood Reviews 41 (2020): 100648.31839434 10.1016/j.blre.2019.100648 · doi ↗ · pubmed ↗
- 5D. L. Hansen , S. Möller , K. Andersen , D. Gaist , and H. Frederiksen , “Increasing Incidence and Prevalence of Acquired Hemolytic Anemias in Denmark,” CLEP 12 (2020): 497–508.10.2147/CLEP.S 250250 PMC 725028932547241 · doi ↗ · pubmed ↗
- 6S. S. Michalak , A. Olewicz‐Gawlik , J. Rupa‐Matysek , E. Wolny‐Rokicka , E. Nowakowska , and L. Gil , “Autoimmune Hemolytic Anemia: Current Knowledge and Perspectives,” Immunity & Ageing 17, no. 1 (2020): 38.33292368 10.1186/s 12979-020-00208-7PMC 7677104 · doi ↗ · pubmed ↗
- 7S. Tranekær , D. L. Hansen , and H. Frederiksen , “Epidemiology of Secondary Warm Autoimmune Haemolytic Anaemia—A Systematic Review and Meta‐Analysis,” JCM 10, no. 6 (2021): 1244.33802848 10.3390/jcm 10061244 PMC 8002719 · doi ↗ · pubmed ↗
- 8M. J. Page , J. E. Mc Kenzie , P. M. Bossuyt , et al., “The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews,” Bmj 372 (2021): n 71.33782057 10.1136/bmj.n 71PMC 8005924 · doi ↗ · pubmed ↗