Parent-Teen Sexual Health Communication and Teens’ Health Information and Service Seeking
Hannah Javidi, Jorge V. Verlenden, Xiwei Chen, Eric R. Walsh-Buhi

TL;DR
Frequent parent-teen sexual health conversations help teens feel more confident to seek health information and services, but only if parents are informed and comfortable.
Contribution
The study reveals that the impact of parent-teen communication on teen self-efficacy depends on parents' perceived knowledge and comfort.
Findings
Frequent communication increased teen self-efficacy when parents felt informed and comfortable.
Frequent communication decreased teen self-efficacy when parents lacked information or comfort.
Parents with higher education or income were less likely to communicate about sexual health.
Abstract
Is the frequency of parent-teen sexual health communication associated with teens’ self-efficacy to seek sexual and reproductive health (SRH) information and services? In this cross-sectional study of 522 parent-teen dyads, frequent communication was associated with higher teen self-efficacy when parents felt informed and comfortable. When parents did not feel informed or comfortable, frequent communication was associated with decreases in teen self-efficacy. This study suggests that parents must have quality information and strategies to increase comfort around sexual health conversations, which may in turn be associated with higher levels of teens’ confidence to seek SRH information and services when needed. Parent-teen sexual health communication can support and empower teens in their sexual and reproductive health (SRH) decision-making. These conversations may differ in their…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
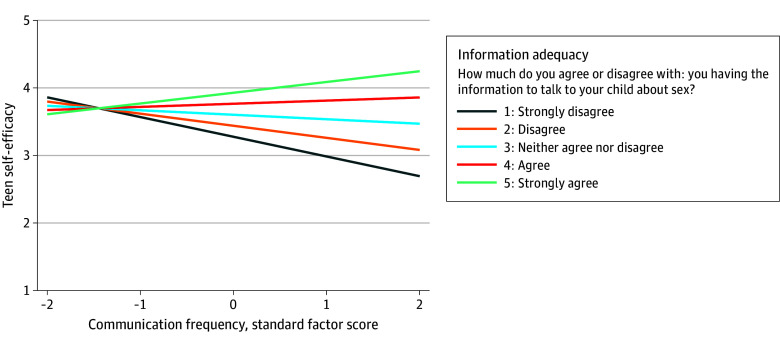 Figure 1
Figure 1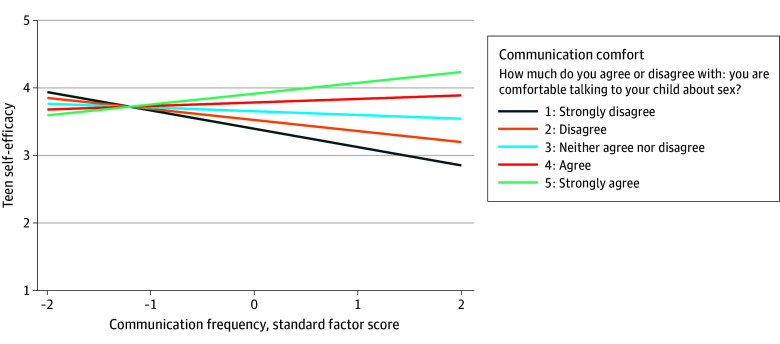 Figure 2
Figure 2| Characteristic | Overall, unweighted No. (% weighted) | Sexual health communication frequency | Perceived sexual health information adequacy | Sexual health communication comfort | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % (95% CI) | % (95% CI) | % (95% CI) | ||||||||||
| Low (≤median) | High (>median) | Inadequate | Ambivalent | Adequate | Discomfort | Ambivalent | Comfort | |||||
|
| ||||||||||||
| Sex | ||||||||||||
| Male | 145 (38.7) | 66.0 (56.3-74.5) | 34.0 (25.5-43.7) | .001 | 3.6 (1.4-9.1) | 18.2 (10.7-29.2) | 78.2 (68.9-85.3) | .58 | 12 (7.7-18.2) | 19.6 (14.0-26.7) | 68.4 (60.0-75.8) | .08 |
| Female | 377 (61.3) | 45.5 (39.8-51.4) | 54.5 (48.6-60.2) | 2.1 (0.7-5.5) | 15.1 (10.6-21.3) | 82.8 (76.4-87.7) | 5.6 (3.7-8.4) | 18.5 (12.6-26.2) | 76.0 (68.1-82.4) | |||
| Age, y | ||||||||||||
| 18-44 | 308 (46.5) | 42.0 (35.6-48.7) | 58.0 (51.3-64.4) | <.001 | 3.9 (1.7-8.6) | 16.3 (11.9-21.9) | 79.8 (73.7-84.8) | .48 | 6.5 (4.0-10.3) | 17.3 (13.0-22.7) | 76.2 (70.3-81.2) | .37 |
| ≥45 | 214 (53.5) | 63.0 (55.8-69.7) | 37.0 (30.3-44.2) | 1.6 (0.4-5.5) | 16.4 (10.1-25.5) | 82.0 (74.0-88.0) | 9.4 (6.1-14.3) | 20.2 (13.8-28.7) | 70.3 (61.6-77.8) | |||
| Race and ethnicity | ||||||||||||
| Black, non-Hispanic | 80 (12.8) | 25.7 (13.4-43.5) | 74.3 (56.5-86.6) | .01 | 4.6 (0.7-23.7) | 26.8 (15.3-42.8) | 68.6 (59.0-76.8) | .05 | 1.5 (0.2-10.3) | 29.8 (21.0-40.3) | 72.3 (65.1-78.6) | .09 |
