Severe Iron-Deficiency Anemia due to Hookworm Hyperinfestation
Ravi Teja Reddy, Venkatesh Vaithiyam, Sanjeev Sachdeva

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
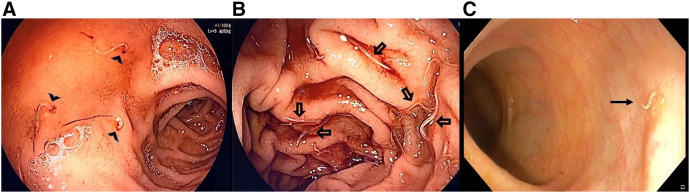 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParasites and Host Interactions · Dermatological diseases and infestations · Helminth infection and control
A 20-year-old male residing in an Indian metropolitan city, with low socio-economic status and no prior comorbidities or addictions, presented with a 2-month history of progressive shortness of breath on exertion, palpitations, and fatigue. Physical examination showed tachycardia, pallor, and pedal edema, but no lymphadenopathy, jaundice, or organomegaly. Laboratory investigations revealed a hemoglobin level of 1.8 g/dL, total leukocyte count of 4.9 × 10^9^/L (differential leukocyte count: 50% neutrophils, 30% lymphocytes, 15% eosinophils, 5% monocytes), absolute eosinophil count of 735/µL, and platelet count of 780,000/µL. The patient’s total protein level was 6.9 g/dL, with albumin of 2.7 g/dL, and the rest of the liver function test and renal parameters were normal. Peripheral smear revealed microcytic hypochromic red cells and pencil cells suggestive of iron-deficiency anemia (IDA). His serum iron level (20 [normal range: 60–170 mcg/dL]) and ferritin level (10 [normal range 20–500 ng/mL]) were low, and his total iron-binding capacity (TIBC) (510 [normal range: 240–450 mcg/dL]) was increased, confirming IDA. Stool examination revealed ova of hookworms. Because of severe anemia and hypoalbuminemia, the patient underwent upper and lower gastrointestinal endoscopy to rule out other organic causes and was found to have multiple hookworms in the duodenum and terminal ileum (Figure 1). The patient was treated with intravenous iron, blood transfusions, and a 400 mg single dose of oral albendazole. At 6 weeks follow-up, the patient had significant clinical improvement, and his hemoglobin level increased to 8.5 g/dL
IDA is the most common form of anemia worldwide, especially in low-resource settings. The most common etiologies include chronic gastrointestinal blood loss, poor dietary intake, and parasitic infestations.1 The parasitic infections most associated with IDA are hookworm (Necator americanus and Ancylostoma duodenale), whipworm (Trichuris trichiura), malaria, and schistosomiasis. Hookworm infestation can cause chronic intestinal blood loss, intestinal inflammation, protein malabsorption, intestinal villous atrophy, and anorexia, leading to iron-deficiency anemia and hypoalbuminemia, as seen in our patient.1 Chronic exposure and reinfection in endemic areas can result in profound anemia requiring transfusions. Direct endoscopic visualization of hookworms is considered a useful diagnostic tool for unexplained anemia with suspected parasitic infections.2^,^3 Treatment involves stabilization with blood transfusion, iron therapy, and antihelminth drugs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hotez PJ, , 2004. Hookworm infection. N Engl J Med 351: 799–807.15317893 10.1056/NEJ Mra 032492 · doi ↗ · pubmed ↗
- 2Chen YY Soon MS, 2005. Endoscopic diagnosis of hookworm infection that caused intestinal bleeding. Gastrointest Endosc 62: 142.15990838 10.1016/s 0016-5107(05)00515-8 · doi ↗ · pubmed ↗
- 3Rana SS Bhasin DK Sinha SK, 2008. Endoscopic diagnosis of chronic severe upper GI bleeding due to helminthic infection. Gastrointest Endosc 68: 1023.10.1016/j.gie.2008.03.106118984109 · doi ↗ · pubmed ↗