Recurrent Sigmoid Volvulus in Pregnancy: Case Report
Hayte M. Samo, Martini Gemuwang, Fides Canuty, Joshua G. Gidabayda, Emanuel Q. Nuwass

TL;DR
A pregnant woman experienced a rare condition called sigmoid volvulus twice, requiring surgery for a successful recovery of both mother and baby.
Contribution
This case report highlights the management and successful surgical intervention of recurrent sigmoid volvulus during late pregnancy.
Findings
A 33-year-old pregnant woman at 32 weeks gestation was diagnosed with recurrent sigmoid volvulus.
Surgical resection of the redundant sigmoid colon led to a favorable outcome for both mother and fetus.
Timely diagnosis and multidisciplinary surgical intervention are crucial in managing sigmoid volvulus during late gestation.
Abstract
Sigmoid volvulus in pregnancy is a rare condition occurring during the third trimester with a high recurrence rate and having fatal complications to both fetus and mother. It requires a prompt diagnosis and multidisciplinary approach. We present a case of a 33 year old, pregnant woman, Gravida 4, Para 3, at 32 weeks of gestation, who presented with abdominal pain, distension, and tenderness. A Plain abdominal X-ray showed a dilated loop of the sigmoid colon. This was her second admission with similar symptoms. Having previously diagnosed with sigmoid volvulus one month earlier, she was treated conservatively, recovered, and discharged. On this admission she was diagnosed with recurrent sigmoid volvulus, after stabilization she underwent laparotomy which revealed sigmoid colon volvulus at 180 degrees twist. A resection of redundant sigmoid was done, resulting in uneventful postoperative…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 FIGURE 1
FIGURE 1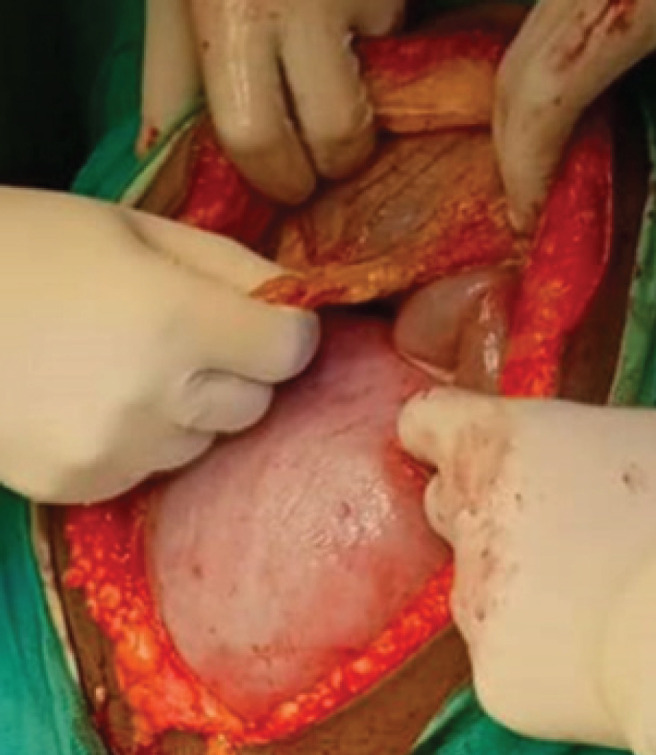 FIGURE 2
FIGURE 2 FIGURE 3
FIGURE 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntestinal Malrotation and Obstruction Disorders · Appendicitis Diagnosis and Management · Pediatric Hepatobiliary Diseases and Treatments
BACKGROUND
Sigmoid volvulus during pregnancy is a rare but serious condition that can lead to significant maternal and fetal complications if not diagnosed and treated promptly. In pregnancy, the enlarging uterus displaces abdominal organs, which may increase the risk of volvulus. Reported incidence of sigmoid volvulus ranges from 1:66,431 to 1:1500 pregnancies.^1^ Most cases occur in the second or third trimester due to increased intra-abdominal pressure and anatomical shifts.^1,2^ Pregnancy can mask classic signs of bowel obstruction, and poses diagnostic and management challenges especially in low-resource settings.
