Antimicrobial Susceptibility Profile of Klebsiella pneumoniae Isolates From a Tertiary Care Hospital: A Retrospective Study
Kumudini Panigrahi, Basanti Kumari Pathi, Jyoti Prakash Sahoo

TL;DR
This study analyzed antibiotic resistance patterns in Klebsiella pneumoniae from a hospital, finding high resistance to some drugs and better sensitivity to others.
Contribution
The study provides updated antimicrobial susceptibility data for K. pneumoniae isolates in a specific hospital setting.
Findings
Tigecycline showed the highest susceptibility among K. pneumoniae isolates.
Hospital-acquired infections were four times more common than community-acquired infections.
High resistance was observed against ciprofloxacin, cefuroxime, and ceftriaxone.
Abstract
Background and objectives: Globally, drug resistance has been growing in number and severity. Klebsiella pneumoniae is one of the multidrug-resistant organisms (MDROs) found in healthcare settings, especially in intensive care units (ICUs). We mapped this study to determine the antimicrobial susceptibility testing (AST) patterns of K. pneumoniae isolates found in our hospital. We also determined the AST findings of the ICU and non-ICU patients and those with hospital-acquired infection (HAI) and community-acquired infection (CAI). Methods: This retrospective study was conducted from October 2022 to September 2024 at Kalinga Institute of Medical Sciences (KIMS), Bhubaneswar, India. We included adult inpatients with positive culture reports for K. pneumoniae. All specimens (blood, urine, endotracheal tube (ETT), body fluid, sputum, pus, wound, and skin swabs) from the eligible…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
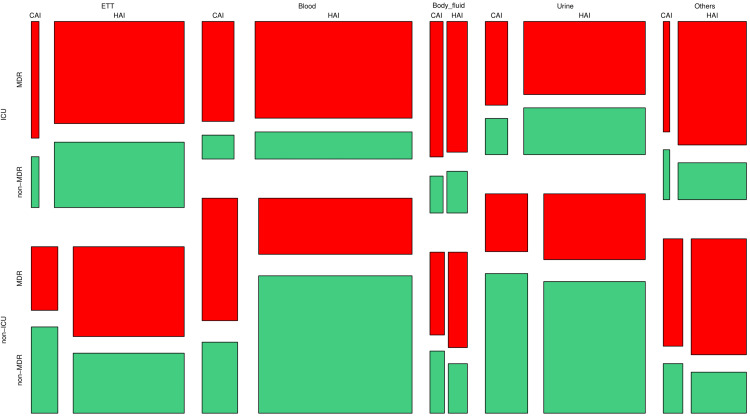 Figure 1
Figure 1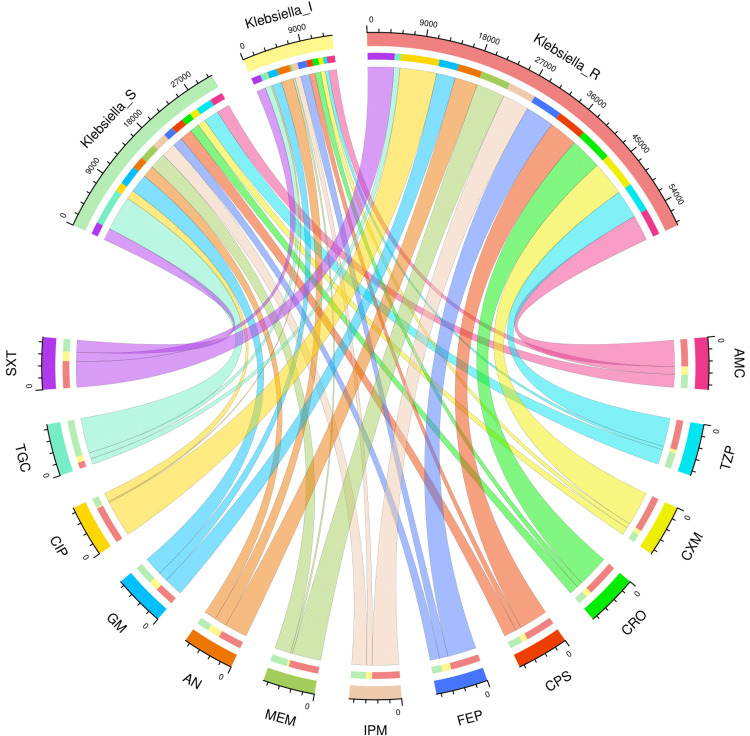 Figure 2
Figure 2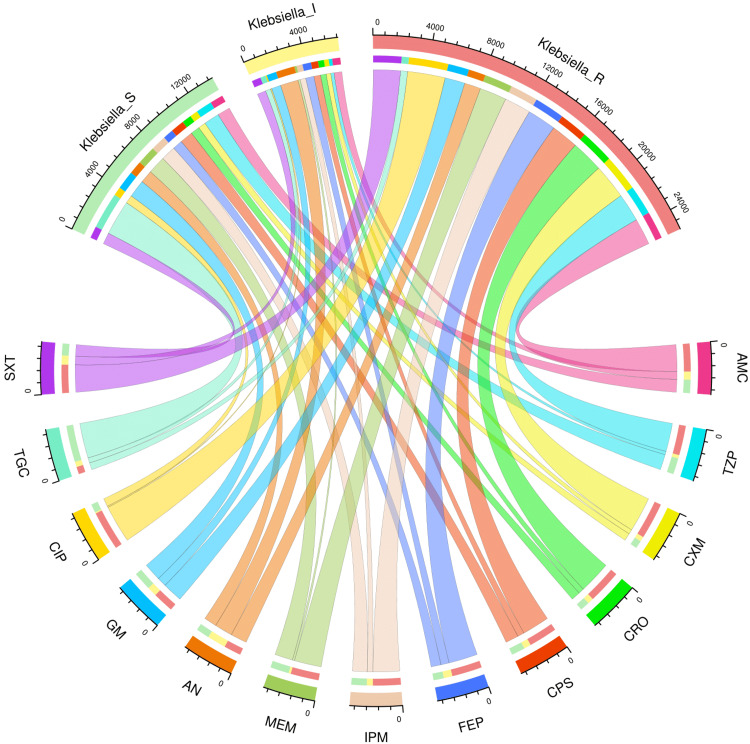 Figure 3
Figure 3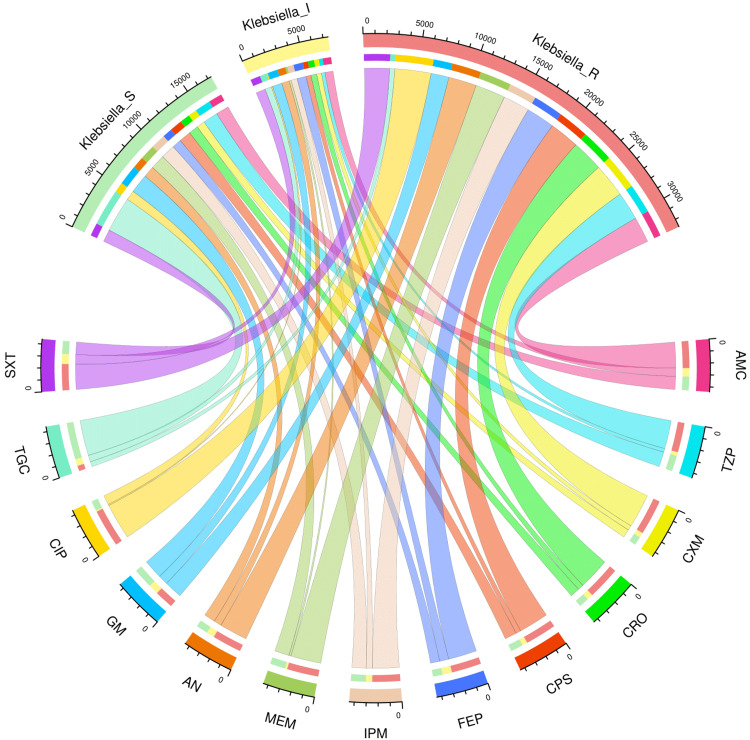 Figure 4
Figure 4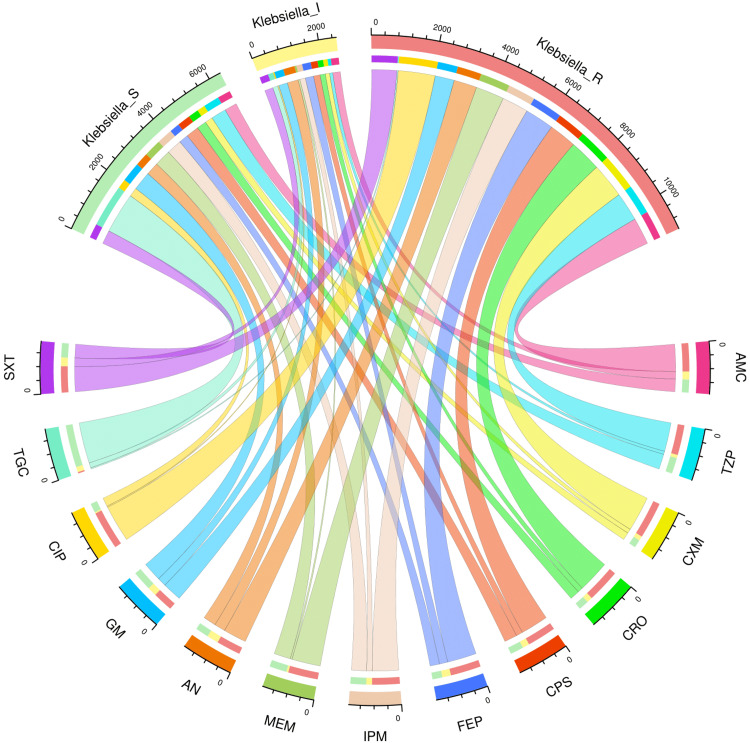 Figure 5
Figure 5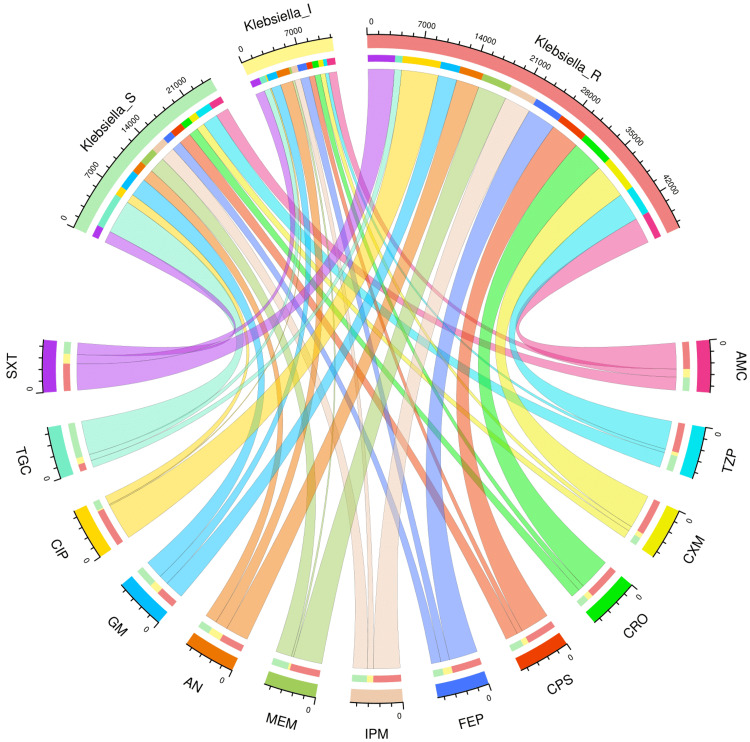 Figure 6