| Hispanic | 92 (22.7) | 47.6 (35.1-60.4) | 52.4 (39.6-64.9) | 3.7 (0.8-15.4) | 21.1 (11.0-36.8) | 75.2 (59.2-86.4) | 5.5 (2.1-14.0) | 17.9 (8.8-33.2) | 68.8 (58.1-77.7) | |||
| White, non-Hispanic | 309 (57.0) | 60.4 (52.7-67.6) | 39.6 (32.4-47.3) | 1.0 (0.3-2.8) | 12.7 (8.8-18.0) | 86.3 (81.0-90.3) | 9.2 (6.3-13.3) | 18.5 (13.4-25.0) | 76.5 (61.1-87.1) | |||
| Other | 41 (7.5) | 61.8 (37.6-81.4) | 38.2 (18.6-62.4) | 9.2 (3.7-21.3) | 11.6 (4.7-25.9) | 79.2 (64.9-88.7) | 17.8 (7.5-36.6) | 7.6 (2.2-23.0) | 74.6 (56.8-86.7) | |||
| Educational level | ||||||||||||
| Less than Bachelor’s degree | 325 (56.7) | 47.2 (40.4-54.2) | 52.8 (45.8-59.6) | .03 | 2.7 (1.1-6.5) | 17.9 (12.4-25.0) | 79.4 (72.5-84.9) | .39 | 6.1 (3.7-9.9) | 19.2 (13.6-26.5) | 74.7 (66.9-81.2) | .35 |
| Bachelor’s degree or higher | 197 (43.3) | 61.4 (52.1-70.0) | 38.6 (30.0-47.9) | 2.6 (0.9-7.3) | 14.3 (8.6-23.0) | 83.1 (75.9-88.5) | 10.7 (7.0-15.9) | 18.4 (12.0-27.3) | 70.9 (62.4-78.1) | |||
| Household income, $ | ||||||||||||
| <30 000 | 124 (22.3) | 35.5 (27.1-44.9) | 64.5 (55.1-72.9) | <.001 | 4.3 (1.2-14.3) | 20.0 (12.7-30.1) | 75.7 (64.6-84.2) | .51 | 2.6 (0.6-9.7) | 22.2 (13.8-33.6) | 75.3 (63.5-84.2) | .07 |
| 30 000 to <60 000 | 154 (24.9) | 46.6 (36.5-56.9) | 53.4 (43.1-63.5) | 1.9 (0.5-7.2) | 17.5 (10.1-28.5) | 80.7 (70.0-88.2) | 3.7 (1.4-9.3) | 19.1 (12.3-28.4) | 77.2 (67.2-84.9) | |||
| 60 000 to <100 000 | 121 (24.8) | 58.0 (46.4-68.7) | 42.0 (31.3-53.6) | 1.0 (0.3-3.7) | 14.6 (7.9-25.5) | 84.4 (73.8-91.2) | 10.9 (6.2-18.4) | 13.7 (7.0-25.2) | 75.3 (63.8-84.1) | |||
| ≥100 000 | 123 (28.1) | 68.9 (58.9-77.4) | 31.1 (22.6-41.1) | 3.6 (1.1-10.9) | 13.9 (8.4-22.3) | 82.5 (74.8-88.2) | 13.7 (8.3-21.8) | 20.7 (12.5-32.4) | 65.6 (54.8-74.9) | |||
|
| ||||||||||||
| Sex | ||||||||||||
| Male | 244 (50.3) | 49.5 (41.5-57.6) | 50.5 (42.4-58.5) | .11 | 1.8 (0.6-6.0) | 13.8 (8.5-21.7) | 84.3 (77.6-89.3) | .29 | 6.8 (3.9-11.6) | 15.8 (10.7-22.7) | 77.4 (70.2-83.3) | .11 |
| Female | 273 (49.7) | 57.9 (52.4-63.3) | 42.1 (36.7-47.6) | 3.1 (1.3-7.3) | 19.0 (14.2-24.9) | 77.9 (71.9-82.8) | 9.2 (6.3-13.2) | 22.2 (16.8-28.8) | 68.6 (62.1-74.4) | |||
| Sexual orientation | ||||||||||||
| Heterosexual | 394 (79.8) | 50.4 (44.5-56.2) | 49.6 (43.8-55.5) | .09 | 2.3 (1.0-5.1) | 16.9 (12.5-22.5) | 80.8 (75.0-85.6) | .52 | 7.3 (5.0-10.6) | 19.9 (14.9-26.0) | 72.8 (66.3-78.4) | .43 |
| LGB+ | 103 (20.2) | 59.1 (49.3-68.2) | 40.9 (31.8-50.7) | 0.8 (0.2-2.7) | 18.9 (10.4-31.8) | 80.4 (67.6-88.9) | 11.7 (5.9-22.0) | 15.3 (7.4-29.1) | 73.0 (59.5-83.2) | |||
| Model | β (95% CI) | |
|---|---|---|
|
| ||
| Model 1 | ||
| Intercept | 3.83 (3.75 to 3.92) | <.001 |
| Communication frequency | 0.12 (0.04 to 0.20) | <.001 |
| Model 2 | ||
| Intercept | 3.14 (2.69 to 3.59) | <.001 |
| Information adequacy | 0.16 (0.06 to 0.26) | <.001 |
| Model 3 | ||
| Intercept | 3.35 (3.07 to 3.64) | <.001 |
| Communication comfort level | 0.11 (0.05 to 0.18) | <.001 |
|
| ||
| Model 1 | ||
| Intercept | 3.29 (2.80 to 3.78) | <.001 |
| Communication frequency | 0.08 (0.00 to 0.17) | .05 |
| Information adequacy | 0.13 (0.01 to 0.24) | .03 |
| Model 2 | ||
| Intercept | 3.47 (3.15 to 3.79) | <.001 |
| Communication frequency | 0.08 (−0.01 to 0.16) | .09 |
| Communication comfort level | 0.09 (0.01 to 0.17) | .03 |
| Model | β (95% CI) | |
|---|---|---|
|
| ||
| Intercept | 3.11 (2.65 to 3.58) | <.001 |
