Prevalence and Risk Factors of Hypotension in Patients Undergoing Caesarean Section with Spinal Anaesthesia at Muhimbili National Hospital
Willbroad Kyejo, Sunil Samji, Allyzain Ismal, Edwin Lugazia

TL;DR
This study found that nearly 57% of patients undergoing caesarean section with spinal anesthesia experienced hypotension, with risk factors including inadequate fluid preload and higher sensory block levels.
Contribution
The study identifies specific risk factors for hypotension during spinal anesthesia in caesarean sections at a Tanzanian hospital.
Findings
Hypotension occurred in 56.7% of patients undergoing spinal anesthesia for caesarean section.
Risk factors included preload <10 mL/kg, higher sensory block levels, and absence of wedge positioning.
Abstract
Spinal anaesthesia is a common regional technique for caesarean sections, but is associated with hypotension in up to 80% of patients. Preventive measures include; intravenous fluid preloading, left uterine displacement, compression stockings, and vasopressors. This study aimed to determine the prevalence and risk factors of hypotension during spinal anaesthesia in pregnant patients undergoing caesarean section at Muhimbili National hospital. A descriptive cross-sectional study was conducted at Muhimbili National Hospital's Obstetric theatre, involving patients who received spinal anaesthesia during caesarean section from August 2021 to January 2022. The study excluded patients with sedation, anti-hypertensive, pregnancy-induced hypertension, modified Bromage score, or combination anaesthesia. Data was collected, and analysed using SPSS version 20. A total of 300 patients were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
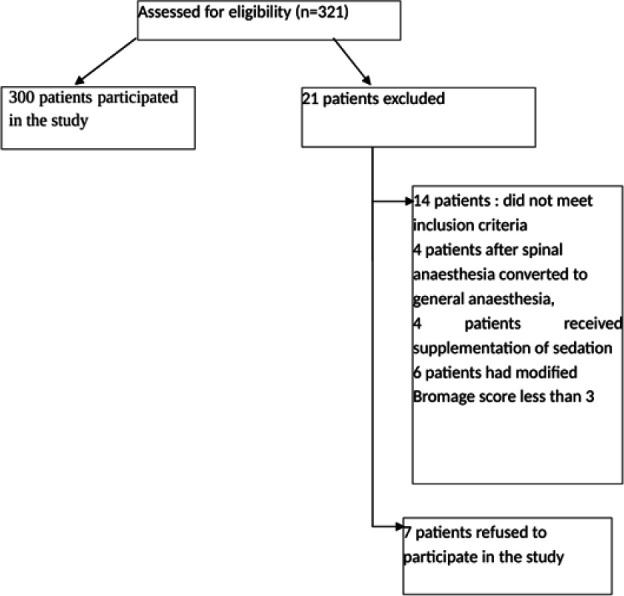 FIGURE 1
FIGURE 1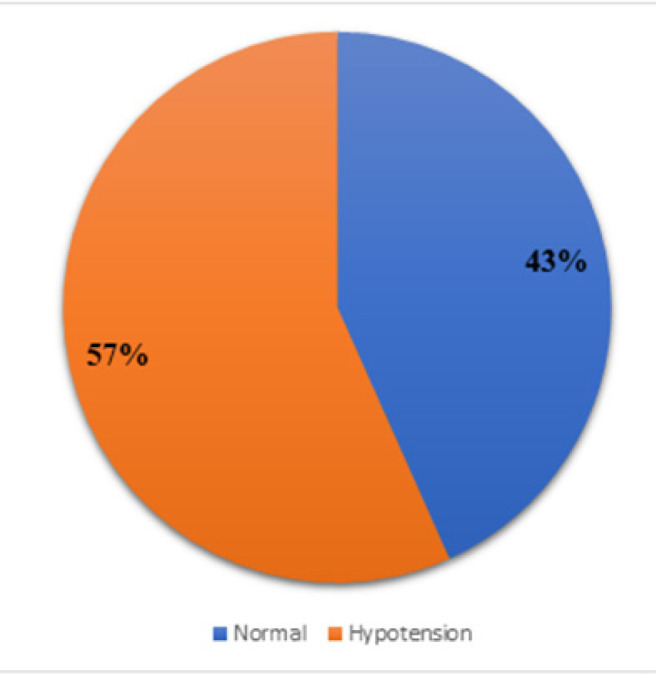 FIGURE 2
FIGURE 2| Variable | Frequency (N) | Percent (%) |
|---|---|---|
| Heights (cm) | ||
| ≤150 | 53 | 17.7 |
| >150 | 247 | 82.3 |
| Gravidity | ||
| Primigravida | 98 | 32.7 |
| 2–4 | 182 | 60.7 |
| >4 | 20 | 6.7 |
| Nature of Caesarean Section | ||
| Elective | 100 | 33.3 |
| Emergency | 200 | 66.7 |
| Local Anaesthetics | ||
| 0.5% hyperbaric Bupivacaine | ||
| 7.5 mg | 60 | 20.0 |
| 10.0 mg | 207 | 69.0 |
| 12.5 mg | 9 | 3.0 |
| 5% heavy Lidocaine | ||
| 75 mg | 24 | 8.0 |
| Total | 300 | 100 |
| Variable | Hypotension. No (%) | Hypotension. Yes (%) | TOTAL (N) (%) | p-value |
|---|---|---|---|---|
| Apgar score | ||||
| Yes ≥ 7 | 129 (99.2) | 164 (96.5) | 293 (97.7) | 0.117 |
| No < 7 | 1 (0.8) | 6 (3.5) | 7 (2.3) | |
| Factor | Hypotension. No (%) | Hypotension. Yes (%) | TOTAL N (%) | p-value |
|---|---|---|---|---|
| Preload (ml/Kg) | ||||