Figure 6| Parameter | Value |
| Total participants | 7,942 |
| Age (years) | 53.50 (39.75-63.25) |
| Male | 4,948 (62.30%) |
| Samples collected (positive for | |
| ETT | 1,887 (23.76%) |
| Blood | 2,591 (32.62%) |
| Body fluid | 462 (5.82%) |
| Urine | 1,975 (24.87%) |
| Others | 1,027 (12.93%) |
| Location | |
| ICU | 3,523 (44.36%) |
| Non-ICU | 4,419 (55.64%) |
| Infection type | |
| CAI | 1,541 (19.40%) |
| HAI | 6,401 (80.60%) |
| Drug resistance status | |
| MDR | 4,418 (55.63%) |
| Non-MDR | 3,524 (44.37%) |
| Susceptibility type | AMC | TZP | CXM | CRO | CPS | FEP | IPM | MEM | AN | GM | CIP | TGC | SXT |
| Total (n = 7,942) | |||||||||||||
| Sensitive | 2,178 (27.42%) | 2,576 (32.44%) | 1,342 (16.90%) | 1,577 (19.86%) | 2,099 (26.43%) | 1,623 (20.44%) | 2,444 (30.77%) | 2,727 (34.34%) | 2,017 (25.40%) | 3,133 (39.45%) | 1,516 (19.08%) | 5,940 (74.79%) | 2,022 (25.46%) |
| Intermediate | 1,349 (16.99%) | 581 (7.32%) | 791 (9.96%) | 968 (12.19%) | 978 (12.31%) | 1,471 (18.52%) | 1,006 (12.67%) | 351 (4.42%) | 2,061 (25.95%) | 1,616 (20.35%) | 199 (2.50%) | 1,003 (12.63%) | 1,544 (19.44%) |
| Resistant | 4,415 (55.59%) | 4,785 (60.25%) | 5,809 (73.14%) | 5,397 (67.96%) | 4,865 (61.26%) | 4,848 (61.04%) | 4,492 (56.56%) | 4,864 (61.25%) | 3,864 (48.65%) | 3,193 (40.20%) | 6,227 (78.40%) | 999 (12.57%) | 4,376 (55.10%) |
| ICU (n = 3,523) | |||||||||||||
| Sensitive | 951 (26.99%) | 1,161 (32.95%) | 564 (16.01%) | 677 (19.22%) | 975 (27.68%) | 745 (21.15%) | 1,107 (31.42%) | 1,345 (38.18%) | 955 (27.11%) | 1,325 (37.61%) | 611 (17.34%) | 2,618 (74.31%) | 853 (24.21%) |
| Intermediate | 583 (16.55%) | 243 (6.90%) | 345 (9.79%) | 424 (12.04%) | 504 (14.31%) | 618 (17.54%) | 428 (12.15%) | 159 (4.51%) | 1,345 (38.18%) | 700 (19.87%) | 91 (2.58%) | 384 (10.90%) | 648 (18.39%) |
| Resistant | 1,989 (56.46%) | 2,119 (60.15%) | 2,614 (74.20%) | 2,422 (68.75%) | 2,044 (58.02%) | 2,160 (61.31%) | 1,988 (56.43%) | 2,019 (57.30%) | 1,223 (34.71%) | 1,498 (42.52%) | 2,821 (80.07%) | 521 (14.79%) | 2,022 (57.39%) |