| Sexual health communication frequency | −0.40 (−0.79 to −0.02) | .04 |
| Sexual health information adequacy | 0.16 (0.06 to 0.27) | <.001 |
| Sexual health communication frequency × sexual health information adequacy | 0.11 (0.03 to 0.20) | .01 |
|
| ||
| Intercept | 3.26 (2.86 to 3.66) | <.001 |
| Sexual health communication frequency | −0.38 (−0.80 to 0.04) | .08 |
| Sexual health communication comfort | 0.13 (0.04 to 0.22) | .01 |
| Sexual health communication frequency × sexual health communication comfort | 0.11 (0.01 to 0.20) | .03 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdolescent Sexual and Reproductive Health · Health Literacy and Information Accessibility · Child Abuse and Trauma
Introduction
Parent-teen sexual health communication (ie, bidirectional communication between parents or parental figures and their teenage children about sex, sexuality, and sexual health outcomes)^1^ can support positive teen sexual health behaviors and outcomes.^2^ Findings from conceptual and meta-analytic reviews indicate that parent-teen sexual health communication is robustly related to teens’ safer-sex cognitions (eg, condom-related attitudes, self-efficacy to resist unwanted sexual encounters) and behaviors, including contraceptive and condom use.^3,4^
By fostering open, frequent dialogue around sex, parents can equip their teens with the knowledge and skills necessary to navigate complex sexual and reproductive health (SRH)–related issues.^5^ One goal of effective parent-teen communication is preparing adolescents for adulthood by empowering them with skills to proactively take their health into their own hands, including the ability to make informed decisions and seek health care when needed.^6,7,8,9^ Studies of interventions designed to strengthen parent-teen sexual health communication suggest that ongoing, quality conversations characterized by openness, comfort, and accurate information can increase knowledge about puberty, promote health decision-making skills, and build understanding of the purpose and importance of receiving sexual health care from a qualified clinician.^10,11^
The effectiveness of these conversations, however, may depend on various factors, including the extent of parents’ knowledge and comfort discussing sexual health topics. Parents who are ill equipped to discuss sexual health with their teens may initiate harmful conversations that are associated with increased risk behavior.^12^ Conversely, parents who feel comfortable and ready to discuss intimacy and sexuality, and who demonstrate openness and nonjudgment in their communication, may provide better support and successfully empower their teens to make healthier decisions around sex and bodily autonomy.^13,14^ However, these factors have not been explored at length in research on associations between sexual communication and teen health outcomes. In addition, sexual communication may differ by sociodemographic characteristics of both parents and teens (eg, age, race and ethnicity, sex).^15,16,17^ Understanding the association of these factors with teens’ self-efficacy to seek SRH information and services is necessary to identify potential disparities and work to address them through tailored initiatives designed to support equitable and effective communication.
