Prenatal diagnosis of fetuses with ultrasound soft markers
Qianzhu Jiang, Chang Tan, Lin Yuan, Aziz Ur Rehman Aziz, Haihua Yu, Xiliang Wang

TL;DR
This study examines how ultrasound soft markers relate to fetal chromosomal issues and compares two genetic tests for prenatal diagnosis.
Contribution
The study compares karyotype and CMA testing for prenatal diagnosis of ultrasound soft markers and highlights their diagnostic differences.
Findings
11.41% of cases had chromosomal abnormalities, with multiple soft markers strongly linked to aneuploidy.
CMA detected 65 abnormalities while karyotype found 63, with 18 discordant results.
Live births with abnormalities showed no abnormal phenotypes at 3–5 years.
Abstract
This study aims to evaluate the association between ultrasound soft markers and fetal chromosomal abnormalities and to compare the diagnostic efficacy of karyotype analysis versus chromosomal microarray analysis (CMA) for prenatal testing strategy optimization. A retrospective review was conducted on 622 cases receiving prenatal diagnosis for abnormal ultrasound soft markers at our center over three years. All cases underwent chromosomal karyotype analysis and CMA testing. The differences between the results of these two tests, as well as the correlation between genetic testing results and abnormal ultrasound soft markers, were analyzed. Additionally, the pregnancy outcomes and postnatal phenotypes of all cases were monitored. The overall prevalence of chromosomal abnormalities was 11.41% (71/622). Echogenic intracardiac focus (P = 0.012) and multiple soft markers (P < 0.001)…
Click any figure to enlarge with its caption.
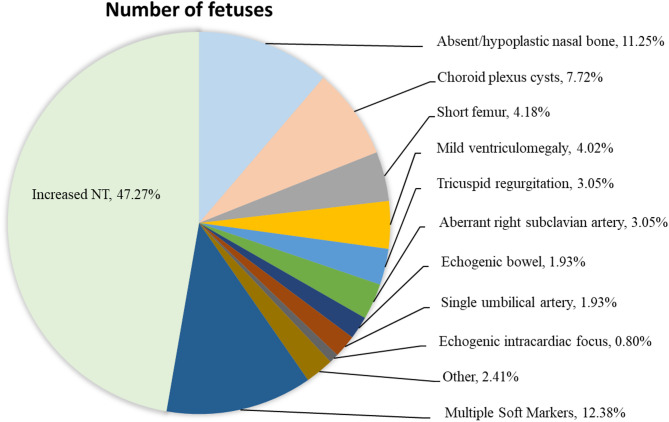 Figure 1
Figure 1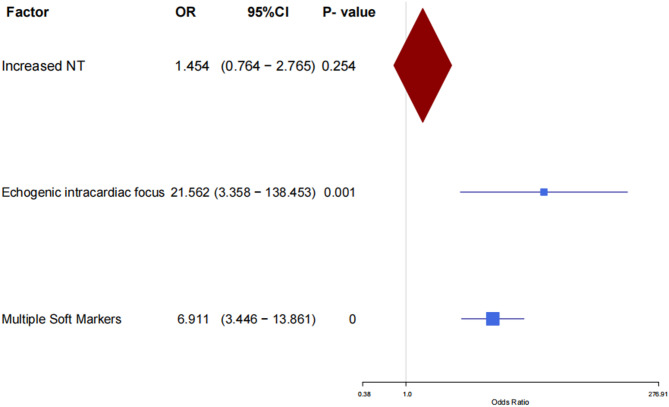 Figure 2
Figure 2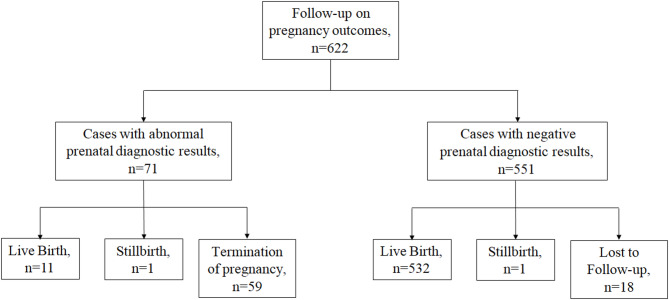 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPrenatal Screening and Diagnostics · Fetal and Pediatric Neurological Disorders · Genomic variations and chromosomal abnormalities
Introduction
The soft markers of the fetus are nonspecific, slight, and often temporary variations in fetal structure, including increased nuchal translucency (NT), absent nasal bone, choroid plexus cyst, short femur, mild ventriculomegaly, tricuspid regurgitation, aberrant right subclavian artery, echogenic bowel [1]. The incidence of isolated soft markers in normal fetuses is about 10% [2]. These markers often appear during a particular stage of fetal growth and development, and commonly resolve in the third trimester of pregnancy, but they may be associated with chromosomal abnormalities [3, 4].
