An unhealthy lifestyle and incident activity-limiting neck and back problems in university students: the Sustainable UNiversity Life (SUN) study
Clara Onell, Martin Asker, Helene Wiberg, Pierre Côté, Fred Johansson, Tobias Sundberg, Klara Edlund, Eva Skillgate

TL;DR
University students with unhealthy lifestyles are more likely to develop neck and back pain that limits their daily activities.
Contribution
This study identifies a link between an unhealthy lifestyle and new-onset activity-limiting neck/back problems in university students.
Findings
Students with three or more unhealthy behaviors had a 35% higher risk of developing activity-limiting neck/back problems.
Unhealthy lifestyle behaviors included physical inactivity, high sitting time, and risky substance use.
The study followed participants for one year to assess the development of musculoskeletal issues.
Abstract
Neck and back pain are common musculoskeletal conditions in university students and associated with unhealthy lifestyle behaviors such as physical inactivity, unhealthy dietary habits, smoking and risky alcohol use. Cohort studies have investigated the effect of a healthy lifestyle including several lifestyle behaviors on the risk and prognosis for neck and back pain. Studies of an association between an unhealthy lifestyle and musculoskeletal conditions in university students are lacking. This study aimed to assess the association between an unhealthy lifestyle and incident activity-limiting neck/back problems (ALNBP) in university students. Participants enrolled in the Sustainable UNiversity Life (SUN) study who did not report baseline ALNBP in the past three months were included (n = 3492). The baseline web-survey assessed unhealthy lifestyle behaviors (physical inactivity, high…
Click any figure to enlarge with its caption.
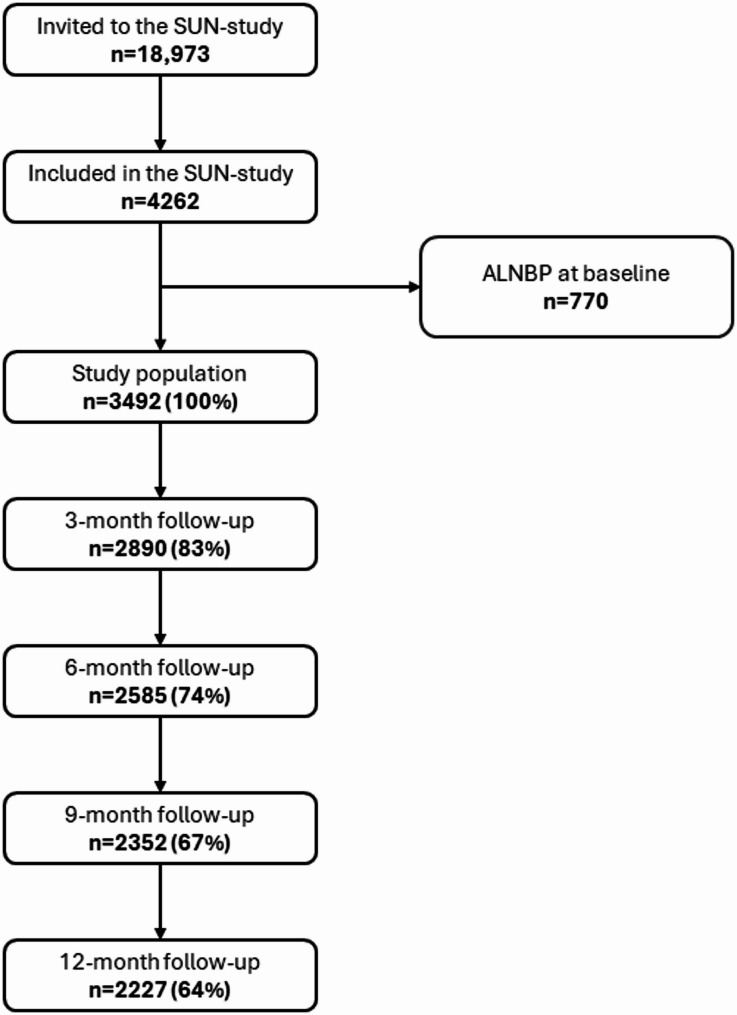 Figure 1
Figure 1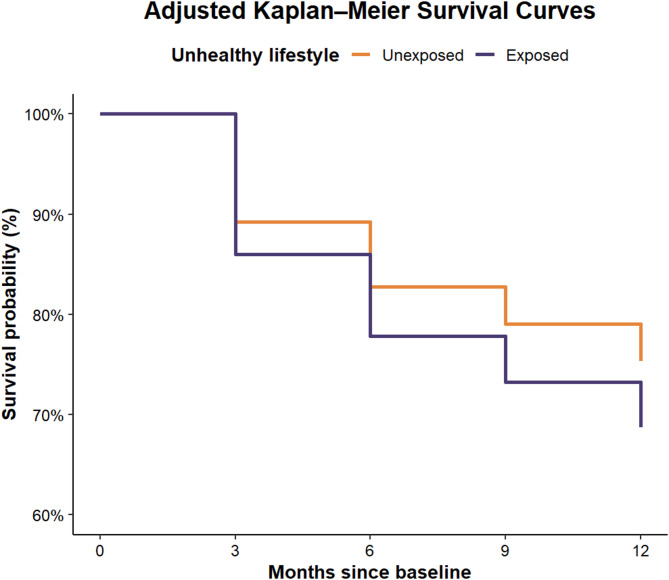 Figure 2
Figure 2- —Sophiahemmet University College
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMusculoskeletal pain and rehabilitation · Workplace Health and Well-being · Occupational Health and Performance
Background
Neck and back pain (NBP) are the most common musculoskeletal conditions and leading contributors to global ill-health, disability and need of rehabilitation worldwide [1–4]. The prevalence of NBP increases with age, yet a large burden is imposed also in younger populations [5], including university students [6, 7]. The prevalence of musculoskeletal pain in university students is suggested to have increased since the