Scapular Tuberculosis
Kenta Nakamoto, Shinnosuke Fukushima, Kohei Oguni, Hideharu Hagiya

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
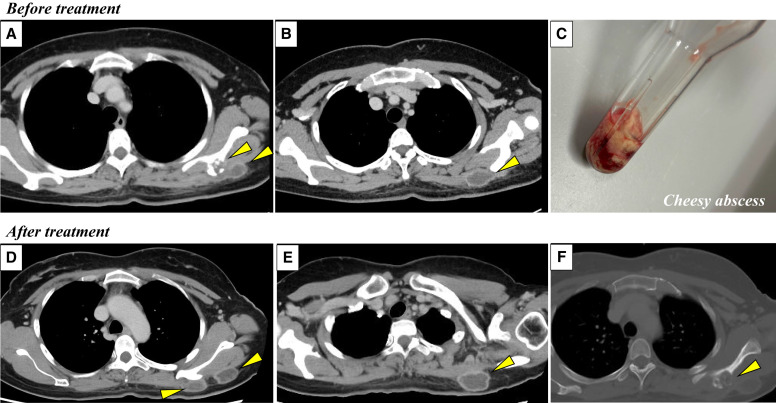 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Diseases and Tuberculosis · Orthopedic Infections and Treatments · Hematological disorders and diagnostics
A 44-year-old Filipino woman without remarkable underlying disease presented with progressive left shoulder tenderness that developed over several weeks. Radiological investigations revealed multiple abscess lesions measuring 25 mm, accompanied by osteolytic changes in the left scapula (Figure 1A and B). Laboratory investigations demonstrated positive results for interferon-gamma release assay, and Mycobacterium tuberculosis (TB) was isolated from the bacterial culture of an aspirated cheesy abscess (Figure 1C). Under the diagnosis of osteoarticular tuberculosis, the patient underwent standard multi-drug antitubercular therapy (Rifampin [450 mg/day], Isoniazid [300 mg/day], Pyrazinamide [1,300 mg/day], and Ethambutol [750 mg/day]). Four weeks later, she experienced increased tenderness and restricted range of motion in her left shoulder region, with imaging revealing enlargement of the TB lesions (Figure 1D–F). Surgical intervention with local incision and drainage yielded caseous material, after which the patient demonstrated clinical improvement. Mycobacterial culture of the specimen was negative, suggesting a paradoxical inflammatory response rather than treatment failure of anti-TB therapy.
This case exemplifies the diverse manifestations of M. tuberculosis. Osteoarticular involvement occurs in approximately 2% of all TB patients, representing an uncommon but clinically significant extrapulmonary manifestation of the ubiquitous pathogen.1 Spinal involvement constitutes the predominant presentation of the osteoarticular TB infection, while shoulder joint infection is exceedingly rare,2^,^3 and reported in <2% of all osteoarticular TB cases.1 Patients with osteoarticular TB infection manifest only nonspecific clinical symptoms, and making a definite diagnosis is challenging.4
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Banshelkikar SP Tandon N., 2022. Scapula abscess secondary to shoulder tuberculosis: Case report with review of literature. J Orthop Case Rep 12: 74–77.10.13107/jocr.2022.v 12.i 06.2872 PMC 1009240437065510 · doi ↗ · pubmed ↗
- 2Sharma BK, , 2013. Scapular bone destruction: Do not forget to think of tuberculosis in endemic areas. BMJ Case Rep: bcr 2013200051.10.1136/bcr-2013-200051 PMC 373668123833009 · doi ↗ · pubmed ↗
- 3Idsaid K, , 2024. Tuberculous osteomyelitis of the scapular spine revealing HIV-1 infection. Trop Med Infect Dis 10: 8.39852659 10.3390/tropicalmed 10010008 PMC 11769330 · doi ↗ · pubmed ↗
- 4Jagtap SA Sonawane DV Saraogi AA, 2013. Isolated tuberculosis of scapula in a young adult. Int J Mycobacteriol 2: 11–47.10.1016/j.ijmyco.2013.03.00426785899 · doi ↗ · pubmed ↗