Amniocentesis stands as the principal modality for prenatal genetic diagnosis, with a decades-long trajectory of clinical implementation. Although existing studies have demonstrated that this invasive procedure does not significantly increase the risk of pregnancy loss before 24 weeks of gestation, its clinical adoption remains constrained by procedural invasiveness [5]. Previous studies have investigated the prenatal diagnosis of cases with abnormal ultrasound soft markers, the clinical decision regarding whether pregnant women presenting ultrasound soft markers should undergo invasive diagnostic genetic testing remains complex [6–8].
Multiple modalities are currently available for chromosomal abnormality detection. As the gold standard for prenatal diagnosis, karyotype analysis enables reliable detection of aneuploidies. Meanwhile, chromosomal microarray analysis (CMA) based on comparative genomic hybridization (CGH) arrays and single-nucleotide polymorphism (SNP) arrays demonstrate superior performance in detecting copy number variations (CNVs) and uniparental disomy (UPD) [6, 9]. However, the optimal diagnostic strategy for pregnant women presenting with abnormal ultrasound soft markers remains to be determined.
To provide further reference information, we have reviewed prenatal diagnosis cases from January 2019 to December 2021, focusing specifically on those with ultrasound soft markers for comprehensive analysis. Our primary objective is to investigate associations between ultrasound soft markers and fetal chromosomal abnormalities, and to compare the diagnostic performance of karyotype analysis versus CMA. The findings of this study will offer invaluable references for prenatal genetic counseling, guiding decisions on the necessity of prenatal diagnosis and the selection of appropriate methods in relevant cases.
Methods
Participants
The study retrospectively analyzed cases at the Dalian Women and Children’s Medical Center (Group) from January 2019 to December 2021, specifically focusing on pregnant women who underwent amniocentesis for genetic testing after fetal ultrasound examinations revealed the presence of soft markers. Notably, pregnant women with confirmed fetal structural abnormalities were excluded from this study.
Ultrasound examination
In our center, the ultrasound soft markers were identified during the first-trimester (11 ~ 13 weeks + 6 days) and second-trimester (20 ~ 24 weeks) scans (GE Voluson E8; GE Voluson E10). All ultrasound examinations were performed in strict accordance with the standardized protocols established by the International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) and the Ultrasound Branch of the Chinese Medical Association [10, 11]. The ultrasound soft markers analyzed included: increased NT (11w ~ 13w + 6, ≥ 3.0 mm), absent nasal bone (including unilateral and bilateral absence), choroid plexus cyst (> 2 mm), short femur length (≤ 10 percentile), mild ventriculomegaly (≥ 10 mm and < 13 mm), tricuspid regurgitation, aberrant right subclavian artery, echogenic bowel (echo intensity equal to or exceeding that of adjacent bone), single umbilical artery, echogenic intracardiac focus, reversed A-wave in the ductus venosus, umbilical cord cyst, persistent right umbilical vein and pyelic separation (≥ 4 mm). The ultrasound soft markers evaluated in the first trimester include increased NT, absent nasal bone, reversed A-wave in the ductus venosus, and single umbilical artery. The remaining markers were assessed during the second trimester.
Genetic counseling
For cases with ultrasound soft marker anomalies detected in the first trimester, non-invasive prenatal testing (NIPT) or amniocentesis were recommended [12]. For soft marker anomalies identified in the second trimester, amniocentesis was primarily recommended. Amniocentesis was optimally performed between 18 and 24 weeks of gestation. Procedures outside this window required rigorous risk-benefit evaluation and multidisciplinary review, with emphasis on maternal-fetal safety and procedural feasibility. All participants must be duly informed about the potential for false-positive and false-negative outcomes in NIPT [13]. Additionally, participants were informed that amniocentesis carries potential complications including fetal loss, premature rupture of membranes, chorioamnionitis, fetal injury, and severe maternal complications, though the incidence rates of these adverse events are extremely low [5, 14]. For pregnant women with contraindications to invasive prenatal diagnosis, including threatened abortion, bleeding diathesis, active chronic pathogen infection, or Rh-negative blood type, amniocentesis is contraindicated. Instead, NIPT is suggested as an alternative [14]. All participants voluntarily chose whether to undergo amniocentesis after providing informed consent.