| Non-ICU (n = 4,419) | |||||||||||||
| Sensitive | 1,227 (27.76%) | 1,415 (32.02%) | 778 (17.60%) | 900 (20.37%) | 1,124 (25.44%) | 878 (19.87%) | 1,337 (30.26%) | 1,382 (31.27%) | 1,062 (24.03%) | 1,808 (40.91%) | 905 (20.48%) | 3,322 (75.18%) | 1,169 (26.45%) |
| Intermediate | 766 (17.33%) | 338 (7.65%) | 446 (10.09%) | 544 (12.31%) | 474 (10.73%) | 853 (19.30%) | 578 (13.08%) | 192 (4.34%) | 716 (16.20%) | 916 (20.73%) | 108 (2.44%) | 619 (14.00%) | 896 (20.28%) |
| Resistant | 2,426 (54.90%) | 2,666 (60.33%) | 3,195 (72.30%) | 2,975 (67.32%) | 2,821 (63.84%) | 2,688 (60.83%) | 2,504 (56.66%) | 2,845 (64.39%) | 2,641 (59.77%) | 1,695 (38.36%) | 3,406 (77.08%) | 478 (10.82%) | 2,354 (53.27%) |
| CAI (n = 1,541) | |||||||||||||
| Sensitive | 409 (26.54%) | 498 (32.32%) | 251 (16.29%) | 317 (20.57%) | 419 (27.90%) | 313 (20.31%) | 495 (32.12%) | 545 (35.37%) | 421 (27.32%) | 621 (40.23%) | 291 (18.89%) | 1,333 (86.50%) | 447 (29.01%) |
| Intermediate | 248 (16.09%) | 102 (6.62%) | 141 (9.15%) | 173 (11.23%) | 216 (14.02%) | 273 (17.72%) | 181 (11.75%) | 59 (3.83%) | 362 (23.49%) | 290 (18.82%) | 39 (2.53%) | 166 (10.77%) | 276 (17.91%) |
| Resistant | 844 (57.35%) | 941 (61.06%) | 1,149 (74.56%) | 1,051 (68.20%) | 906 (58.79%) | 955 (61.97%) | 865 (56.13%) | 937 (60.80%) | 758 (49.19%) | 630 (40.88%) | 1,211 (78.59%) | 42 (2.73%) | 818 (53.08%) |
| HAI (n = 6,401) | |||||||||||||
| Sensitive | 1,769 (27.64%) | 2,078 (32.46%) | 1,091 (17.04%) | 1,260 (19.68%) | 1,680 (26.25%) | 1,310 (20.47%) | 1,949 (30.45%) | 2,182 (34.09%) | 1,596 (24.93%) | 2,512 (39.24%) | 1,225 (19.13%) | 4,607 (71.97%) | 1,575 (24.60%) |
| Intermediate | 1,101 (17.20%) | 479 (7.48%) | 650 (10.15%) | 795 (12.42%) | 762 (11.90%) | 1,198 (11.72%) | 825 (12.89%) | 292 (4.56%) | 1,699 (26.54%) | 1,326 (20.72%) | 160 (2.50%) | 837 (13.08%) | 1,268 (19.81%) |