The present study aims to investigate the association of the frequency of parent-teen sexual health communication frequency with teens’ self-efficacy to seek SRH information and services in a nationally representative sample of US parents and teens. Self-efficacy (ie, one’s belief in their ability to do something) is a proximal antecedent to health behavior change.^18^ Previous research demonstrates connections between communication and self-efficacy,^19,20^ including information-seeking self-efficacy.^21^ Although existing research addresses teen self-efficacy for sexual behaviors such as condom use and sexual communication,^4^ teen self-efficacy to seek SRH information and services is an underexplored area. We explore 2 potential moderators: parents’ perceived information adequacy and comfort regarding sexual health discussions. We also examine whether parents’ sexual health communication frequency, information adequacy, and comfort differ by a number of sociodemographic variables: parent sex, age, race and ethnicity, educational level, and household income, as well as teen sex and sexual orientation.
Method
Data were collected from parent-teen (aged 15-17 years) dyads participating in the Teen and Parent Surveys of Health. Participants were recruited from AmeriSpeak and AmeriSpeak Teen panels,^22^ which are operated by the National Opinion Research Center (NORC), an independent, nonpartisan research and public policy organization at the University of Chicago.^23^ Panels were designed using probability sampling to be representative of US households. Panel recruitment and management methods are published elsewhere.^23,24^ Of the 2444 invited panelists who completed the screener to determine eligibility for the parent survey, 1230 were determined eligible, and 902 completed informed written consent and were invited to take the survey. Of these, 777 parents completed the survey (June 16 to September 29, 2022; 86.1% response rate). Among teens aged 15 to 17 years, 766 received informed written parental consent and were invited to take the teen survey. Of these, 522 teens completed the survey (May 12 to September 30, 2022; 68.1% response rate), resulting in 522 dyadic pairs. All participants received a cash equivalent of 2 for completing the screener and consent. This study was approved by NORC’s institutional review board and was consistent with applicable federal law and Centers for Disease Control and Prevention (CDC) policy. The study was prepared in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for cross-sectional studies.^25^
Measures
Parents self-reported sex, age, race and ethnicity (Black, non-Hispanic; Hispanic; White, non-Hispanic; and other [participants who reported being multiracial or another race not listed, and were not Hispanic]), educational level, and household income. Race and ethnicity data were collected as part of the standard demographic information gathered from all participants. Teens self-reported sex and sexual orientation. These demographic characteristics were standard questions that all AmeriSpeak panelists receive when they are sampled into the survey. Parents self-reported sexual health communication frequency, information adequacy, and comfort level, and teens self-reported self-efficacy to seek SRH information and services. eTable 1 in Supplement 1 includes item wording and measure operationalization.