Chromosome karyotype analysis
The procedure involves collecting 20mL of the amniotic fluid from each patient under the ultrasound guidance (GE Voluson E10). For each sample, a minimum of 20 karyotypes were selected for counting, and an additional 5 karyotypes were selected for further detailed analysis, in accordance with the guidelines outlined in the International System for Human Cytogenomic Nomenclature (ISCN 2016).
The abnormalities diagnosed using chromosome karyotype analysis included aneuploidy, deletions, duplications, mosaicism, balanced and unbalanced translocations, inversions, small supernumerary marker chromosomes. However, chromosomal polymorphism was excluded from the diagnosis (relevant cases presented in Supplement Table 3).
CMA
For each case, 10mL of amniotic fluid was selected. The procedure was carried out in accordance with the manufacturer’s guidelines, as detailed in our previously published work [15]. Annotation was performed using the Genome Reference Consortium Human Build 37 (GRCh37), and the database utilized for data analysis has been detailed in our previous research [15]. The interpretation of CNVs was based on the consensus guidelines provided by the American College of Medical Genetics and Clinical Genome Resource (ACMG-ClinGen). CNVs were divided into five categories: pathogenic, likely pathogenic, variants of uncertain significance (VUS), likely benign and benign. The study primarily focuses on the discussion of pathogenic and likely pathogenic CNVs as well as uniparental disomies (UPDs).
Pregnancy outcomes and postnatal follow-up
All cases underwent follow-up on pregnancy outcomes via telephone interviews and medical record reviews. For cases with abnormal prenatal diagnostic results who were born, a secondary follow-up was conducted at 3–5 years of age through telephone and in-person interviews to evaluate postnatal health examination outcomes, including systematic physical examinations, organ-specific functional assessments, metabolic/hematological testing, and neurobehavioral development evaluations.
Statistical processing
Statistical analysis was conducted using statistical software SPSS19.0. The forest plot was generated using R software (version 3.6.0). The count data were statistically described as the number of cases (percentage) [n (%)]. For the statistical analysis, cases of aneuploidy combined CNVs and aneuploidy combined translocation were classified into the aneuploid group. The chi-square (χ²) test or Fisher’s exact test was used to compare the prevalence of abnormal ultrasound markers across different prenatal diagnosis outcomes. Variables with P < 0.1 in univariate analysis were selected for multifactorial binary logistic regression and presented through a forest plot, with P < 0.05 considered statistically significant.
Results
Case profiles
The total number of cases was 622, including 545 cases in the isolated soft marker group and 77 cases in the multiple soft markers group. The average maternal age was 31.6 years, with a range of 19 to 43 years, while the average gestational age for prenatal diagnosis was 20w + 6, ranging from 17w to 28w + 3. Among our cohort, the majority of cases belonged to the increased NT group (294/622, 47.27%), followed by the absent nasal bone group (70/622, 11.25%) and the choroid plexus cyst group (48/622, 7.72%) (shown in Fig. 1; Table 1).