| Less than 10 | 17 (29.8) | 40 (70.2) | 57 (19.0) | .009 |
| 10 to 14 | 54 (42.2) | 74 (57.8) | 128 (42.7) | |
| 15 to 19 | 29 (43.3) | 38 (56.7) | 67 (22.3) | |
| 20 and above | 30 (62.5) | 18 (37.5) | 48 (16.0) | |
| Level of block | ||||
| T4 | 9 (21.4) | 33 (78.6) | 42 (14) | .003 |
| T5 | 63 (41.7) | 88 (58.3) | 151 (50.3) | |
| T6 | 31 (52.5) | 28 (47.5) | 59 (19.7) | |
| T7 | 27 (56.2) | 21 (43.8) | 48 (16) | |
| Presence of wedge | ||||
| Forgotten | 6 (24) | 19 (76) | 25 (8.3) | .042 |
| Wedge 15° left lateral | 124 (45.1) | 151 (54.9) | 275 (91.7) | |
| Nature of surgery | ||||
| Elective | 51 (51) | 49 (49) | 100 (33.3) | .058 |
| Emergency | 79 (39.5) | 121 (60.5) | 200 (66.7) | |
| Gravidity | ||||
| Prime gravida | 47 (36.2) | 51 (30.0) | 98 (32.7) | .495 |
| 1 to 4 | 74 (56.9) | 108 (63.5) | 182 (60.7) | |
| More than 4 | 9 (6.9) | 11 (6.5) | 20 (6.7) | |
| Age | ||||
| 16 to 19 | 10 (7.7) | 8 (4.7) | 18 (6) | .288 |
| 20 to 24 | 15 (11.5) | 30 (17.6) | 45 (15) | |
| 25 to 29 | 46 (35.4) | 54 (31.8) | 100 (33.3) | |
| 30 to 34 | 38 (29.2) | 41 (24.1) | 79 (26.3) | |
| 35 to 39 | 20 (15.4) | 32 (18.8) | 52 (17.3) | |
| More than 39 | 1 (8) | 5 (2.9) | 6 (2) | |
| ASA | ||||
| I | 62 (47.7) | 62 (36.5) | 124 (41.3) | .348 |
| II | 68 (52.3) | 108 (63.5) | 176 (58.7) | |
| Local Aesthetics | ||||
| 5% heavy Lidocaine | 11 (46) | 13 (54) | 24 (8) | .623 |
| 0.5% hyperbaric Bupivacaine. | 119 (43). | 57 (57). | 276 (91.7) | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHemodynamic Monitoring and Therapy · Anesthesia and Pain Management · Intraoperative Neuromonitoring and Anesthetic Effects
BACKGROUND
Spinal anaesthesia, also known as subarachnoid anaesthesia, is a regional anaesthesia technique used to provide numbness and pain relief for surgical procedures.^1,2^ It involves the injection of a local anaesthetic medication into the subarachnoid space, which is the space surrounding the spinal cord and filled with cerebrospinal fluid.^1,2^
The local anaesthetic medication used in spinal anaesthesia blocks the transmission of nerve impulses, resulting in loss of sensation and muscle relaxation in the lower part of the body.^2^ Spread of the anaesthetic agent depends on baricity of solution, patient position, dosage, site of injection, physiological status and height, and once injected, will spread due to gravity and currents of cerebral spinal fluid flow.^3^ As the block progresses, autonomic fibers are blocked first, followed by sensory loss to touch/pinprick, then loss of proprioception, and finally motor function loss. This sequence allows for pain-free surgery or other procedures below the level of the injection.