| Resistant | 3,531 (55.16%) | 3,844 (60.05%) | 4,660 (72.80%) | 4,346 (67.90%) | 3,959 (61.85%) | 3,893 (60.82%) | 3,627 (56.67%) | 3,927 (61.35%) | 3,106 (48.52%) | 2,563 (40.04%) | 5,016 (78.36%) | 957 (14.95%) | 3,558 (55.59%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Resistance in Bacteria · Antibiotic Use and Resistance · Nosocomial Infections in ICU
Introduction
Antimicrobial resistance (AMR) is a worldwide threat that challenges breakthroughs across multiple disciplines [1]. Among the Enterobacterales, Klebsiella pneumoniae is one of the most prevalent multidrug-resistant organisms (MDROs) [1,2]. Klebsiella species are rod-shaped, nonmotile, Gram-negative bacteria. These are commensals of the mouth, nasopharynx, and gastrointestinal system in humans [3,4]. Pneumonia, urinary tract infections (UTIs), meningitis, skin and soft tissue infections, liver abscesses, and endophthalmitis are the common diseases caused by Klebsiella species [3,5]. Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and *Enterobacter *spp (ESKAPE) pathogens cause the majority of the hospital-acquired infections (HAIs). K. pneumoniae is the "K" in that group [6,7]. Globally, most drug-resistant infections are brought on by extended-spectrum beta-lactamase (ESBL) and carbapenemase-producing K. pneumoniae [7-9].
Cell wall protein receptors and lipopolysaccharides (LPS) contribute to the pathogenicity of K. pneumoniae. These elements mediate the binding process to host cells and enable protection against the human immune system [10]. The antibiotic resistance of bacteria is grouped into the following three categories: multidrug-resistant (MDR), extensively drug-resistant (XDR), and pandrug-resistant (PDR). MDR K. pneumoniae develops resistance towards at least one antimicrobial from three different drug classes. XDR K. pneumoniae strains are resistant to at least one antibiotic from most antibiotic classes. PDR K. pneumoniae isolates are resistant to each drug in all antibiotic groups [11-13]. The nosocomial infections by K. pneumoniae are increasing in the ICUs [10,14]. Moreover, the MDR K. pneumoniae strains are most frequently seen in the ICUs [10,15].