Fig. 1. Phenotypic characteristics of 622 prenatal cases
Table 1. Prevalence rates of chromosomal abnormalities in different soft marker groupsUltrasound categoryUltrasound-determined gestational ageNumber of fetusesChromosomal abnormalities (n (%))AneuploidiesCNVsTranslocationsIncreased NTFirst-trimester29427(9.18)2043Absent nasal boneFirst-trimester709(12.86)810Single umbilical arteryFirst-trimester120(0.00)000Choroid plexus cystSecond-trimester483(6.25)120Short femurSecond-trimester261(3.85)100Mild ventriculomegalySecond-trimester250(0.00)000Tricuspid regurgitationSecond-trimester192(10.53)020Aberrant right subclavian arterySecond-trimester191(5.26)001Echogenic bowelSecond-trimester120(0.00)000Echogenic intracardiac focusSecond-trimester53(60.00)300Other-150(0.00)000Multiple Soft Markers-7725(32.47)2401Total-62271(11.41)5795
Prevalence of chromosomal abnormalities
In our cohort, the overall prevalence of chromosomal abnormalities was 11.41% (71/622). The chi-square (χ²) test or Fisher’s exact test revealed that increased NT, echogenic intracardiac focus, and multiple soft markers might be associated with chromosomal abnormalities (shown in Table 2). Further multifactorial binary logistic regression analysis and the forest plot validated that echogenic intracardiac focus, particularly multiple soft markers, demonstrated a highly significant correlation with chromosomal abnormalities (shown in Table 3; Fig. 2). In the echogenic intracardiac focus group, trisomy 21 was identified in 1 case, while complex chromosomal mosaicism accounted for the remaining 2 cases. In the multiple soft markers group, 19 cases of trisomy 21, 5 cases of trisomy 18, 1 case of balanced translocation were identified, with no CNVs detected (shown in Table 4). Statistical analysis using the χ² test revealed a significant difference in the proportions of aneuploidies between isolated and multiple soft marker groups (χ² = 38.519, P < 0.001). In contrast, no significant difference was observed in the rate of CNVs between these groups.
Table 2. Chi-square test with abnormal ultrasound markers and prenatal diagnosesFindings on ultrasoundPrenatal diagnostic results P Increased NT (n (%))Normal267(48.46)0.098^#^Aberrant27(38.03)Absent nasal bone (n (%))Normal61(11.07)0.687Aberrant9(12.68)Choroid plexus cyst (n (%))Normal45(8.17)0.241Aberrant3(4.23)Short femur (n (%))Normal25(4.54)0.344Aberrant1(1.41)Mild ventriculomegaly (n (%))Normal25(4.54)0.1Aberrant0(0)Tricuspid regurgitation (n (%))Normal17(3.09)1Aberrant2(2.82)Aberrant right subclavian artery (n (%))Normal18(3.27)0.712Aberrant1(1.41)Echogenic bowel (n (%))Normal12(2.18)0.378Aberrant0(0)Single umbilical artery (n (%))Normal12(2.18)0.378Aberrant0(0)Echogenic intracardiac focus (n (%))Normal2(0.36)0.012Aberrant3(4.23)Other (n (%))Normal15(2.72)0.239Aberrant0(0)Multiple soft markers (n (%))Normal52(9.44)< 0.001**Aberrant25(35.21)^#^ P < 0.1, *P < 0.05, ** P < 0.01, ***P < 0.001
Table 3. Binary logistic regression analysis of abnormal ultrasound soft markers and prenatal diagnosesRelated factorsBSEWalP-valueOR95% CILowerUpperIncreased NT0.3740.3281.30.2541.4540.7642.765Echogenic intracardiac focus3.0710.94910.4770.00121.5623.358138.453Multiple Soft Markers1.9330.35529.64< 0.0016.9113.44613.861SE* Standard error, OR odds ratio, CI confidence interval; **, P < 0.01; ***, P < 0.001
Fig. 2. Forest plot of abnormal ultrasound soft markers vs. prenatal diagnosis outcomes
Results of chromosome karyotype analysis
A total of 63 cases of the abnormality were diagnosed by the chromosome karyotype analysis with the prevalence of 10.13% (63/622). The largest number of these abnormalities was 47,XN,+21, followed by 47,XN,+18. Apart from aneuploidies, some special chromosomal abnormalities were diagnosed. There were two cases of complex chromosomal mosaicism, namely mos45,X[4]/47,XYY[38]/46,XY[5] and mos45,X[2]/47,XXX[2]/46,XX[57]. Five cases were diagnosed as balanced translocation. Two additional cases were aneuploidy combined translocation, both of which were 46,XX, rob(13;21)(q10;q10),+21. Meanwhile, one small supernumerary marker chromosome was detected, and further testing was required to identify its origin (shown in Table 4).
