A Diagnostic Puzzle: Unveiling Tuberculosis Peritonitis in an Immunocompromised Patient
André Pereira, Inês Peixoto, Ana Silva, Rosa Cardoso, Helena Sarmento

TL;DR
This case study highlights the difficulty in diagnosing abdominal tuberculosis in an HIV-positive patient and emphasizes the importance of peritoneal biopsy for accurate diagnosis.
Contribution
The paper presents a case where peritoneal biopsy was crucial for diagnosing TB peritonitis in an HIV-positive patient with atypical symptoms.
Findings
Ascitic fluid analysis was negative for TB, but peritoneal biopsy confirmed granulomatous inflammation and M. tuberculosis.
The patient showed favorable clinical improvement after starting anti-tuberculous therapy.
Abdominal TB should be considered in immunocompromised patients with unexplained ascites.
Abstract
Tuberculosis (TB) remains a leading cause of infectious morbidity and mortality worldwide. Extrapulmonary TB, particularly abdominal TB, is a diagnostic challenge due to its nonspecific presentation and often low sensitivity for conventional tests. Immunocompromised patients, such as those with human immunodeficiency virus (HIV), are at increased risk and may lack classic systemic symptoms, preventing timely diagnosis. A 61-year-old HIV-positive female on antiretroviral therapy and with an undetectable viral load presented with progressive abdominal distension, postprandial fullness, and altered bowel habits over two months. Physical examination revealed ascites and a right supraclavicular lymphadenopathy. Laboratory findings showed normocytic anemia, thrombocytosis, hypoalbuminemia, and elevated inflammatory markers. Computed tomography demonstrated large-volume ascites, bilateral…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
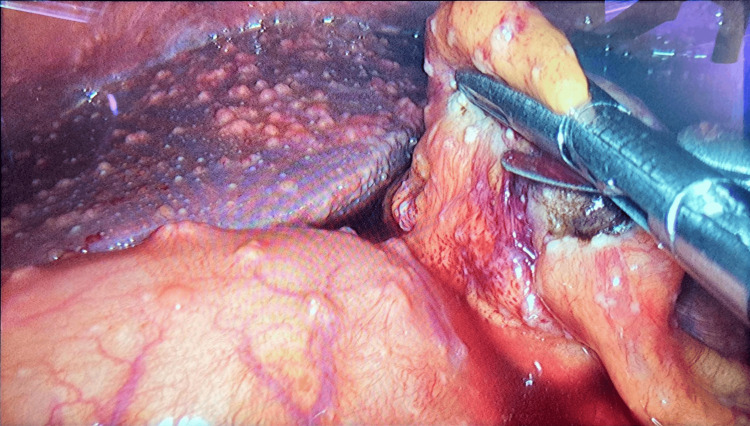 Figure 1
Figure 1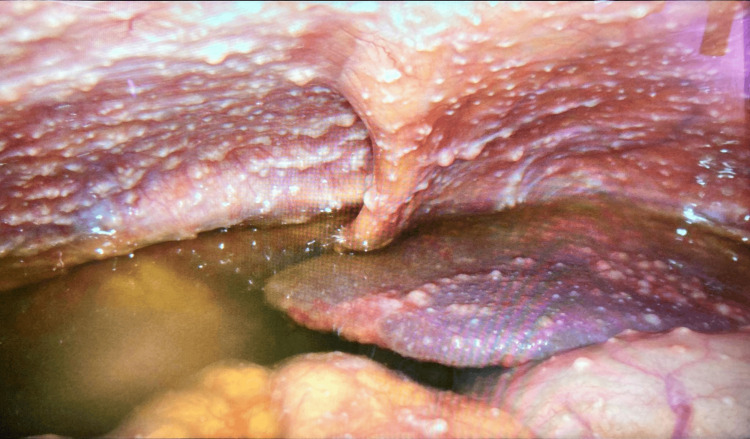 Figure 2
Figure 2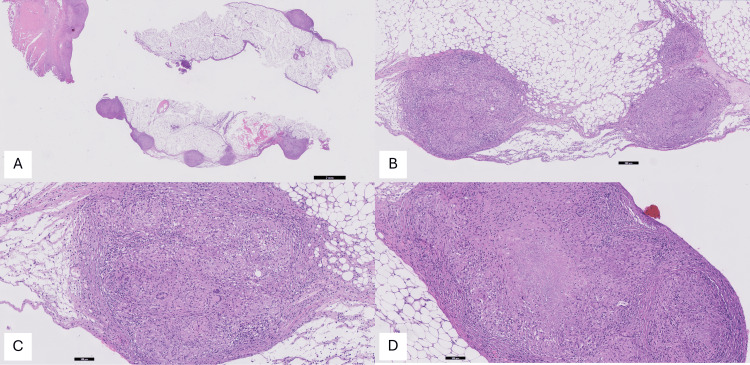 Figure 3
Figure 3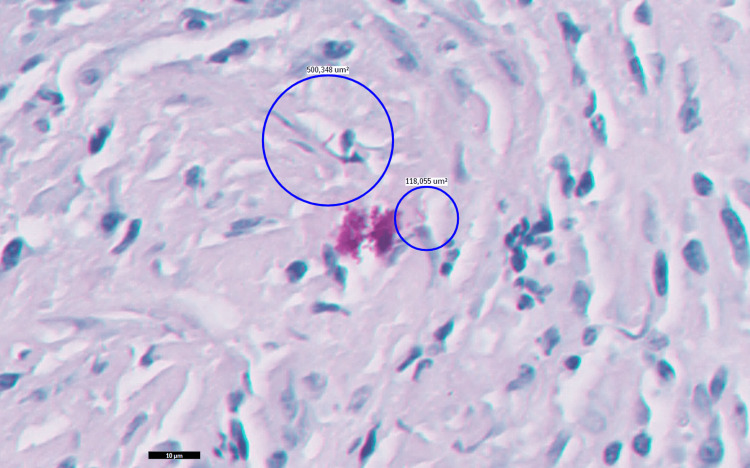 Figure 4
Figure 4| Test | Result | Reference Range |
| Hemoglobin (g/dL) | 9.5 | 14.0–18.0 |
| Hematocrit (%) | 29.2 | 41–53 |
| MCV (fL) | 74.3 | 83–103 |
| MCHC (g/dL) | 32.5 | 32.0–36.0 |
| WBC (×103/µL) | 5.0 | 4.8–10.8 |
| Neutrophils (×10³/µL) | 2.9 | 1.8–7.7 |