beginning of this century [8], and chronic pain has been estimated to affect 54% of university students [6], where NBP is most common [6, 9]. Not all musculoskeletal conditions interfere with daily functioning, but many can become activity-limiting and have a significant impact on overall health [4]. For example, musculoskeletal conditions in university students are associated with impaired academic functioning, poor sleep quality and poor health-related quality of life [10, 11].
In university students, NBP is more common among women [12], older students and students in health care programs [13]. Cross-sectional studies suggest that NBP in university students is associated with sedentary behavior [14], physical inactivity and coffee intake [15], use of digital devices [12, 16–21], anxiety, stress, and sleep disturbances [13, 14, 22, 23]. Cohort studies have identified discrimination and a poor study environment [24], previous NBP, poor back support, muscle tightness [25], sedentary behavior, computer, and mobile use [26] as potential risk factors for NBP in university students.
University students are prone to unhealthy lifestyle behaviors, including sedentary behavior, physical inactivity, and low intake of fruits and vegetables [27–30]. Such behaviors are part of a broader public health concern, as physical inactivity, unhealthy diet, tobacco use, and risky alcohol consumption are recognized contributors to chronic noncommunicable diseases and account for a substantial portion of the disease burden in Sweden [31, 32]. Moreover, individual lifestyle behaviors often cluster [33–36], and clustering of healthy or unhealthy behaviors is common among university students [34, 36], with an unhealthy lifestyle being associated with impaired quality of life [34].
Studies of non-student populations have investigated the importance of lifestyle behaviors for the risk and prognosis of NBP [37–41], where a healthy lifestyle consistently has been shown to be protective against NBP and associated with favorable prognosis among those affected. To the best of our knowledge, no studies have investigated the role of an unhealthy lifestyle for the risk of NBP in university students. Deepening the knowledge about modifiable risk factors for NBP in university students, and especially for activity-limiting conditions, is key for implementation of future preventive strategies. The aim of this study was, therefore, to investigate the association between an unhealthy lifestyle and incident activity-limiting neck/back problems (ALNBP) in university students.