Table 4. Results of chromosome karyotype analysisUltrasound categoryChromosome karyotype analysis results47, XN, + 2147, XN, + 1845, XO47, XXX47, XXY47, XYYmosaicismtranslocationsaneuploidy combined translocationsmall supernumerary marker chromosomesIncreased NT11241010310Absent nasal bone6000100010Short femur1000000000Choroid plexus cyst0100000000Echogenic intracardiac focus1000002000Aberrant right subclavian artery0000000100Tricuspid regurgitation0000000001Multiple soft markers19500000100Total38841112521
Results of CMA
CMA was performed on 622 prenatal cases with ultrasound soft markers, resulting in the prevalence of 10.45% (65/622). There were 55 cases of aneuploidies, 1 case of the aneuploidy combined pathogenic CNVs, 6 cases of pathogenic CNVs, and 3 cases of likely pathogenic CNVs. The CNVs were associated with duplications of 17q12, 12p13.33p11.23, 16p13.11; deletions of 16p13.12p13.11, 3q29, 16p11.2, 15q11.2 and Xp22.31. The cases diagnosed with pathogenic or likely pathogenic CNVs had ultrasonic phenotypes that included tricuspid regurgitation, increased NT, absent nasal bone, and choroid plexus cyst (shown in Table 5).
Table 5. Results of CNVsFindings on ultrasoundCMASize of CNVs (kb)Pathogenicity1Tricuspid regurgitationarr[GRCh37]16p13.12p13.11(14780640–16527659)x11747Pathogenic2NT 3.8 mmarr[GRCh37]3q29(195718751–197386180)x11667Pathogenic3NT 5.3 mmarr[GRCh37]16p11.2(29567296–30190029)x1623Pathogenic4NT 3.4 mmarr[GRCh37]16p11.2(29351826–30190029)x1838Pathogenic5NT 3.2 mmarr[GRCh37]15q11.2(22582283–23060000)x1478Pathogenic6Absent nasal bonearr[GRCh37]Xp22.31(6537109–8167604)x11630Pathogenic7Absent nasal bonearr[GRCh37]17q12(36466620–37940921)x3,(21)×31470Pathogenic8Tricuspid regurgitationarr[GRCh37]12p13.33p11.23(173786-27350550)x427,177Likely pathogenic9Choroid plexus cystarr[GRCh37]16p13.11(15077292–16178545)x31100Likely pathogenic10Choroid plexus cystarr[GRCh37]16p13.11(14892976–16517413)x41620Likely pathogenic
Resulting comparison of the chromosome karyotype analysis and CMA
In this study, all cases underwent chromosome karyotype analysis and CMA. In most cases, the results of the two tests were consistent, but there were still some cases with different results (shown in Table 6).
For instance, five balanced translocations (cases 1 ~ 5) and one pseudodiploid (case 6) were missed by CMA. In addition, two cases with CMA results of “arr(21)×3” were supplemented by karyotyping (cases 7 and 8).
However, compared to karyotype analysis, CMA diagnosed 9 cases of pathogenic and likely pathogenic CNVs (cases 9 to 17) and supplemented a case initially diagnosed as aneuploidy by karyotype analysis, revealing the presence of both aneuploidy and pathogenic CNV in this case (case 18). It was noteworthy that case 15 was initially diagnosed as a small supernumerary marker chromosome by karyotype analysis and was identified as arr[GRCh37]12p13.33p11.23(173786-27350550) x4 by CMA.