| Eosinophils (×10³/µL) | 0.0 | 0.00–0.49 |
| Basophils (×10³/µL) | 0.0 | 0.0–0.1 |
| Lymphocytes (×10³/µL) | 1.7 | 1.0–4.8 |
| Monocytes (×10³/µL) | 0.3 | 0.12–0.80 |
| Platelets (×10³/µL) | 467 | 150–350 |
| Urea (mg/dL) | 20 | 15–39 |
| Creatinine (mg/dL) | 0.65 | 0.55–1.02 |
| Sodium (mEq/L) | 139 | 135–136 |
| Potassium (mEq/L) | 4.7 | 3.5–5.1 |
| Chloride (mEq/L) | 101 | 95–105 |
| Total Bilirubin (mg/dL) | 0.58 | 0.3–1.2 |
| Direct Bilirubin(mg/dL) | 0.24 | 0.0–0.3 |
| AST (U/L) | 25 | 12–40 |
| ALT (U/L) | 10 | 7–40 |
| GGT (U/L) | 22 | 0–38 |
| LDH (U/L) | 241 | 120–246 |
| CRP (mg/L) | 138.1 | <3.0 |
| Albumin (g/dL) | 2.8 | 3.4–5.0 |
| Prothrombin time (sec) | 14.3 | 8.4–14.4 |
| INR | 1.2 | - |
| APTT (sec) | 29.7 | 20.9–34.9 |
| Test | Result |
| Cell count | |
| RBC (µL) | 1,600 |
| WBC (µL) | 352 |
| PMN/mononuclear cells | 15.6%/84.4% |
| Other nucleated cells | 9 |
| Biochemistry | |
| pH | 7.52 |
| Glucose (mg/dL) | 69 |
| Albumin (g/dL) | 1.9 |
| Total proteins (g/dL) | 6.3 |
| LDH (U/L) | 220 |
| ADA (U/L) | 124.4 |
| Test | Result | Reference range |
| Folate (ng/mL) | 2.3 | >5.38 |
| Vitamin B12 (pg/mL) | 612 | 211–911 |
| Serum iron (µg/dL) | 12 | 50–170 |
| TIBC (µg/dL) | 125 | 250–425 |
| Transferrin (mg/dL) | 77 | 250–380 |
| TSAT (%) | 9.6 | 15–50 |
| Ferritin (ng/mL) | 472.8 | 10–291 |
| Lymphocyte Subset | Result | Reference Range |
| T cells (µL) | 64.61% (786) | 49.0–81.0% (527–2846) |
| CD4 T cells (µL) | 40.32% (489) | 28.0–51.0% (332–1642) |
| CD8 T cells (µL) | 23.91% (290) | 12.0–38.0% (170–811) |
| B cells (µL) | 9.64% (118) | 7–32% (78–899) |
| NK cells (µL) | 25.38% (310) | 6–29% (67–1134) |
| CD4/CD8 Ratio | 1.69 | - |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiagnosis and treatment of tuberculosis · Infectious Diseases and Tuberculosis · Intraperitoneal and Appendiceal Malignancies
Introduction
Tuberculosis (TB) remains one of the leading infectious causes of morbidity and mortality worldwide, despite being a preventable and curable disease [1,2]. According to the World Health Organization (WHO), an estimated 10.8 million people developed TB in 2023, with 1.09 million deaths among HIV-negative individuals and an additional 161,000 deaths among those living with HIV [1].