Methods
This study is based on the Sustainable UNiversity Life (SUN) study with the primary aim to identify risk and prognostic factors for mental health problems and musculoskeletal problems in university students (ClinicalTrials.gov ID NCT04465435 registration date 2020-06−17). The SUN-study is described in detail in the published study protocol [42]. Students enrolled at educational programs at eight Swedish universities in Stockholm and Örebro were invited to participate in the SUN-study. Participant recruitment was ongoing between August 2019 and December 2020. Participants were recruited at university campuses in 2019, where study staff gave classroom presentations explaining the study’s purpose and significance. Following the outbreak of the COVID-19 pandemic in 2020, physical recruitment was replaced with digital methods, including online presentations or email invitations. All eligible students received an invitation through email with a link to a baseline web-survey. Included participants received four follow-up surveys with three-month intervals over one year. To ensure accessibility, the surveys were provided both in Swedish and English. Data collection finished in December 2021, when the last group of students responded to the fourth follow-up survey. The SUN-study was conducted according to the Helsinki Declaration, obtained ethical approval by the Swedish Ethical Review Authority (reference number 2019–03276 and 2020 − 01449) and all participants provided informed consent electronically prior to enrollment in the study.
Study population
A total of 18,973 university students were invited to the SUN-study, and 4262 students (22%) agreed to participate. At baseline, 770 participants reported ALNBP the past three months and were therefore excluded from the analyses, resulting in a cohort of 3492 participants. Participants were included until the first follow-up with an event of ALNBP, loss to follow-up or end of the one-year study period, whichever came first. Inclusion and follow-up in this study is presented in Fig. 1.
Fig. 1. Flowchart of participant inclusion and follow-ups. Abbreviations: ALNBP, activity-limiting neck/back problems; SUN-study, Sustainable UNiversity Life study
Baseline measures
Physical activity
Two questions from the National Board of Health and Welfare [32] in Sweden were used to assess physical activity. Weekly minutes of exercise (e.g. running, ball sports) and daily activities (e.g. walking, cycling) during a normal week were reported. Total physical activity was calculated as a sum of minutes per week in exercise and minutes per week in daily activities, with exercise minutes doubled to account for intensity. Physical inactivity was categorized as physical activity < 150 min per week [43].
Sitting time
Sitting time was assessed with the SED-GIH single question [44], which has shown excellent reliability but poor validity, in line with other common questionnaires assessing sitting time. Habitual daily sitting time, excluding sleep, was reported in hours. High sitting time was categorized as sitting ≥ 10 h per day [44].
Meal frequency
Meal frequency was assessed with questions about habitual intake frequency of main meals breakfast, lunch, and dinner, reported as 0–7 days per week. Meal skipping was categorized as skipping at least one of the main meals ≥ 4 days per week [45].
Alcohol, tobacco, and illicit drug use
Alcohol, tobacco and illicit (non-medical) drug use were assessed with the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST), which has shown acceptable validity for identifying varying degrees of use [46, 47]. The ASSIST generates a score of 0–42 categorized as low, moderate, or high-risk of problems or dependence. Risky alcohol, tobacco, and illicit drug use, respectively, were categorized as a moderate or high-risk score for alcohol, tobacco, and illicit drugs.
Exposure: unhealthy lifestyle
The separate unhealthy lifestyle behaviors physical inactivity, high sitting time, meal skipping, and risky use of alcohol, tobacco, and illicit drugs, respectively, were combined into a total of 0–6 unhealthy lifestyle behaviors, with ≥ 3 unhealthy lifestyle behaviors (the highest quantile) categorized as exposure to an unhealthy lifestyle.
Outcome: activity-limiting neck/back problems
The outcome ALNBP was evaluated at each follow-up with a modified version of the Nordic Musculoskeletal Questionnaire (NMQ) as being limited in normal daily activities (e.g. studies, hobbies) in the past three months due to trouble (ache, pain, discomfort) in the neck, low back and/or midback [48]. The questionnaire was modified to allow measurements every third month for one year and asked about the past three months instead of the past twelve months as in the original NMQ. The NMQ has been widely used in the Nordic countries, and reliability tests with test-retest have been conducted with adequate results (0–23% of non-identical answers) as well as validity tests against clinical history (0–20% of non-identical answers) [48].