Commonly reported symptoms include abdominal pain, distention, constipation, and vomiting when complicated by peritonitis abdominal tenderness may be present.^3^ The condition being rare requires various modes of treatment according to gestational age.^2^
Timely diagnosis is critical in management of sigmoid volvulus. When diagnosis is delayed beyond 48 hours there is high risk of mortality and morbidity to both the mother and the fetus.^4^ The diagnosis requires high index of suspicion and multidisciplinary team including a general surgeon, obstetrician, pediatrician, and radiologist. Radiological investigation plays a key role as a plain abdominal X-ray may reveal a typical sign such as an inverted U-shaped colonic gas pattern, a coffee bean-shaped appearance and whirl sign. However, fear of radiation exposure to fetus may delay radiologic imaging.^3^
MRI is the preferred radiological investigation due to its safety profile, but CT scan may be considered when there is no MRI.^5^
The treatment depends on gestation age and the presence of peritonitis. At any gestation age, suspected peritonitis and gangrene, warrants emergency explorative laparotomy. In term pregnancy cesarean section may be performed with resection in the same sitting. In early gestation conservative management may be tried with administration of dexamethasone to enhance the fetus lung maturity.^6^
During both the first and second trimester and if there is no sign of peritonitis, enema and rectal tube decompresion can be considered. In the third trimester, sigmoid colectomy is indicated especially if there is peritonitis and gangrene. The non-recurrent sigmoid volvulus with no peritonitis or gangrene may be managed conservatively to promote fetal maturity.^2^ If surgery is indicated in the absence of gangrene, a resection with an end-to-end anastomosis is safe, alternatively in presence of gangrene stoma can be raised and closed in intervals of 2 to 3 months.^6^ There is a need to increase awareness among the healthcare practitioners to enhance their capability on timely diagnosis and intervention of this life-threatening condition.
CASE PRESENTATION
A 33-year-old pregnant woman, gravida 4, para 3, at 32 weeks gestation age from Iramba district in Singida region, presented with generalized abdominal pain, distension, and constipation for three days with two episodes of vomiting. She was admitted at Haydom Lutheran Hospital in September 2023. During the admission there was no vaginal bleeding or amniotic fluid leakage. She had the same presentation two months prior, and she was managed conservatively, with Nasogastric tube decompression and IV fluids. She improved and discharged a few days later after passing stool and flatus with no abdominal pain.
On the second admission, she had a recurrent painful markedly distended abdomen, and tenderness, making it difficult to assess fundal height. On examination she had stable vitals, with blood pressure of 124/82 mmHg, Heart rate of 71 beats per minute, respiratory rate of 23 cycles per minute, temperature of 37°C, and on abdominal examination, she had a tender grossly distended abdomen, with palpable gravid uterus. Fundal height was estimated to correspond to gestational age of 32 weeks. The Abdomen was hyper tympanic with exaggerated bowel sounds. Rectal examination revealed an empty rectum and no mass. Her laboratory findings revealed stable electrolytes serum potassium 4 mmol/L, blood glucose of 85 mg/dL. Full blood picture with white blood cell count of 6000, Hemoglobin of 14 gm/dL. The provisional diagnosis of acute intestinal obstruction was made by the team. Following the decision of diagnosis, the dexamethasone 4 mg was initiated, however only received two doses as the patient was operated before she finished the four doses due to worsening clinical condition.
Initial management included Nil per oral (NPO), Nasogastric tube decompression, IV fluid, and urethral catheterization. Initial investigations included abdominal Ultrasound complete blood picture and electrolytes panel.
Ultrasound revealed a live single intra uterine fetus in a cephalic position with adequate amniotic fluid. Multidisciplinary team including a general surgeon, an obstetrician, and a pediatrician approved a plain abdominal X ray which revealed a bean shaped colonic distention (Figure 1).