Table 6. Summary of cases with different results from chromosome karyotype analysis and CMAFindings on ultrasoundChromosome karyotype analysisCMA1NT 3.0 mm46,XX, t(11;19)(q25;p13.1)dnNormal2NT 3.3 mm46,XY, t(3;12)(q26.2;q13)dnNormal3NT3.5 mm45,XY, rob(14;15)(q10;q10)Normal4Echogenic intracardiac focus, echogenic bowel46,XX, t(11;22)(q25;q13.1)Normal5Aberrant right subclavian artery46,XX, t(10;13)(q21.2;q32)dnNormal6Echogenic intracardiac focusmos45,X[2]/47,XXX[2]/46,XX[57]Normal7Absent nasal bone46,XX, rob(13;21)(q10;q10),+21arr(21)×38NT 3.5 mm46,XX, rob(13;21)(q10;q10)mat,+21arr(21)×39Tricuspid regurgitationNormalarr[GRCh37]16p13.12p13.11(14780640–16527659)x110NT 3.8 mmNormalarr[GRCh37]3q29(195718751–197386180)x111NT 5.3 mmNormalarr[GRCh37]16p11.2(29567296–30190029)x112NT 3.4 mmNormalarr[GRCh37]16p11.2(29351826–30190029)x113NT 3.2 mmNormalarr[GRCh37]15q11.2(22582283–23060000)x114Absent nasal boneNormalarr[GRCh37]Xp22.31(6537109–8167604)x115Tricuspid regurgitation47,XX,+mararr[GRCh37]12p13.33p11.23(173786-27350550)x416Choroid plexus cystNormalarr[GRCh37]16p13.11(15077292–16178545)x317Choroid plexus cystNormalarr[grch37]16p13.11(14892976–16517413)x418Absent nasal bone47,XX,+21arr[GRCh37]17q12(36466620–37940921)x3,(21)×3
Results of pregnancy outcomes and postnatal follow-up
A follow-up was conducted on the pregnancy outcomes of all 622 cases, confirming the outcomes of 604 cases (excluding 18 lost to follow-up in the prenatal diagnostic negative group). In the group with abnormal prenatal diagnostic results, one case resulted in stillbirth (prenatal ultrasound indicated absent nasal bone), 59 cases underwent termination of pregnancy, and 11 cases resulted in live birth (shown in Fig. 3; Table 7). Secondary follow-up at 3–5 years of age was conducted for the 11 live-born cases, revealing no significant phenotypic abnormalities.
Table 7. Live birth cases with abnormal prenatal diagnostic resultsFindings on ultrasoundChromosome karyotype analysis resultsCMA1Increased NT47,XXXarr(X)×32Increased NT47,XYY[10]/46,XY[11]arr(1–22)×2,(X)×1,(Y)×2[0.5]3Increased NT46,XX, t(11;19)(q25;p13.1)dnNormal4Increased NT47,XYYarr[GRCh37] Yp11.32q11.223(118551_26192662)x2,Yq11.23(27769668_28799654)x25Increased NT45,XY, rob(14;15)(q10;q10)Normal6Echogenic intracardiac focus45,X[2]/47,XXX[2]/46,XX[57]Normal7Echogenic intracardiac focus, echogenic bowel46,XX, t(11;22)(q25;q13.1)Normal8Absent nasal bone46,XXarr[GRCh37] Xp22.31(6537109_8167604)x19Aberrant right subclavian artery46,XX, t(10;13)(q21.2;q32)dnNormal10Choroid plexus cyst46,XYarr[GRCh37] 16p13.11(15077292_16178545)x311Choroid plexus cyst46,XYarr[GRCh37] 16p13.11(14892976_16517413)x4
Fig. 3. Follow-up of pregnancy outcomes
Discussion
This study focuses on the prenatal diagnosis of fetuses with soft markers using the chromosome karyotype analysis and CMA. The overall prevalence of chromosomal abnormalities was found to be 11.41% (71/622), which was consistent with the previous study performed by Cai et al. (10.17%) [4]. Furthermore, our data demonstrate that the prevalence of chromosomal aneuploidy is significantly higher in the multiple soft marker group compared to the isolated soft marker group. Additionally, through statistical analysis, it was found that the echogenic intracardiac focus may exhibit a correlation with chromosomal abnormalities. However, the number of related cases in this study is limited. Therefore, while this result has heightened our attention to the echogenic intracardiac focus, the current cases are insufficient to support the conclusion regarding its correlation with chromosomal abnormalities, and further validation with a larger cohort remains necessary. For increased NT, existing literature has reported a significant association with chromosomal abnormalities [16]. While a certain correlation was observed in this study, it did not reach statistical significance, indicating the need for further investigation with a larger sample size. Based on the finding of this study and existing literature, special attention should be paid to cases with multiple soft markers, echogenic intracardiac focus, the absent nasal bone and the increased NT [4, 7, 16, 17]. For these cases, the invasive diagnostic genetic testing should not be ignored.
5 cases of balanced translocations were diagnosed by chromosome karyotype analysis, and all of them had normal CMA results. This finding offers valuable reference for future reproductive health strategies of these individuals as they mature. Furthermore, the potential risks associated with balanced translocation should be addressed during prenatal genetic counseling. For example, the Philadelphia chromosome, characterized by ABL1-BCR fusion at translocation breakpoints, plays a critical role in leukemogenesis [18, 19]. In addition, a 46,XX, t(4;7)(q27;p22) case with PCDH10 and TNRC18 mutations at the translocation breakpoint presented neurodevelopmental delay, facial dysmorphism and high myopia [20]. Therefore, it is essential to assess the inheritance pattern and the family history, and gene sequencing of breakpoints should be considered for fetuses with de novo mutations. In this study, three of the five cases of the balanced translocation underwent parental genetic verification, and all of them were de novo mutations. Among the five cases, only one underwent pregnancy termination, while the remaining four demonstrated normal physical development during the 3–5year follow-up period. Certainly, their physical condition will be monitored continuously.