The clinical presentation of TB is heterogeneous, influenced by the site of infection, the host's immune status, and the disease burden [2,3]. Extrapulmonary TB may manifest with more subtle or organ-specific symptoms, postponing prompt diagnosis [3].
Abdominal TB is a form of extrapulmonary TB that involves the gastrointestinal tract, peritoneum, intra-abdominal lymph nodes, and visceral organs, either singly or in combination [4-6]. This TB manifestation accounts for 1% to 3% of all TB cases worldwide and represents 6% to 13% of extrapulmonary TB cases, with rates varying by geography [5]. The condition typically arises from the reactivation of latent *Mycobacterium tuberculosis *infection or via hematogenous or lymphatic dissemination from a primary pulmonary focus [5,6].
In HIV-positive patients, abdominal TB is increasingly recognized, with reported gastrointestinal involvement ranging from 1.7% to 19.7% in China and up to 71% in symptomatic cohorts in sub-Saharan Africa. Yet, large-scale epidemiological data remain limited [7-9].
Timely diagnosis and initiation of standard anti-TB therapy are crucial to prevent complications such as intestinal obstruction, fistula formation, or perforation [5,10]. This case underscores the importance of considering abdominal TB in patients presenting with chronic or unexplained abdominal symptoms, especially among individuals with known risk factors.
Case presentation
A 61-year-old autonomous Black female from a middle-to-low-income background, an immigrant from Angola, and living in Portugal for the past four years, presented to the emergency department with a two-month history of increased abdominal circumference, associated with postprandial fullness and decreased stool frequency. She denied fever, nausea, vomiting, anorexia, or weight loss.
Past medical history included a sexually acquired HIV-1 infection, on antiretroviral therapy (elvitegravir, emtricitabine, tenofovir alafenamide, and cobicistat) with irregular follow-up since 2019, and arterial hypertension. Her last immunovirological assessment in 2019 showed a CD4 count of 612/µL (21.16%) and an undetectable HIV-1 viral load. No history of alcohol or drug abuse.
On physical examination, the patient was hemodynamically stable and afebrile. A painless, right-sided, infracentimetric supraclavicular lymphadenopathy was noted. The abdomen was distended, with shifting dullness and a positive fluid wave test, evidence of ascites.
Laboratory evaluation revealed normocytic normochromic anemia, thrombocytosis, hypoalbuminemia, and elevated C-reactive protein (Table 1).
Abdominopelvic computed tomography (CT) demonstrated moderate bilateral pleural effusion, large-volume ascites, and imaging features suggestive of chronic liver disease (liver heterogeneity with left and caudate lobe hypertrophy).
Given the patient's presentation with new-onset ascites, the initial differential diagnoses included portal hypertension secondary to cirrhosis, peritoneal carcinomatosis, tuberculous peritonitis, and, less likely, pancreatic or cardiac causes. A diagnostic paracentesis was performed, yielding clear yellow peritoneal fluid, which was sent for cytological and microbiological analysis. Ascitic fluid analysis revealed 352 leukocytes/µL, with a predominance of mononuclear cells. Biochemical analysis showed elevated adenosine deaminase (ADA) and a low serum-ascites albumin gradient (SAAG: 0.9 g/dL) (Table 2). In view of the lymphocytic predominance, high ADA level, and low SAAG (findings suggestive of an exudative, non-portal hypertensive etiology), TB peritonitis became a strong diagnostic consideration given the HIV history. Accordingly, the ascitic fluid was subsequently sent for *Mycobacterium tuberculosis *polymerase chain reaction (PCR) testing.
The patient was admitted for clinical monitoring and further etiological investigation.
On day one, the peripheral blood smear was unremarkable. Hematinic studies revealed folate deficiency and elevated ferritin levels (Table 3). Lymphocyte subset analysis revealed a CD4 count of 489/µL (40.32%), and the HIV-1 RNA level was undetectable (Table 4). By day four, cytological, microbiological, and PCR analyses for *M. tuberculosis *in the ascitic fluid were negative.