Parent-Teen Sexual Health Communication Frequency
The original dataset contained 17 parent-teen communication items with the stem “During the past 12 months, how often have you talked with [child’s name] about each of the following?” Exploratory factor analysis was performed to seek the latent structure underlying parent communication frequency items.^26^ The 17 items were summarized into 2 latent scales: “sexual health communication” (eg, “Where to get healthcare services for sexual and reproductive health, like birth control or sexually transmitted infection testing”) and “other communication” (“How to keep information private while using the internet”). Because 2 items showed relatively lower factor loadings, we removed these and reran the factor analysis. Both factor analyses are reported in eTable 2 in Supplement 1. The resulting 7-item parent-teen sexual health communication frequency scale showed evidence of strong reliability (Cronbach α = 0.93; eTable 3 in Supplement 1).^27^ The factor score was extracted as a standardized normal (mean [SD], 0 [1]) and used for the analyses. Items included: (1) [Your child]’s decisions about whether to have sex; (2) How to create and maintain healthy, respectful romantic relationships; (3) The importance of giving and receiving consent for sex; (4) How to say no to sex; (5) How to prevent pregnancy; (6) How to prevent sexually transmitted infections, including HIV; and (7) Where to get health care services for sexual and reproductive health, like birth control or sexually transmitted infection testing. Parents rated their frequency for each item on a 4-point scale: (1 = more than a few times, 2 = a few times, 3 = once or twice, 4 = never). Items were reverse coded, with higher scores indicating that parents communicate more frequently. eTable 4 in Supplement 1 shows associations between parent demographics and individual communication frequency items.
Parent Information Adequacy
Parents were asked, “How much do you agree or disagree with the following statement?” with the item: “I have the information I need to talk to [child name] about sex.” Parents responded on a 5-point Likert scale (1 = strongly agree, 5 = strongly disagree). The item was reverse coded, with higher scores indicating parents feeling more informed.
Parent Comfort Level
Parents were asked, “How much do you agree or disagree with the following statement?” with the item: “I am comfortable talking to [child name] about sex.” Parents responded on a 5-point Likert scale (1 = strongly agree, 5 = strongly disagree). The item was reverse coded, with higher scores indicating parents feeling more comfortable.
Teen Self-Efficacy to Seek SRH Information and Services
Teens were asked, “How much do you agree or disagree with the following statements?” with 5 items (eTable 1 in Supplement 1). Items included (1) “I am confident that I know where to seek information about sexual and reproductive health”; (2) “I am confident using the internet or telephone to find information about sexual and reproductive health”; (3) “I am confident talking with a healthcare provider, like a doctor or nurse, to get information about sexual and reproductive health”; (4) “I have access to resources (eg, provider, internet, friends) about sexual and reproductive health”; and (5) “I am confident sharing information about sexual and reproductive health with a healthcare provider through virtual platforms (eg, a video call).” Items were rated on a 5-point Likert scale (1 = strongly agree, 5 = strongly disagree), and reverse coded, with higher scores indicating higher self-efficacy. Items were averaged for a total scale score.
Statistical Analysis
Statistical analysis was performed from February to May 2024. The χ^2^ tests assessed whether levels of parent sexual health communication frequency, information adequacy, and comfort level differed by any of our categorical parent-reported and teen-reported demographic variables. For only these analyses, sexual health communication frequency, information adequacy, and communication comfort were treated as categorical to capture demographic group differences among participants (categorization of these variables is presented in the footnotes of Table 1). Univariate and multivariate regression models for parent-reported communication variables and teen self-efficacy were performed. Moderated linear regression analyses evaluated the association between parent sexual health communication frequency and teen self-efficacy to seek SRH information and services, examining the moderating association of 2 prespecified parent variables: information adequacy and communication comfort. Analyses were conducted in Stata, version 18 (StataCorp LLC). All analyses were weighted, and all tests were 2-sided, with statistical significance set at P < .05.
Results
Table 1 displays demographic characteristics of the 522 parents and teens. Parents included 377 women (61.3%) and 145 men (38.7%), were mostly 45 years or older (214 [53.5%]), and identified as non-Hispanic Black (80 [12.8%]), Hispanic (92 [22.7%]), non-Hispanic White (309 [57.0%]), and other race or ethnicity (41 [7.5%]). In terms of educational level, more than half of parents held less than a bachelor’s degree (325 [56.7%]). Over one-fourth of parents reported a household income of $100 000 or more (123 [28.1%]), with the rest distributed across lower income brackets. Among teens, the sample was evenly split by sex (244 male [50.3%] and 273 female [49.7%]), and the majority identified as heterosexual (394 [79.8%]). Approximately 1 in 5 teens (103 [20.2%]) identified as lesbian, gay, bisexual, or another nonheterosexual orientation.