The extent and duration of both sensory and motor blockade can be controlled by adjusting the type and dose of anaesthetic medication administered.^2^
Spinal anaesthesia is a widely used technique for caesarean section delivery due to its fast and effective sensory and motor block.^4^. It offers significant advantages in this setting, providing effective pain relief and ensuring a smooth surgical experience for the mother. One of the key advantages of spinal anaesthesia is its quick onset of action, providing rapid pain relief within minutes of administration. This allows for prompt initiation of the surgical procedure, minimising any delays or discomfort for the mother. However, one of the most common complications associated with spinal anaesthesia is hypotension, which can have adverse effects on both the mother and the foetus.^5–7^
Hypotension occurs due to the non-specific conduction block produced by local anaesthetics, which affects not only the sensory fibers, but also the pre-ganglionic sympathetic fibers resulting into a sympathetic blockade.^8^ This blockade will induce relaxation of blood vessels resulting in venous dilation, and pooling of blood in the venous system. Consequently, venous return to the right side of the heart decreases, ultimately causing a fall in mean arterial blood pressure.^2,9^ In pregnant women, increased sensitivity to local anaesthetics, combined with aorto-caval compression from the gravid uterus that reduces venous return to the heart, further predisposes them to hypotension^10^ Maternal hypotension during caesarean section can adversely affect both mother and foetus, leading to reduced utero-placental perfusion, foetal bradycardia, and acid-base abnormalities, which may compromise neonatal outcomes.^6^
Despite preventive measures such as crystalloid preloading and left uterine displacement, the incidence of hypotension during spinal anaesthesia remains high, highlighting the need for further investigation and optimisation of management strategies.^6,11,12^ Some adjuvants such as midazolam and α−2 agonists have been studied, as they prolong the sensory blockade, and thereby reduce the required dosage of anaesthesia, which may reduce the incidence of hypotension.^13,14^ Globally, hypotension occurs in 50 to 80% of caesarean sections with spinal anaesthesia, with variability largely attributed to differences in study definitions and populations.^15^
Understanding the proportion of pregnant patients who develop hypotension and identifying associated risk factors is crucial for improving maternal care and outcomes. Such knowledge can guide the development of evidence-based guidelines and protocols for the prevention and management of hypotension during spinal anaesthesia in Tanzania. Maternal hypotension reduces uteroplacental blood flow, directly affecting the foetus and leading to acidosis, metabolic derangements and low APGAR scores at delivery.^16–18^ Implementing standardised guidelines will harmonise practices across healthcare facilities and ensure safe administration of anaesthesia for obstetric patients undergoing caesarean section. In Tanzania, there is limited data regarding the proportion of pregnant patients who develop hypotension during spinal anaesthesia and the associated risk factors. This study aims to provide region-specific estimates and close this gap.
METHODS
Study Design
This hospital-based descriptive cross-sectional study was conducted to determine the prevalence of hypotension and identify associated risk factors among pregnant patients undergoing caesarean section under spinal anaesthesia.
Study Duration
The study was conducted over a 6 months period, from August 2021 to January 2022. This timeframe allowed for the enrolment of adequate number of participants and the collection of sufficient data to achieve the study objectives.