Community-acquired infection (CAI) can be described as an infection either incubating or present during hospitalization or within 48 hours of admission. The infection that develops after 48 hours of hospitalization is regarded as HAI [16,17]. Nowadays, K. pneumoniae is one of the leading causes of HAI and CAI [18-22]. Recently, Sharma et al. [23] and Kaur et al. [24] discovered new trends in antimicrobial susceptibility testing (AST) findings of K. pneumoniae isolates in India. We planned this study to evaluate the prevalence of infections caused by K. pneumoniae in our hospital and the AST findings of those bacterial isolates. We also determined the AST findings of the K. pneumoniae isolates of ICU and non-ICU patients and those with HAI and CAI.
Materials and methods
Study design
This retrospective study was conducted between October 2022 and September 2024 at Kalinga Institute of Medical Sciences (KIMS), Bhubaneswar, India. The Institutional Ethics Committee of Kalinga Institute of Medical Sciences (KIMS), Bhubaneswar, India, granted us ethical clearance to begin the study (KIIT/KIMS/IEC/1917/2024, dated 23.10.2024). The study complied with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline, the Declaration of Helsinki, Good Laboratory Practices, and institutional norms.
Patient recruitment
We scrutinized the laboratory data of the adult patients having positive culture reports who got admitted to our hospital during the above-mentioned period. Only those patients who had positive K. pneumoniae culture reports were analysed. The AST findings of those isolates were assessed. Inadequate samples and outpatients were excluded.
Data collection
Blood, endotracheal tube (ETT), body fluid, and urine samples were collected and sent to the microbiological laboratory. Following Gram staining, respiratory and body fluid samples were inoculated into blood agar and MacConkey agar. Then they were incubated overnight with 5% CO_2_ in an incubator. Blood samples were incubated within the BacT/Alert 3D machine (bioMérieux, Marcy-l'Étoile, France). They were cultivated on MacConkey agar and sheep blood agar following a positive flag. Urine samples were inoculated on cystine-lactose-electrolyte deficient (CLED) agar. MacConkey agar and blood agar were used to inoculate other specimens, e.g., pus, wound swab, nasal swab, and skin swab. All of the samples were incubated for 24-48 hours at 37°C. Strains of K. pneumoniae were distinguished by their biochemical and morphological traits. Using the Clinical and Laboratory Standard Institute (CLSI) 2022 cut-off values [25], the VITEK 2 system (bioMérieux, Marcy-l'Étoile, France) was utilized to identify isolates and assess antimicrobial susceptibility. AST functions through micro-broth dilution. The term "minimum inhibitory concentration" (MIC) refers to the highest dilution of an antibiotic that inhibits the growth of the organism. Validated software was used to interpret the growth kinetics and MIC data of K. pneumoniae isolates. All data were collected from the microbiology laboratory and analysed.
Statistical analysis
This retrospective study was accomplished using convenience sampling. All patients admitted between October 2022 and September 2024 were scrutinized. Those having positive culture reports for K. pneumoniae were considered for analysis. The Kolmogorov-Smirnov test was used to ascertain the normality of the data distribution. We calculated the continuous data's median and interquartile range (IQR). For the categorical data, we computed the frequency and proportion. We created a mosaic plot to show the participants' distribution. Clinical samples (blood, ETT, urine, body fluids, or others), location (ICU or non-ICU), infection type (HAI or CAI), and medication resistance status (MDR or non-MDR) were the parameters used for preparing the mosaic plot. The AST patterns of K. pneumoniae isolates from the entire research population and different subgroups were shown using chord diagrams. The R Program (Vienna, Austria) version 4.4.3 was used for data analysis and plot generation [26]. p-values less than 0.05 were interpreted as statistically significant.
Results
We screened only the 50,057 culture-positive reports of the patients admitted during the stipulated duration. Out of 13,547 positive blood samples, 2,591 (19.13%) were positive for K. pneumoniae. A total of 1,975 (11.17%) of 17,683 urine samples and 1,887 (30.27%) of 6,234 ETT samples were positive for K. pneumoniae. Of 4,971 positive body fluid samples, 462 (9.29%) were positive for K. pneumoniae. A total of 1,027 (13.47%) of the other 7,622 positive samples were sputum, nasal swab, pus, bronchoalveolar lavage (BAL), wound, and skin samples. The study profile is shown in Table 1. The median age of the participants was 53.50 (39.75-63.25) years. Our study had 4,948 (62.30%) male patients. Of the 7,942 positive samples collected, the most common sample was blood (2,591, 32.62%), followed by urine (1,975, 24.87%), ETT (1,887, 23.76%), and body fluid (462, 5.82%). Other samples, like sputum, nasal swabs, pus, bronchoalveolar lavage (BAL), wound, and skin samples, comprised 1,027 (12.93%) of all positive samples. A total of 3,523 (44.36%) participants were admitted to the ICU. The incidences of CAI and HAI in our hospital were 1,541 (19.40%) and 6,401 (80.60%). MDR cases were 4,418 (55.63%).