Statistical analyses
The association between an unhealthy lifestyle and the first event of ALNBP was estimated using crude and adjusted Cox proportional hazard regression models and presented as a hazard rate ratio (HRR) with a 95% confidence interval (CI). Plots of the Schoenfeld and Martingale residuals indicated proportional hazards and no nonlinearity or influential observations. Months since baseline was the underlying timescale. A priori, age (continuous), gender (woman or other), and highest parental education (at least one parent with a university degree, proxy for socioeconomic status) assessed at baseline were included covariates in the analysis. These, and other factors considered but not included in the final analysis, are presented in a directed acyclic graph (DAG) in Supplemental Fig. 1. To visualize the proportion of exposed and unexposed participants with the outcome at each follow-up, Kaplan–Meier survival curves were generated based on the adjusted Cox proportional hazard regression model. The curves were estimated using the conditional method, which estimates survival probabilities for a hypothetical individual with fixed baseline covariate values selected to represent a typical participant profile in the sample. As a sensitivity analysis, an E-value was calculated to estimate the magnitude of a confounder association that could produce bias equal to the observed association, i.e. the strength of association that an unmeasured confounder would need to have with both the exposure and the outcome, conditional on the covariates, to explain away the association [49]. Data management and analyses were performed in R version 4.2.1 (2022-06−23 UCRT).
Results
Descriptive characteristics of the included participants are presented by exposure status in Table 1. Most participants were young women, enrolled in a medicine/health or technology education program, born in Sweden and had at least one parent with a university degree. Also, the vast majority did not report moderate or severe symptom levels of mental health problems (depression, anxiety, and stress).Table 1. Baseline participant characteristics presented by exposure statusExposed to an unhealthy lifestyle^1^ (n = 574)Unexposed to an unhealthy lifestyle (n = 2918)Age, mean years ± SD24.0 ± 5.324.6 ± 6.1Gender, n (%) Woman328 (57)1760 (60) Man241 (42)1143 (39) Other5 (1)15 (< 1)Type of education, n (%) Medicine/health218 (38)1335 (46) Technology283 (49)1221 (42) Social science50 (9)230 (8) Economy20 (3)82 (3) Other3 (1)50 (2)Born outside Sweden, n (%)133 (23)613 (21)Living alone, n (%)179 (32)793 (27)≥One parent with university degree, n (%)411 (72)2142 (73)≥Moderate depression symptoms^2^, n (%)232 (40)659 (23)≥Moderate anxiety symptoms^2^, n (%)136 (24)422 (14)≥Moderate stress symptoms^2^, n (%)157 (27)525 (18)Physical inactivity^3^, n (%)355 (62)431 (15)High sitting time^4^, n (%)435 (76)1006 (34)Meal skipping^5^, n (%)445 (76)713 (24)Risky alcohol use^6^, n (%)213 (37)209 (7)Risky tobacco use^6^, n (%)345 (60)446 (15)Risky illicit drug use^6^, n (%)112 (20)58 (2)^1^Having ≥ 3 unhealthy lifestyle behaviors (i.e. physical inactivity, high sitting time, meal skipping, risky alcohol use, risky tobacco use and risky illicit drug use)^2^Depression, Anxiety and Stress Scale 21 [50]^3^Total physical activity < 150 min per week^4^Daily sitting ≥ 10 h per day^5^Skipping breakfast, lunch and/or dinner ≥ 4 days per week^6^Alcohol, Smoking and Substance Involvement Screening Test [46]
At baseline, a total of 574 participants (16%) were exposed to an unhealthy lifestyle. Of these, 355 (62%) were categorized as physically inactive, 435 (76%) had a high sitting time, 445 (76%) skipped meals, 213 (37%) had a risky alcohol use, 345 (60%) had a risky tobacco use and 112 (20%) had a risky illicit drug use.
There were 583 events among the 2918 participants unexposed to an unhealthy lifestyle (20% of the unexposed participants had ALNBP) and 135 events among the 574 participants exposed to an unhealthy lifestyle (24% of the exposed participants had ALNBP) during the one-year follow-up. Adjusted Kaplan Meier survival curves are illustrated in Fig. 2.
Fig. 2. Adjusted Kaplan–Meier survival curves comparing participants exposed and unexposed to an unhealthy lifestyle at follow-up. Curves were estimated using the conditional method based on the Cox proportional hazard regression model, for the covariate levels median age (23 years), female gender, and having at least one parent with a university degree
Crude HRR for the association between an unhealthy lifestyle and incident ALNBP was 1.32 (95% CI 1.10, 1.59). The adjusted analysis generated a HRR of 1.35 (95% CI 1.12, 1.63).