Findings indicated no statistically significant differences in the frequency of parent-reported sexual health communication based on any demographic characteristics of teens; however, frequency differed significantly by parent demographic characteristics (sex, age, race and ethnicity, educational level, and household income). Specifically, female parents had greater likelihood of high-frequency sexual health communication compared with male parents (54.5% [95% CI, 48.6%-60.2%] vs 34.0% [95% CI, 25.5%-43.7%]; P = .001) and parents who were younger (18-44 years) were more likely to communicate frequently compared with parents who were 45 years of age or older (58.0% [95% CI, 51.3%-64.4%] vs 37.0% [95% CI, 30.3%-44.2%]; P < .001) (Table 1). Black parents reported the most frequent communication (74.3% [95% CI, 56.5%-86.6%]) compared with other racial and ethnic groups (Hispanic parents, 52.4% [95% CI, 39.6%-64.9%]; White parents, 39.6% [95% CI, 32.4%-47.3%]; and parents who were multiracial or another race, 38.2% [95% CI, 18.6%-62.4%]; P = .01). Parents who held a bachelor’s degree or higher were less likely to have high sexual health communication frequency compared with parents who had less than a bachelor’s degree (38.6% [95% CI, 30.0%-47.9%] vs 52.8% [95% CI, 45.8%-59.6%]; P = .03). Parents with annual household incomes under 100 000 or more had the lowest likelihood of communicating (31.1% [95% CI, 22.6%-41.1%]; P < .001). There were no statistically significant differences in parents’ information adequacy or comfort level based on parent or teen demographic characteristics.
Table 2 shows the results of both univariate regression models and main effects models with teen self-efficacy as the outcome. In univariate models, communication frequency (β = 0.12 [95% CI, 0.04-0.20]; P < .001), information adequacy (β = 0.16 [95% CI, 0.06-0.26]; P < .001), and communication comfort (β = 0.11 [95% CI, 0.05-0.18]; P < .001) were each positively associated with teen self-efficacy. In main effects models, information adequacy (β = 0.13 [95% CI, 0.01-0.24]; P = .03) and communication comfort (β = 0.09 [95% CI, 0.01-0.17]; P = .03) remained significant, while communication frequency no longer showed a significant association.
Table 3 builds on these findings by showing the associations between parent communication frequency and teen self-efficacy, with communication comfort and information adequacy included as moderators to examine interactions. The association was significantly moderated by both variables; teens whose parents talked frequently had higher self-efficacy to seek SRH information and services when parents felt more informed about the topics (β = 0.11 [95% CI, 0.03-0.20]; P = .01) (Figure 1 and Table 3), and when parents felt more comfortable communicating (β = 0.11 [95% CI, 0.01-0.20]; P = .03) (Figure 2 and Table 3). Slope differences in Figure 1 and Figure 2 indicate that information adequacy and communication comfort each strengthen the positive association between frequent communication and teen self-efficacy to seek SRH information and services. The pattern of results remained the same when adjusting for demographic differences in communication frequency (eTable 5 in Supplement 1).
Teens’ Self-Efficacy to Seek Sexual and Reproductive Health (SRH) Services and Parents’ Frequency of Communication About SRH, Moderated by Parent-Perceived Sexual Health Information AdequacyModeration effects of sexual health information adequacy on the association between parent-teen sexual health communication frequency and teens’ self-efficacy to seek SRH information and services. Sexual health communication frequency was derived from a factor analysis of parent-rated items (see eTable 1 in Supplement 1 for information on operationalization and coding). Higher scores indicate more frequent communication. See the Measures subsection of the Methods section for more detail regarding the teen self-efficacy to seek SRH information and services measure.
Teens’ Self-Efficacy to Seek Sexual and Reproductive Health (SRH) Services and the Frequency of Parents’ Communication About SRH, Moderated by Parent Report of Sexual Health Communication ComfortModeration effects of parents’ comfort with communicating with their teen about sex on the association between parent-teen sexual health communication frequency and teens’ self-efficacy to seek SRH information and services. Sexual health communication frequency was derived from a factor analysis of parent-rated items (see eTable 1 in Supplement 1 for information on operationalization and coding). Higher scores indicate more frequent communication. See the Measures subsection of the Methods section for more detail regarding the teen self-efficacy to seek SRH information and services measure.