Distribution of the study population
Figure 1 shows the participants’ distribution via a mosaic plot. We segregated the study population with the following parameters: sample used (ETT, blood, body fluid, urine, or others), location (ICU or non-ICU), infection type (CAI or HAI), and drug resistance status (MDR or non-MDR). The order of the division was sample collected, location, infection type, and resistance status. The most frequent samples (positive for K. pneumoniae) were obtained from blood (2,591, 32.62%), followed by urine (1,975, 24.87%), ETT (1,887, 23.76%), and body fluid (462, 5.82%). The largest block represents the non-ICU patients with HAI and blood culture positive for non-MDR K. pneumoniae (911, 11.47%), followed by the ICU patients with HAI and blood culture positive for MDR K. pneumoniae (656, 8.26%), the non-ICU patients with HAI and urine culture positive for non-MDR K. pneumoniae (578, 7.28%), and the ICU patients with HAI and ETT culture positive for MDR K. pneumoniae (573, 7.21%).
Distribution of the study populationThe mosaic plot showcases the study participants’ distribution per the sample used (ETT, blood, body fluid, urine, or others), location (ICU or non-ICU), infection type (CAI or HAI), and drug resistance status (MDR or non-MDR). ETT: endotracheal tube, ICU: intensive care unit, CAI: community-acquired infection, HAI: hospital-acquired infection, MDR: multidrug resistance.
AST patterns of the study population and various subgroups
Figures 2-6 demonstrate the AST patterns of K. pneumoniae isolates via chord diagrams. Among the 7,942 K. pneumoniae isolates detected in our study population (Figure 2), the highest sensitivity was seen towards tigecycline (5,940, 74.79%), followed by gentamicin (3,133, 39.45%), meropenem (2,727, 34.34%), and piperacillin-tazobactam (2,576, 32.44%). The resistance was the maximum against ciprofloxacin (6,227, 78.40%), followed by cefuroxime (5,809, 73.14%), and ceftriaxone (5,397, 67.96%). The drug resistance was the least against tigecycline (999, 12.57%). Among the 3,523 K. pneumoniae isolates detected in our ICU participants (Figure 3), the highest sensitivity was seen towards tigecycline (2,618, 74.31%), followed by meropenem (1,345, 38.18%), gentamicin (1,325, 37.61%), and piperacillin-tazobactam (1,161, 32.95%). The resistance was the maximum against ciprofloxacin (2,821, 80.07%), followed by cefuroxime (2,614, 74.20%), and ceftriaxone (2,422, 68.75%). The drug resistance was the least against tigecycline (521, 14.79%). Among the 4,419 K. pneumoniae isolates detected in our non-ICU participants (Figure 4), the highest sensitivity was seen towards tigecycline (3,322, 75.18%), followed by gentamicin (1,808, 40.91%), piperacillin-tazobactam (1,415, 32.02%), meropenem (1,382, 31.27%), and imipenem (1,337, 30.26%). The resistance was the maximum against ciprofloxacin (3,406, 77.08%), followed by cefuroxime (3,195, 72.30%), and ceftriaxone (2,975, 67.32%). The drug resistance was the least against tigecycline (478, 10.82%). Among the 1,541 K. pneumoniae isolates detected in the participants with CAI (Figure 5), the highest sensitivity was seen towards tigecycline (1,333, 86.50%), followed by gentamicin (621, 40.23%), meropenem (545, 35.37%), piperacillin-tazobactam (498, 32.32%), and cotrimoxazole (447, 29.01%). The resistance was the maximum against ciprofloxacin (1,211, 78.59%), followed by cefuroxime (1,149, 74.56%), and ceftriaxone (1,051, 68.20%). The drug resistance was the least against tigecycline (42, 2.73%). Among the 6,401 K. pneumoniae isolates detected in the participants with HAI (Figure 6), the highest sensitivity was seen towards tigecycline (4,607, 71.97%), followed by gentamicin (2,512, 39.24%), meropenem (2,182, 34.09%), and piperacillin-tazobactam (2,078, 32.46%). The resistance was the maximum against ciprofloxacin (5,016, 78.36%), followed by cefuroxime (4,660, 72.80%), and ceftriaxone (4,346, 67.90%). The drug resistance was the least against tigecycline (957, 14.95%). Table 2 narrates the frequencies and proportions of all K. pneumoniae specimens and their AST findings.
AST findings of Klebsiella pneumoniae isolates found among the study participants (n = 7,942)The lower and upper sections represent 13 drugs (shown in different colours) and three types of antibiotic susceptibility (S: sensitive, I: intermediate, and R: resistant) of Klebsiella pneumoniae isolates found in the entire study population (n = 7,942). The widths of the bands correspond with the number of Klebsiella pneumoniae isolates and their AST patterns for the 13 drugs. AST: antimicrobial sensitivity testing, AMC: amoxicillin-clavulanic acid, TZP: piperacillin-tazobactam, CXM: cefuroxime, CRO: ceftriaxone, CPS: cefoperazone-sulbactam, FEP: cefepime, IPM: imipenem, MEM: meropenem, AN: amikacin, GM: gentamicin, CIP: ciprofloxacin, TGC: tigecycline, SXT: cotrimoxazole.