The sensitivity analysis shows that the adjusted HRR could be explained away by an unmeasured confounder associated with an unhealthy lifestyle and ALNBP by a risk ratio of 1.76 above and beyond the measured confounders, whereas weaker confounding would not do so. Likewise, the CI could be moved to include the null by an unmeasured confounder associated by a risk ratio of 1.38 above and beyond the measured confounder, whereas weaker confounding would not do so.
Discussion
This study found an association between an unhealthy lifestyle, categorized as ≥ 3 unhealthy lifestyle behaviors (physical inactivity, high sitting time, meal skipping, risky alcohol use, risky tobacco use and risky illicit drug use), and incident ALNBP in university students, compared to < 3 unhealthy lifestyle behaviors.
The study addresses disease prevention including the assessment of health risks, in contrast to most previous research on this topic focusing on health-promotion, with the aim to encourage activities that facilitate healthy living and well-being [51]. Therefore, previous studies are not totally comparable with our study. Cohort studies by Bohman et al. (2014 and 2019) and Skillgate et al. (2017) investigated the association between a healthy lifestyle and the risk and prognosis of NBP [37–39], where a healthy lifestyle including recommended physical activity levels and sufficient fruits/vegetables intake, low alcohol consumption and non-smoking were associated with a lower risk and a better prognosis of NBP. To the best of our knowledge, only one previous cohort study has investigated the association between an unhealthy lifestyle and musculoskeletal outcomes [40]. Smedbråten et al. (2022) found that an accumulation of ≥ 4 unhealthy lifestyle behaviors (low physical activity level, sleep problems, insufficient fruit/vegetables consumption, smoking, frequent alcohol intoxication and illicit drug use) was associated with persistent musculoskeletal pain eleven years later in adolescents with musculoskeletal pain at baseline. Apart from focusing on musculoskeletal pain instead of activity-limiting musculoskeletal problems, as well as including some other lifestyle behaviors (i.e., sleep, fruits/vegetables intake and frequency of alcohol, tobacco, and drugs instead of risk use), the study by Smedbråten et al. (2022) also differs from the current study by including a higher cut-off of what is considered an unhealthy lifestyle. Given the advances in public health research of the severe and manifold consequences of having an unhealthy lifestyle [31], a cut-off of ≥ 3 instead of ≥ 4 unhealthy lifestyle behaviors was considered more appropriate. Moreover, we used a slightly different definition of an unhealthy lifestyle that was based on scientific consensus of which unhealthy lifestyle behaviors that are of highest concern for global ill-health [31], with cut-offs based on current public health recommendations [43–47].
This study includes a large sample of university students from a range of education programs, which strengthens the results’ external validity. The longitudinal study design allows investigation of a temporal, potentially causal relationship between an unhealthy lifestyle and incident ALNBP. For that purpose, students with ALNBP at baseline were excluded. Having an unhealthy lifestyle was less common among included participants (16%) compared to participants that were excluded due to having ALNBP at baseline (22%).
It is important to acknowledge that although the outcome was defined as being limited in normal daily activities due to a musculoskeletal problem, it is possible that some participants had a musculoskeletal problem that not yet had been developed to activity-limiting, but that the problem itself could impact lifestyle behaviors. For example, NBP not being so severe that it had become activity-limiting might have influenced alcohol or illicit drug use, which would have led to reverse causality with a potential overestimation of the results.
A set of covariates was included in the analysis. However, residual or unmeasured confounding of the association between an unhealthy lifestyle and ALNBP cannot be ruled out, especially since lifestyle behaviors are complex and likely related to a range of factors. An unhealthy lifestyle could be a proxy for an overall poorer health, compared to a healthy lifestyle. For example, a larger proportion of the participants exposed to an unhealthy lifestyle had moderate or severe symptoms of mental health problems as well as poor sleep quality, which are associated with both unhealthy lifestyle behaviors and NBP. It is, however, possible that mental health problems and poor sleep quality, although measured at baseline, are part of the causal pathway between an unhealthy lifestyle and ALNBP, as suggested in the DAG in Supplemental Fig. 1, in which an unhealthy lifestyle could lead to poor sleep or mental health problems (or vice versa). Including these factors in the statistical model could, potentially and erroneously, adjust away the association, which was the rationale for not including factors other than demographics, preceding both the exposure and outcome, in the final model. The E-value sensitivity analysis indicates that unmeasured or residual confounders would need to increase the risk of an unhealthy lifestyle and ALNBP by 76% to move the HRR point estimate to the null. Residual confounding could, hence, potentially explain away the observed association, but needs to be moderately associated with an unhealthy lifestyle and ALNBP, even after adjustment of potential confounders. Given the complexity of lifestyle behaviors, it is not impossible that other factors (e.g. genetics) could confound the association, hence the result would be explained by confounding.