Discussion
Parent-teen sexual health communication can be influential in reducing sexual risk behaviors and helping ensure teens are equipped to navigate sexual and reproductive health care systems.^1,3,26^ This study supplements existing literature on frequent parent-teen sexual communication^1,3,4^ by examining associations between parent communication frequency and teen service-seeking self-efficacy, and the relevance of parents’ comfort and information adequacy. Findings indicate that teens whose parents talk frequently about sexual health generally have higher self-efficacy in seeking services related to sexual health, but this association depends on how comfortable and informed parents feel about the topics. This frequent communication can have a positive influence on teens’ confidence to engage in health-supportive behaviors, but if parents do not feel informed or comfortable regarding sexual health topics, then their more frequent communication is associated with lower teen self-efficacy to seek SRH information and services when needed.
As communication about sexual health topics is not uniformly associated with positive teen health outcomes, simply encouraging parents to “talk about sex more” with their teens may not be sufficient. Rather, the present study’s findings highlight a need for interventions that provide parents with knowledge, skills, and support they will need to feel ready to engage in these conversations. Previous research shows that parents may not feel adequately supported to talk with their teens about sexual health or protection against risky sexual behaviors.^28,29^ Programs designed to increase parents’ comfort around talking about sex with their teens and ensure they have access to current, evidence-based sexual health information may help their communication achieve its intended benefits. School-based, health care professional–based, and community-based interventions can involve parents, focusing on enhancing their knowledge about SRH topics and their ability to discuss them.^3,28,30^ Similar interventions have been shown to improve teens’ feelings of parental support and have resulted in fewer behavioral risks.^31^ The CDC’s Division of Adolescent and School Health offers resources for parents, including CDC Healthy Youth Parent Resources and tips for Talking with Your Teen about Sex.^32,33^ Programs with structured workshops or online modules offering a judgment-free setting and concrete strategies for initiating and maintaining open dialogue about SRH topics may increase parents’ knowledge and comfort communicating, although further research is needed to understand how best to implement such interventions.^34,35,36^
Consistent with previous research, mothers (compared with fathers) had a greater likelihood of engaging in sexual health discussions with their teens,^17,28,37,38^ a pattern that may reflect broader norms around gender socialization, where mothers are expected to play a more active role in their children’s upbringing, including providing sexual health education.^39,40,41,42^ Black parents also indicated more frequent discussion about sexual health compared with parents of other racial and ethnic groups. Previous research studies suggest this pattern may be indicative of greater awareness of (and desire to combat) sexual health disparities within Black communities, where Black teens face disproportionately higher rates of HIV or sexually transmitted infections and unintended pregnancies due to structural inequities (eg, limited availability of affordable health care; implicit racial bias among health care professionals).^43,44,45,46^ As one study shows, early and frequent parent-teen sexual health communication is a protective strategy used among Black families to delay sexual initiation and promote safer sexual behavior.^47^ However, there was cultural variability; for example, Haitian families (compared with African American and Jamaican families) expressed lower comfort, value, and breadth of parent-teen sexual health communication.^47^ This finding speaks to the necessity of not treating Black families as a monolith—in general, but particularly in this kind of research. Interventions should be culturally sensitive and tailored to families’ comfort levels and values surrounding sex.^48,49,50^ In addition, because studies have shown that parents of racial and ethnic minority groups report lower effectiveness beliefs concerning their sexual health communication, future research should seek to identify specific barriers that parents of racial and ethnic minority groups face and work to eliminate these barriers.^28,51,52^
Our study also found that parents with lower educational levels and annual incomes discussed sexual health topics more frequently; this may result from attempts to fill gaps in their teens’ education if the families do not have access to high-quality sex education programs. Younger parents (<45 years) also reported more frequent communication, potentially indicating a shift in cultural norms surrounding open sexual communication. Together, these findings illustrate factors shaping parent-teen communication dynamics, and prompt a need for more exploration of these factors, how they intersect, and how we could design and deliver interventions to promote effective, equitable sexual health communication within families. Studies may also consider teens’ perceptions more in depth, as factors such as teens’ trust in their parents and comfort discussing sex with them may also be associated with the effectiveness of these conversations.