AST findings of Klebsiella pneumoniae isolates found among the ICU patients (n = 3,523)The lower and upper sections represent 13 drugs (shown in different colours) and three types of antibiotic susceptibility (S: sensitive, I: intermediate, and R: resistant) of Klebsiella pneumoniae isolates found in the ICU patients (n = 3,523). The widths of the bands correspond with the number of Klebsiella pneumoniae isolates and their AST patterns for the 13 drugs. ICU: intensive care unit, AST: antimicrobial sensitivity testing, AMC: amoxicillin-clavulanic acid, TZP: piperacillin-tazobactam, CXM: cefuroxime, CRO: ceftriaxone, CPS: cefoperazone-sulbactam, FEP: cefepime, IPM: imipenem, MEM: meropenem, AN: amikacin, GM: gentamicin, CIP: ciprofloxacin, TGC: tigecycline, SXT: cotrimoxazole.
AST findings of Klebsiella pneumoniae isolates found among the non-ICU patients (n = 4,419)The lower and upper sections represent 13 drugs (shown in different colours) and three types of antibiotic susceptibility (S: sensitive, I: intermediate, and R: resistant) of Klebsiella pneumoniae isolates found in the non-ICU patients (n = 4,419). The widths of the bands correspond with the number of Klebsiella pneumoniae isolates and their AST patterns for the 13 drugs. ICU: intensive care unit, AST: antimicrobial sensitivity testing, AMC: amoxicillin-clavulanic acid, TZP: piperacillin-tazobactam, CXM: cefuroxime, CRO: ceftriaxone, CPS: cefoperazone-sulbactam, FEP: cefepime, IPM: imipenem, MEM: meropenem, AN: amikacin, GM: gentamicin, CIP: ciprofloxacin, TGC: tigecycline, SXT: cotrimoxazole.
AST findings of Klebsiella pneumoniae isolates found among the patients with CAI (n = 1,541)The lower and upper sections represent 13 drugs (shown in different colours) and three types of antibiotic susceptibility (S: sensitive, I: intermediate, and R: resistant) of Klebsiella pneumoniae isolates found in the patients with CAI (n = 1,541). The widths of the bands correspond with the number of Klebsiella pneumoniae isolates and their AST patterns for the 13 drugs. CAI: community-acquired infection, AST: antimicrobial sensitivity testing, AMC: amoxicillin-clavulanic acid, TZP: piperacillin-tazobactam, CXM: cefuroxime, CRO: ceftriaxone, CPS: cefoperazone-sulbactam, FEP: cefepime, IPM: imipenem, MEM: meropenem, AN: amikacin, GM: gentamicin, CIP: ciprofloxacin, TGC: tigecycline, SXT: cotrimoxazole.
AST findings of Klebsiella pneumoniae isolates found among the patients with HAI (n = 6,401)The lower and upper sections represent 13 drugs (shown in different colours) and three types of antibiotic susceptibility (S: sensitive, I: intermediate, and R: resistant) of Klebsiella pneumoniae isolates found in the patients with HAI (n = 6,401). The widths of the bands correspond with the number of Klebsiella pneumoniae isolates and their AST patterns for the 13 drugs. HAI: hospital-acquired infection, AST: antimicrobial sensitivity testing, AMC: amoxicillin-clavulanic acid, TZP: piperacillin-tazobactam, CXM: cefuroxime, CRO: ceftriaxone, CPS: cefoperazone-sulbactam, FEP: cefepime, IPM: imipenem, MEM: meropenem, AN: amikacin, GM: gentamicin, CIP: ciprofloxacin, TGC: tigecycline, SXT: cotrimoxazole.
Discussion
The AST findings of 7,942 adult patients with positive culture reports for K. pneumoniae were gauged. All types of clinical samples were considered for analysis in this retrospective study. Out of 50,057 samples positive for bacterial growth, 7,942 (15.87%) were positive for K. pneumoniae. Blood samples contribute to the majority of the positive culture reports. The study population comprised 4,948 (62.30%) males and 2,994 (37.70%) females. The participants’ average age was 53.50 (39.75-63.25) years. A total of 3,523 (44.36%) participants were admitted to the ICU. The incidence of HAI was around four times higher than that of CAI. The MDR cases were more prevalent in ICU patients (2,460, 30.97%) than in non-ICU patients (1,958, 24.65%). Tigecycline (5,940, 74.79%) demonstrated the maximum efficacy against K. pneumoniae isolates, followed by gentamicin (3,133, 39.45%), meropenem (2,727, 34.34%), and piperacillin-tazobactam (2,576, 32.44%). Ciprofloxacin (6,227, 78.40%), cefuroxime (5,809, 73.14%), and ceftriaxone (5,397, 67.96%) were the drugs against which K. pneumoniae isolates were highly resistant. The drug resistance was the least against tigecycline (999, 12.57%). Male preponderance and similar AST patterns of K. pneumoniae isolates had been observed in our earlier research paper [27]. Our AST findings matched the studies by Sharma et al. [23] and Kaur et al. [24].