Study Area
The study was carried out in the Obstetric Theatre of Muhimbili National Hospital, the largest referral hospital in Tanzania. Located in Tanzania, the hospital receives referrals from municipal hospitals and other regions of the country. It provided an appropriate setting for the study due to its high volume of obstetric cases and availability of experienced anaesthetists.
Study Population
The study population consisted of all patients who underwent elective and emergency caesarean sections under spinal anaesthesia at Muhimbili National Hospital. Consecutive sampling was employed, enrolling all patients who met the inclusion criteria and gave consent over the 6-month study period.
Inclusion Criteria
Obstetric patients classified as ASA II, scheduled for elective or emergency caesarean sections and consenting to receive spinal anaesthesia were included. This ensured that participants had appropriate health status for spinal anaesthesia and were willing to participate in the study.
Exclusion Criteria
Patients who received sedation or a combination of anaesthesia modalities, including cases where spinal anaesthesia was converted to general anaesthesia, were excluded. Those on anti-hypertensive treatment or with pregnancy-induced hypertension were also excluded. Additionally, patients with a modified Bromage score of 0, 1, or 2 (indicating incomplete motor block) were not included in the study.
Sample Size Estimation
The sample size was determined using the formula for estimating proportions. The following parameters were used:
Critical value (Z) for a 5% significance level: 1.96 Estimated prevalence (P) of hypotension in patients undergoing caesarean section under spinal anaesthesia: 80%^12^
Margin of error (E): 5%
Using the formula N = Z^2^ × P × (100 - P)/E^2^, the estimated sample size (N) was calculated as follows:
To account for potential missing data, 10% was added to the calculated sample size, yielding a target of 270 patients. Ultimately, 300 patients were enrolled, providing a larger sample size and accounting for potential dropouts and incomplete data.
Data collection and study procedure
All eligible patients who provided informed consent were included in the study. For elective cases, demographic data was recorded during the pre-visit period, while for emergency cases, data was collected during the pre-anaesthesia evaluation. Pre-operative fasting time was documented prior to surgery. Crystalloid preload was calculated based on patient weight (10–15 mL/kg) prior to spinal anaesthesia; following standardised protocols, even in emergency settings. Baseline blood pressure and heart rate were recorded after patients were connected to an ECG monitor and automated blood pressure machine.
Using aseptic technique, local anaesthesia (2.0% Lidocaine) was administered through skin infiltration, after which spinal anaesthesia was performed in the seated position at the L2–L3 or L3–L4 inter-space using a 25G spinal needle. The intrathecal agent was either 0.5% hyperbaric Bupivacaine or 5% heavy Lidocaine, depending on availability. Following administration, patients were gently assisted into a supine position with left uterine displacement using a wedge to prevent compression of the aorta and vena cava. Examination to confirm adequate block was confirmed and documented before proceeding with caesarean section. Additionally, mothers received 3–5 L/min of supplemental oxygen through a facemask.
The study period commenced at the time of spinal injection and continued for 30 minutes. The upper sensory level of anaesthesia was assessed by evaluating loss of pinprick discrimination, while block height was determined by loss of sensation to cold methylated spirits. Motor block was assessed using the Modified Bromage scale.
Data collection was conducted prospectively using questionnaires completed by the responsible anaesthetist at the end of each operation. Variables such as; age, gravidity, height, preload administration, hypotension and APGAR score were initially recorded as numerical data and later sub grouped into categorical data. Nature of surgery, level of block, type of infusion, size of intravenous cannula, type of anaesthetic agent used and presence of wedge was recorded as categorical data. Hemodynamic variables (Systolic blood pressure, diastolic blood pressure, mean arterial pressure and heart rate) were recorded every 3 minutes using the automated blood pressure monitor, which also stored additional patient records throughout the procedure, including oxygen saturation. Hypotension was defined as either a mean arterial pressure of less than 65 mmHg or a 20% reduction from the baseline mean arterial blood pressure (whichever occurs first).^19^
Quality Control
Before the study commenced, research assistants received training to ensure proficiency in filling out the study questionnaire. Questionnaires were collected twice daily from the obstetric theatre: once in the evening to capture data from the entire day's cases, and again the following morning to include emergency patients recruited overnight. The principal investigator closely supervised the study to ensure accurate documentation and proper record keeping. This meticulous approach aimed to maintain the integrity and quality of the data collected throughout the targeted study period. Data collectors were not blinded, and this is acknowledged as a limitation.