Limitations and Strengths
This study has several limitations. First, while our sample was designed to be representative of US households, the surveys were offered only in English, and parental consent was required for teen participation, which may have led to sampling bias or exclusion.^53,54^ Second, the small sample size limited analyses among certain demographic subgroups, possibly resulting in suppression of differences. Even so, previous studies of parent-teen sexual communication have relied on convenience or nonrandom samples,^55^ so our use of a probability-based sample may strengthen generalizability of findings. Third, sexual health communication frequency reported by parents may be influenced by social desirability bias and subsequently result in underestimation or overestimation of communication. We must also consider the possibility of overlap in participants’ interpretations of the response options for this measure. For example, a parent who discussed a sexual health topic 4 to 6 times within the past year may have considered this “a few times,” while another parent with the same actual communication frequency considered this “more than a few times,” resulting in potential variability within response categories. Fourth, our outcome measure focused on teens’ self-efficacy to seek SRH information and services, rather than the act of service seeking. Despite theoretical and empirical evidence positioning self-efficacy as a key factor associated with health behavior,^56,57,58,59^ our findings do not speak to whether teens engaged in that behavior. In other words, even if teens feel confident in their ability to seek health services, there may be other barriers and situational factors preventing them from doing so when necessary.^60^ Fifth, our parent-perceived information adequacy variable relies on self-reported adequacy, which may or may not accurately reflect the actual accuracy of the information parents have. Despite these limitations, to our knowledge, this cross-sectional study is the first to assess parents’ perceived information adequacy and comfort with sexual health communication as moderators for the association between the frequency of parent-teen sexual health communication and teen-reported self-efficacy to seek SRH information and services. The study’s dyadic nature helped ensure incorporation of both parent and teen perspectives and can strengthen development of interventions that aim to optimize teens’ health and quality of life.^61^
Conclusions
In this cross-sectional study, the frequency with which parents spoke to their children about sex and sexual health was associated with teens’ self-efficacy to seek sexual health information and services, as long as parents were informed and comfortable talking about these topics. Our findings suggest that parents need to have quality information about sexual health and effective strategies to increase their comfort in having these discussions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Flores D, Barroso J. 21st Century parent-child sex communication in the United States: a process review. J Sex Res. 2017;54(4-5):532-548. doi:10.1080/00224499.2016.1267693 28059568 PMC 5808426 · doi ↗ · pubmed ↗
- 2Ashcraft AM, Murray PJ. Talking to parents about adolescent sexuality. Pediatr Clin North Am. 2017;64(2):305-320. doi:10.1016/j.pcl.2016.11.002 28292447 PMC 5517036 · doi ↗ · pubmed ↗
- 3Widman L, Choukas-Bradley S, Noar SM, Nesi J, Garrett K. Parent-adolescent sexual communication and adolescent safer sex behavior: a meta-analysis. JAMA Pediatr. 2016;170(1):52-61. doi:10.1001/jamapediatrics.2015.2731 26524189 PMC 4857605 · doi ↗ · pubmed ↗
- 4Rogers AA. Parent–adolescent sexual communication and adolescents’ sexual behaviors: a conceptual model and systematic review. Adolesc Res Rev. 2017;2(4):293-313. doi:10.1007/s 40894-016-0049-5 · doi ↗
- 5Mc Callister CJ, Akers AY, Worlds AD, Morrison PK. Messages about contraception and condoms in mother-adolescent dyadic conversations: knowledge, risks, and effectiveness. J Pediatr Adolesc Gynecol. 2019;32(4):395-401. doi:10.1016/j.jpag.2019.02.117 30779964 · doi ↗ · pubmed ↗
- 6Hurst JL, Widman L, Maheux AJ, Evans-Paulson R, Brasileiro J, Lipsey N. Parent-child communication and adolescent sexual decision making: an application of family communication patterns theory. J Fam Psychol. 2022;36(3):449-457. doi:10.1037/fam 0000916 34472938 · doi ↗ · pubmed ↗
- 7Sneed CD, Tan HP, Meyer JC. The influence of parental communication and perception of peers on adolescent sexual behavior. J Health Commun. 2015;20(8):888-892. doi:10.1080/10810730.2015.1018584 25951343 · doi ↗ · pubmed ↗
- 8Suldo SM, Fefer SA. Parent-child relationships and well-being. In: Proctor C, Linley PA, eds. Research, Applications, and Interventions for Children and Adolescents. Springer Netherlands; 2013:131-147.