Like other pathogens in the ESKAPE group,* K. pneumoniae* causes multiple infections like pneumonia, respiratory tract infection (RTI), UTI, skin and soft tissue infections, and meningitis [5]. The risks of morbidity and mortality due to these infections are higher for critically ill patients in the ICUs. Excessive and irrational usage of broad-spectrum antibiotics and India’s enormous population might have fuelled the MDR bacteria across the country [23,28,29]. In K. pneumoniae, the blaKPC genes exist mainly on plasmids, reducing susceptibility to nearly all beta-lactam antibiotics [30]. Age, infection source, underlying disease, polypharmacy, duration and frequency of antibiotics, non-compliance with hospital antimicrobial policy, and production of biofilms influence the incidence of CAI, HAI, and AMR [31,32].
The subgroup analyses yielded a few observations that differed from the study population's findings. The patients with HAI had similar AST patterns as the whole study population. For ICU patients, sensitivity was higher for meropenem than for gentamicin and piperacillin-tazobactam. For non-ICU patients, piperacillin-tazobactam was more effective than meropenem. The sensitivity of K. pneumoniae isolates towards cotrimoxazole was higher among those with CAI. However, the resistance against ciprofloxacin, cefuroxime, and ceftriaxone remained the highest for the entire study population and all four subgroups.
The pluses of our study were data analysis for ICU and non-ICU patients, those with CAI and HAI, and data interpretation via mosaic plot and chord diagrams. Our study could have been improved regarding certain aspects. First, the data was collected only from the microbiology laboratory. Hence, the AST findings could not be correlated with the prescribed antimicrobials. We could not trace the duration of stay or the outcome of the patients. Second, we could not perform whole-genome sequencing (WGS) because of the large study population and retrospective design. Third, we excluded Klebsiella species other than K. pneumoniae due to their low incidence. Fourth, we could not assess the impact of diagnosis, comorbidities, and concomitant medications on AST findings.
Conclusions
The majority of samples positive for K. pneumoniae were obtained from blood, urine, and ETT. The incidence of HAI was four times that of CAI. MDR cases were more prevalent in ICUs. K. pneumoniae isolates showed high susceptibility towards tigecycline, gentamicin, meropenem, and piperacillin-tazobactam. The maximum resistance was seen against ciprofloxacin, cefuroxime, and ceftriaxone. We recommend prospective studies to determine the genetic association of growing antimicrobial resistance among K. pneumoniae strains.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clinical outcomes and bacterial characteristics of carbapenem-resistant Klebsiella pneumoniae complex among patients from different global regions (CRACKLE-2): a prospective, multicentre, cohort study Lancet Infect Dis Wang M Earley M Chen L 4014122220223476775310.1016/S 1473-3099(21)00399-6PMC 8882129 · doi ↗ · pubmed ↗
- 2Mortality risk factors and prognostic analysis of patients with multi-drug resistant Enterobacterales infection Infect Drug Resist Wang X Li Q Kang J 322532371520223575478610.2147/IDR.S 366808 PMC 9231684 · doi ↗ · pubmed ↗
- 3Klebsiella species: taxonomy, hypervirulence and multidrug resistancee Bio Medicine Dong N Yang X Chan EW Zhang R Chen S 1039987920223540538710.1016/j.ebiom.2022.103998 PMC 9010751 · doi ↗ · pubmed ↗
- 4Pathogenic potential of environmental Klebsiella pneumoniae isolates Environ Microbiol Struve C Krogfelt KA 584590620041514224610.1111/j.1462-2920.2004.00590.x · doi ↗ · pubmed ↗
- 5Finding order in the chaos: outstanding questions in Klebsiella pneumoniae pathogenesis Infect Immun Gonzalez-Ferrer S Peñaloza HF Budnick JA Bain WG Nordstrom HR Lee JS Van Tyne D 02089202110.1128/IAI.00693-20PMC 809096533558323 · doi ↗ · pubmed ↗
- 6ESKAPE pathogens: antimicrobial resistance, epidemiology, clinical impact and therapeutics Nat Rev Microbiol Miller WR Arias CA 5986162220243883103010.1038/s 41579-024-01054-w PMC 13147291 · doi ↗ · pubmed ↗
- 7Genomic dissection of Klebsiella pneumoniae infections in hospital patients reveals insights into an opportunistic pathogen Nat Commun Gorrie CL Mirčeta M Wick RR 30171320223564152210.1038/s 41467-022-30717-6PMC 9156735 · doi ↗ · pubmed ↗
- 8Colonization with extended spectrum beta-lactamase and carbapenemases producing Enterobacteriaceae among hospitalized patients at the global level: a systematic review and meta-analysis P Lo S One Abera D Alemu A Mihret A Negash AA Abegaz WE Cadwell K 018202310.1371/journal.pone.0293528 PMC 1068125538011148 · doi ↗ · pubmed ↗