Abdominal Radiograph
The diagnosis of acute intestinal obstruction was reached, due to recurrent sigmoid volvulus. Saline enema was initiated which was unsuccessful, as abdominal distension and pain persisted and worsened. Emergency exploration laparotomy was planned after counselling and obtaining the consent form for emergency surgery. The patient was prepared for emergency explorative laparotomy which was performed under general anesthesia. A midline incision was performed by a general surgeon assisted by an obstetrician who performed hysterotomy for baby extraction. There was a pediatrician in the operating room to assist in case of fetus prematurity (Figure 2). The intra operation revealed a sigmoid volvulus which was rotated at its axis at 180 degrees with a long and distended viable loop (Figure 3). A hysterotomy was done and a female baby was extracted weighing 1750 Kg. The baby scored 5, 8, and 9 at 1^st^, 2^nd^ and 3^rd^ minutes respectively.
Demonstrates Gravid Uterus just after Midline Incision
Dilated Loop of Sigmoid Colon
The baby was admitted to the neonatal intensive care unit (NICU). The sigmoidectomy was done and end-to-end anastomosis was performed. The patient was admitted to an intensive care unit (ICU) and administered with intravenous fluids, antibiotics and analgesia parenterally for 24 hours then started on ambulation while the baby was admitted in neonatal unit (NICU) for close monitoring and later the mother was discharged to the maternity ward, where she awaited her baby, who was under pediatricians and neonatal nurses care. Three weeks later, the mother and the child who had achieved 1930Kg were discharged home following uneventful post-operative recovery. Follow-up was extended for one year, and during this period, both mother and her child were progressing well.
DISCUSSION
Recurrent sigmoid volvulus is a very rare cause of intestinal obstruction in pregnancy,^7^ with increased incidence during the third trimester^8^ and it is associated with life-threatening fetal and maternal complications. Pregnancy is a precipitating factor for sigmoid volvulus, as the enlarged gravid uterus in late gestation displaces a redundant or abnormally long sigmoid colon out of the pelvis and twists around its point of fixation where gravid uterus hinders spontaneous untwisting.^8 10^ There are varied clinical presentations of sigmoid volvulus in pregnancy where most of these cases present with abdominal distension, pain, and constipation.^10 11^ This patient presented with the above symptoms and had, in addition, vomiting and abdominal tenderness on deep palpation but without fever.
The diagnosis of sigmoid volvulus in pregnancy at an advanced gestation age is challenging as its presentation can be confused with pregnancy associated complaints.^8^ A high index of suspicion for sigmoid volvulus is required whenever a pregnant woman in her third trimester presents with a triad of abdominal pain, distension, and absolute constipation.^12^ The controversy over imaging options for pregnant mothers pose a diagnostic dilemma, as different literatures recommend that exposure of pregnant mothers to radiation, like X-rays and CT scans of the abdomen, should be avoided.^4^ Meanwhile, other literature reports that MRI is the recommended option, because of its better diagnostic accuracy and safety for the fetus.^6 13 14^ The MRI was the best option for radiological diagnosis for this patient due to absence of radiation risk to fetus however it was not available in our facility. For this case, we had to proceed with a plain abdominal X-ray, which effectively revealed dilatation of the large bowel.