Data Analysis
Categorical variables were summarised as frequencies and proportions. This information was then tabulated and presented in form of pie charts and tables. The Chi-square test was used to asses statistical significance. All statistical analyses were performed using SPSS version 27.0, with a 5% significance level applied.
Ethical Approval and Consent to Participate
Ethical approval was obtained from the Ethics Committee of Muhimbili University of Health and Allied Sciences. The committee ensured that participants’’ rights, safety, and welfare were protected in accordance with established ethical principles. Written informed consent was obtained from all participants before enrolment. For emergency cases requiring immediate intervention, verbal consent was obtained and documented in line with ethical standards.
RESULTS
A total of 300 pregnant patients comprised the study group (Figure 1), and their demographic data is presented in Table 1. Among the 300 pregnant patients, 33.3% underwent elective caesarean section, while 66.7% underwent emergency caesarean section. The average age of the study population was 29.07 ± 5.5 years, with an average weight of 75.25 ± 13.7 kilograms and an average height of 158.71 ± 9.2 centimetres.
Patient Distribution Flow Chart
In the study, 32.7% of the patients were primigravida, while 67.4% were multiparous. Most of the patients (92%) received 0.5% hyperbaric Bupivacaine as the local anaesthetic while 8% received 5% heavy Lidocaine, of which none developed symptoms of transient neurological syndrome. The dosage of 0.5% hyperbaric Bupivacaine varied, with 20% receiving 7.5 mg, 69.0% receiving 10 mg, and 3% receiving 12.5 mg.
The proportion of pregnant patients who developed hypotension (Figure 2) during caesarean section under spinal anaesthesia was 56.7% (95% CI: 0.511–0.623). However, no association was observed between maternal hypotension and neonatal outcome as assessed by APGAR scores (Table 2).
Pie Chart Showing Proportion of Pregnant Patients Who Developed Hypotension
Factors associated with hypotension are presented in Table 3. A higher proportion of patients (70.2%) with a preload volume below 10 ml/kg developed hypotension. The incidence of hypotension increased with higher sensory block levels (T4–T6). Despite wedge use in 91.7% of pregnant patients, 54.9% still developed hypotension. Hypotension occurred more frequently during emergency caesarean sections e(60.5%) than elective caesarean sections (49%). No significant associations were found with age, gravidity, or choice of local anaesthetic.
DISCUSSION
This study highlights the prevalence and associated factors of hypotension in pregnant patients undergoing caesarean section under spinal anaesthesia. The incidence of hypotension was 56.7%, which aligns with findings from studies conducted outside the African subcontinent.^16,19^ Studies in East Africa showed a prevalence range from 30% to 60%.^20–22^ Hypotension remains a well-known complication of spinal anaesthesia, and its occurrence can have significant implications for both the mother and the foetus.^4^
One of the factors that contribute to hypotension during spinal anaesthesia is the sympathetic block induced by local anaesthetics. This block affects not only the sensory fibers but also the pre-ganglionic fibers to the sympathetic chain, resulting in arterial and venous dilatation. The decrease in venous return to the right side of the heart leads to a fall in mean arterial blood pressure. Additionally, the pressure of the gravid uterus on the aorta and inferior vena cava exacerbates the decrease in venous return, further contributing to maternal hypotension.^2,7^ In this study, patients with a preload volume below 10 ml/kg and those with higher sensory block levels were more likely to develop hypotension, underscoring the importance of optimising preload and monitoring block height as preventive strategies.
The prevalence observed in this study was slightly lower compared to some studies conducted in India and Kenya.^9,21^ These differences could be attributed to variations in patient populations, anaesthetic techniques, and clinical management protocols. It is worth noting that the use of different local anaesthetics, such as 5% heavy Lidocaine and 0.5% hyperbaric Bupivacaine, can also influence the incidence of hypotension. In this study, hypotension occurred more frequently in patients receiving Bupivacaine compared to Lidocaine.