There is a risk of misclassification of the separate lifestyle behaviors used to categorize the exposure, where the association between an unhealthy lifestyle and incident ALNBP could have been under or overestimated. The reason for the categorization of exposed as ≥ 3 unhealthy lifestyle behaviors was to capture the lifestyle as an overall behavior and not to assess single lifestyle behaviors, and not to have too few exposed participants in the statistical analysis. Since self-reported lifestyle behaviors tend to be reported in accordance with social desirability, objective methods (e.g. physical activity assessed with an accelerometer) would likely have given more accurate measures. There is, furthermore, a risk of loss of in-depth information by dichotomization of the variables included in the unhealthy lifestyle exposure, such as physical activity where a potential U-shaped association with musculoskeletal problems [52] was not considered. The instruments used to measure physical activity and risky use of alcohol, tobacco and illicit drug use have shown acceptable, yet not excellent, validity and reliability. Also, it is possible that a healthy lifestyle was not captured with the separate lifestyle behaviors included. For example, it would have been more informative to measure adherence to the Nordic Nutrition Recommendations (i.e. intake frequency of fruits/vegetables, whole-grain, candy, sugar-sweetened beverages etc.) than meal frequency for capturing unhealthy dietary habits. Also, it is possible that participants changed their lifestyle behaviors during the one-year follow-up, which could lead to a dilution of the found associations. Finally, the chosen cut-off for an unhealthy lifestyle might not be optimal, since having also < 3 unhealthy lifestyle behaviors could be considered an unhealthy lifestyle from a medical perspective (e.g. a risky alcohol use and smoking one package of cigarettes per day) even if having also other healthy lifestyle behaviors. From this perspective, the associations might be underestimated. Any misclassification of the exposure would, however, likely be non-differential and dilute a true association.
This study had an acceptable three-month follow-up rate of on average 72%, yet potential selection bias might threaten the study’s validity, given that it is unknown whether the non-responders would have different rate of incident ALNBP. Among those lost to follow-up at the last time-point of measurements, 20% were exposed to an unhealthy lifestyle at baseline compared to 14% among those successfully followed. The exposure status is similar but may have introduced selection bias if the loss to follow-up are related to the outcome, i.e. if the non-responders also had a higher rate of incident ALNBP, the results may be somewhat biased.
Given that unhealthy lifestyle behaviors tend to cluster [33–36], our aim was to investigate an unhealthy lifestyle as an overall behavioral pattern. The mechanisms behind the association of an unhealthy lifestyle and ALNBP are likely multi-factorial, where biological, social, and psychological mechanisms interact, and should suggestively be further investigated. The findings of this study add to the existing knowledge about the role of lifestyle behaviors for common musculoskeletal problems with high societal relevance, and advocate for future studies investigating the role of lifestyle in prevention of ALNBP in university students. In the ongoing work to better understand the complex etiology of ALNBP, the findings from this study may offer valuable insights that support the future health of university students. Given the well-established benefits of a healthy lifestyle across various health domains, continued efforts to promote healthy living remain essential.
Conclusion
An unhealthy lifestyle, categorized as ≥ 3 unhealthy lifestyle behaviors, is associated with incident activity-limiting neck/back problems in university students.
Supplementary Information
Supplementary Material 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global, regional, and national burden of low back pain, 1990-2020, its attributable risk factors, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023;5(6):e 316-e 29.10.1016/S 2665-9913(23)00098-XPMC 1023459237273833 · doi ↗ · pubmed ↗
- 2World Health Organization. Noncommunicable diseases. Geneva: World Health Organization. 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases. Cited 2024 May 10.
- 3Socialstyrelsen. Nationella riktlinjer för prevention och behandling vid ohälsosamma levnadsvanor: Stöd för styrning och ledning. Stockholm: Socialstyrelsen. 2018. Available from: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/nationella-riktlinjer/2018-6-24.pdf. Cited 2024 May 10.