In the current study, a limited number of pathogenic and likely pathogenic CNVs were identified, notably including two cases of 16p11.2 deletion syndrome and two cases of 16p13.11 duplication. The 16p11.2 deletion syndrome is mainly manifested as intellectual disability, developmental delay, epilepsy, overweight and spinal deformity, while skeletal deformity, cardiovascular deformity and central nervous system deformity are the predominant phenotypes in fetal period [21, 22]. In this study, both cases of 16p11.2 deletion were associated with increased NT, so as to supplement the fetal phenotype of 16p11.2 deletion cases. The 16p13.11 duplication is a neuro susceptible locus, and the clinical phenotype of patients mainly involves neurological diseases, such as schizophrenia [23]. Although few cases of 16p13.11 duplication fetuses have described phenotypes such as echogenic bowel and corpus callosum agenesis, no established consensus on clinical features exists [24, 25]. Notably, both 16p13.11 duplication cases in this study exhibited choroid plexus cysts, suggesting this finding as a potentially significant fetal phenotype. Both cases were delivered without complications, and a 3-year follow-up revealed no abnormal phenotypic features. However, given the 3-year follow-up limitation, delayed-onset manifestations cannot be entirely ruled out; thus, extended follow-up remains essential.
Additionally, CMA analysis revealed 40 chromosomal variations classified as VUS, including 36 CNVs and 4 UPDs (shown in Supplementary Tables 1 and 2). Given that these variations are classified as VUS and the case presented in this article only involves abnormal ultrasound soft markers, we exercise caution in prenatal interpretations and do not definitively categorize them as chromosomal abnormalities. However, for reference, we present the ultrasound phenotype and CMA results, believing that they will contribute to the accumulation of information regarding the pathogenicity of these variants. It is noteworthy that this study detected 4 UPDs. CMA, which combines array-CGH and SNP-array, is not only capable of diagnosing CNVs but also UPDs, and performs well in prenatal diagnosis.
In recent years, prenatal diagnosis has seen advancements with the introduction of the whole exome sequencing (WES) [26, 27]. Nevertheless, prenatal WES, as a phenotype-dependent testing, is not a routine detection method for detecting fetuses with abnormal ultrasound soft markers. According to the expert consensus, cases with abnormal soft markers are considered for WES testing only when increased NT, especially NT > 4 mm or multiple soft markers are present [28]. Therefore, CMA and karyotype analysis remain the main methods for prenatal diagnosis of fetuses with ultrasound soft markers [29]. Karyotype analysis has the advantages of intuitionistic analysis, especially in the diagnosis of aneuploidy, mosaicism, and chromosomal translocation. CMA can effectively compensate for the problem of low resolution of karyotype analysis, and can detect additional microdeletion, microduplication and UPDs. The combined use of these two tests can help reduce the risk of missing pathogenic variants.
Conclusions
In conclusion, the study underscores the importance for pregnant women who exhibit ultrasound soft markers, particularly those with multiple soft markers, to proactively seek prenatal genetic diagnosis. The synergistic combination of CMA and chromosomal karyotype analysis has proven to be a potent tool in elucidating the underlying genetic factors associated with these soft markers, thereby enabling more informed medical decision-making and tailored care.
Supplementary Information
Supplementary Material 1.
Supplementary Material 2.
Supplementary Material 3.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Application Collaboration Group Of Whole Exome Sequencing In Prenatal D, Lou G, Hou Q, Yang K, Guo L: [Expert consensus on the application of prenatal exome sequencing for fetal structural anomalies]. Zhonghua yi xue yi chuan xue za zhi = Zhonghua yixue yichuanxue zazhi = Chinese journal of medical genetics. 2022;39(5):457–463.10.3760.cma.j.cn 511374-20210920-0076535598257 · doi ↗ · pubmed ↗