The management approach of sigmoid volvulus in the pregnant patient does not deviate from that of the non-pregnant patient. It involves aggressive resuscitation with intravenous fluid, placement of the nasogastric tube for decompression, and endoscopic reduction of the volvulus. And when this fails, surgery is the definitive option. ^8 15^ Several case reports have shown good results in using endoscopic distortion and rectal tube decompression of sigmoid volvulus during pregnancy where bowel necrosis or vascular occlusion has been ruled out.^16^ In the absence of signs and symptoms of peritonitis, it is reasonable to attempt untwisting and decompression by placement of a soft rectal tube or colonoscopy or sigmoidoscopy.^3,17,18^ The presence of abdominal tenderness and grossly dilated sigmoid colon, in our case, it was a contraindication for the use of endoscopic reduction. The other management option includes a saline enema, which in this case was attempted, but it was unsuccessful, and therefore, the patient proceeded to laparotomy as one of the surgical treatments for cases in which conservative management has failed.^19^
This patient had an extremely dilated sigmoid colon twisted at 180 degrees without gangrene, while in other cases a gangrenous and perforated sigmoid loop were intraoperatively found.^10^ In other cases with peritonitis and perforations, the stoma may be raised and later can be closed after a period of 2 to 3 months.^6,13,14,20^ The anticipated complications include maternal and fetal mortality meanwhile maternal mortality occurs at 5% when the bowel is viable and increases to 50% when there is bowel perforation.^21,22^ The other post-operative complications reported are sepsis and anastomotic leak which are also associated with a high risk of fatal complication to the fetus and the mother.^22^ In our case, caesarean section was performed during laparotomy.
CONCLUSION
Recurrent sigmoid volvulus in pregnancy is a rare condition that has a high risk of recurrence, and its prompt diagnosis requires a high index of suspicion with the involvement of a multidisciplinary team. The timely diagnosis, management, and surgical intervention are critical following its recurrence at a late gestational age due to favorable outcomes for the baby and mother.
CONSENT
A written informed consent was voluntarily obtained from the patient for publication of this case report and any accompanying images while maintaining anonymity. A copy of the written and signed consent is available for review.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ghahremani S, Parisa Razmjouei, Parvaneh Layegh, et al. A Case of Sigmoid Volvulus in Pregnancy: A Rare Emergency in Pregnancy. International journal of pediatrics. 2020;8(1):10743–10747. doi: 10.22038/ijp.2020.45675.3734 · doi ↗
- 2Alshawi JS. Recurrent Sigmoid Volvulus in Pregnancy: Report of a Case and Review of the Literature. Diseases of the Colon & Rectum. 2005;48(9):1811–1813. doi: 10.1007/s 10350-005-0118-515991065 · doi ↗ · pubmed ↗
- 3Shaw WZ, Huang CF, Hung TY, Yeh YH. Typical Whirl Sign in Sigmoid Volvulus. ˜The oe Journal of emergency medicine/˜The oe Journal of emergency medicine (Sl Online). 2014;46(3):383–384. doi: 10.1016/j.jemermed.2013.09.01724412055 · doi ↗ · pubmed ↗
- 4Khan MJ, Farid N, Rafique AM, Gul B, Khattak IU. Gangrenous Sigmoid Volvulus in a Complicated Pregnancy: An Alarming Obstetric and Surgical Stigmata. SAJ Case Reports. 2018;5(2):1–5. doi: 10.18875/2375-7043.5.202 · doi ↗
- 5Watanabe T, Kinjo T, Yoshino Kinjyo, et al. Sigmoid Volvulus in Pregnancy Assessed by Contrast-Enhanced Computed Tomography Scanning. Case reports in obstetrics and gynecology. 2021;2021:1–4. doi: 10.1155/2021/6692483 PMC 795217633747587 · doi ↗ · pubmed ↗
- 6Tesnière M, Arnoult A, Roger N. Sigmoid Volvulus in Pregnancy. ˜The oe Journal of emergency medicine/˜The oe Journal of emergency medicine (Sl Online). 2018;54(6):e 129–e 131. doi: 10.1016/j.jemermed.2018.02.03829681418 · doi ↗ · pubmed ↗
- 7Tarik Souiki, Tayeb Ouazzani, Alami B, et al. Sigmoid volvulus in pregnancy. Formosan journal of surgery. 2022;55(6):225–228. doi: 10.4103/fjs.fjs_102_22 · doi ↗
- 8Esra DİŞÇİ, Rıfat PEKSÖZ, Kara S, Sabri Selcuk ATAMANALP. Sigmoid volvulus in pregnancy: Current approach in diagnosis and treatment. Journal of surgery and medicine. 2022;6(3):243–245. doi: 10.28982/josam.1072519 · doi ↗