Preventive measures, including crystalloid preloading and left uterine displacement with a wedge, were implemented in this study. Although left uterine tilt has been shown to provide modest hemodynamic benefits^22^, more than half of the patients still developed hypotension. This highlights the persistent challenge of preventing maternal hypotension during spinal anaesthesia. Alternative approaches and interventions such as prophylactic vasopressors and perioperative echo graphic assessment may help to reduce the prevalence of hypotension and its associated complications.^21,23^
The level of sensory block was also a significant factor. Patients with a block height at or above T5 experienced more frequent hypotension than those with lower block levels, consistent with previous studies.^1,4^ This reinforces the need for vigilant monitoring of block level to identify high-risk patients and implement timely interventions.
CONCLUSION
Hypotension remains a common complication of spinal anaesthesia in pregnant patients undergoing caesarean section. This study contributes to existing evidence by identifying preload volume and block height as significant factors associated with its development. Preventive measures such as adequate fluid preload and left uterine tilt, together with careful selection of anaesthetic agents and monitoring of block level, are essential to reduce the incidence and severity of hypotension and improve maternal and foetal outcomes. Future research should focus on optimising anaesthetic protocols and evaluating additional strategies, including prophylactic vasopressors, to enhance the safety and effectiveness of spinal anaesthesia in obstetric patients.
Limitation
This study has several limitations. First, it was conducted exclusively among healthy ASA II pregnant patients, therefore, the findings may not be generalizable to higher-risk populations. Future research should include women with higher ASA classifications and a broader range of patient profiles to better assess responses to spinal anaesthesia.
Second, some emergency patients may have received aggressive fluid therapy prior to arriving in the operating theatre. As preload measurements were taken only after arrival, prior fluid management may not have fully accounted for, potentially affecting the observed incidence of hypotension.
Finally, this study could not determine whether the choice of anaesthetic agent influenced the development of hypotension. Comparative studies assessing different anaesthetic agents are needed to clarify their relative impact on maternal hemodynamic outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bandi E, Weeks S, Carli F. Spinal block levels and cardiovascular changes during post-Cesarean transport. Canadian Journal of Anesthesia. 1999;46:736–40.10451132 10.1007/BF 03013908 · doi ↗ · pubmed ↗
- 2Ferrarezi WPP, Braga Ad Fd A, Ferreira VB, Mendes SQ, Brandão MJN, Braga F Sd S, et al. Spinal anesthesia for elective cesarean section. Bupivacaine associated with different doses of fentanyl: randomized clinical trial. Brazilian Journal of Anesthesiology. 2021;71:642–8.34411627 10.1016/j.bjane.2021.03.030PMC 9373100 · doi ↗ · pubmed ↗
- 3Hocking G, Wildsmith J. Intrathecal drug spread. British journal of anaesthesia. 2004;93(4):568–78.15220175 10.1093/bja/aeh 204 · doi ↗ · pubmed ↗
- 4Terefe T, Tekalegn Y, Irena A. Comparative study of general with Spinal Anesthesia on maternal outcomes for caesarean delivery among preeclamptic women at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia. 2018.
- 5Rocke D, Rout C. Volume preloading, spinal hypotension and caesarean section. British journal of anaesthesia. 1995;75(3):257–9.7547037 10.1093/bja/75.3.257 · doi ↗ · pubmed ↗
- 6Riley ET, Cohen SE, Rubenstein AJ, Flanagan B. Prevention of hypotension after spinal anesthesia for cesarean section: six percent hetastarch versus lactated Ringer's solution. Anesthesia & Analgesia. 1995;81(4):838–42.7574020 10.1097/00000539-199510000-00031 · doi ↗ · pubmed ↗
- 7Lee A, Kee WDN, Gin T. A quantitative, systematic review of randomized controlled trials of ephedrine versus phenylephrine for the management of hypotension during spinal anesthesia for cesarean delivery. Anesthesia & Analgesia. 2002;94(4):920–6.11916798 10.1097/00000539-200204000-00028 · doi ↗ · pubmed ↗
- 8Park CS, Lee H-Y. Clinical utility of sympathetic blockade in cardiovascular disease management. Expert Review of Cardiovascular Therapy. 2017;15(4):277–88.28292194 10.1080/14779072.2017.1307736 · doi ↗ · pubmed ↗