On day five, upper gastrointestinal endoscopy revealed gastric antral mucosa with areas of erythema and a few scattered erosions, findings consistent with superficial chronic gastritis.
Given the inconclusive non-invasive workup, a laparoscopic peritoneal biopsy was performed on day nine, revealing multiple peritoneal implants disseminated throughout the abdominal cavity, including the *omentum *and intestinal loops (Figures 1, 2). Two tissue samples, one from the parietal peritoneum in the right hypochondrium and another from the greater *omentum *in the left hypochondrium, were submitted for histopathological examination and PCR testing for M. tuberculosis.
LaparoscopyPresence of multiple implants throughout the parietal peritoneum, greater omentum, and Glisson's capsule.
LaparoscopyPresence of multiple implants throughout the parietal peritoneum.
Quadruple anti-TB therapy was initiated, consisting of rifabutin, isoniazid, pyrazinamide, and ethambutol. PCR analysis of the peritoneal tissue confirmed the presence of M. tuberculosis. Histopathological findings from the peritoneal biopsy are illustrated in Figures 3, 4.
Light microscopy (hematoxylin/eosin)(A) Peritoneal adipose tissue exhibiting granulomatous inflammation (0.5x); (B) Peritoneal adipose tissue displaying three distinct fibrotic nodules, each containing centrally located granulomas with multinucleated Langhans-type giant cells, consistent with granulomatous inflammation (5x); (C) Histological section demonstrating fibrotic tissue containing granulomas with three multinucleated Langhans-type giant cells (10×); (D) Fibrotic tissue with peripheral aggregates of epithelioid histiocytes/macrophages exhibiting abundant cytoplasm. The central area shows necrosis, a hallmark feature of tuberculosis-associated granulomas (10×).
Light microscopy (Ziehl-Neelsen 100×)Red-stained bacilli observed on Ziehl-Neelsen staining, compatible with Mycobacterium species.
The patient was subsequently referred to a Pulmonology Diagnostic Center for continuation of anti-TB therapy and to an Infectious Diseases consultation for specialized follow-up. The clinical course was favorable, with complete resolution of the ascites after six months of therapy.
Discussion
Abdominal TB remains a significant diagnostic challenge due to its highly variable clinical presentation and the frequent overlap of symptoms with other intra-abdominal conditions such as malignancies, chronic liver disease, and inflammatory bowel disorders [5-10]. Although pulmonary TB remains the most common manifestation, extrapulmonary involvement accounts for approximately 15-20% of TB cases globally [5]. Geographic variability plays an important role, as higher rates are observed in endemic regions, particularly among immunocompromised populations [1,5].
Building upon this epidemiological context, understanding the underlying mechanisms of abdominal TB is essential for accurate diagnosis. The pathogenesis of abdominal TB involves multiple potential routes of infection. The most widely accepted mechanisms include reactivation of latent *M. tuberculosis *infection, hematogenous dissemination from a primary pulmonary focus, and lymphatic spread from mesenteric nodes [4-6]. Less commonly, direct ingestion of infected sputum or contiguous extension from adjacent organs may contribute. Immunosuppressed individuals, particularly those living with HIV, have an increased susceptibility to extrapulmonary TB due to impaired cellular immunity [3,11]. In our patient, this factor likely played a key role, as HIV infection may have contributed both to disease development and to the atypical clinical presentation observed.
Given these pathophysiological mechanisms, diagnosis of abdominal TB is often delayed due to nonspecific clinical manifestations, such as abdominal distension, altered bowel habits, fever, and weight loss, which can mimic alternative diagnoses, including peritoneal carcinomatosis and cirrhosis [5,6]. In this case, the subacute onset of ascites and nonspecific gastrointestinal symptoms complicated the initial evaluation, leading to a broad differential diagnosis and necessitating a systematic diagnostic approach.
Ascitic fluid analysis remains a cornerstone in the evaluation of suspected TB peritonitis but is inherently limited by low sensitivity in paucibacillary disease [4-6,12]. Typical findings include a lymphocyte-predominant exudate with a low SAAG, as observed in our patient. Of the available biomarkers, ADA is considered one of the most reliable surrogate markers for TB peritonitis. A recent meta-analysis demonstrated that ADA levels above 100 U/L have high specificity for abdominal TB, making this a valuable diagnostic adjunct in clinical practice [12]. In our case, despite negative microbiological and PCR results, the markedly elevated ADA level (124.4 U/L) strongly supported the suspicion of TB peritonitis.
Abdominopelvic imaging is a critical adjunct in the evaluation of suspected abdominal TB. While not pathognomonic, it can demonstrate highly suggestive features, including peritoneal thickening, nodularity, ascites, omental caking, and intra-abdominal lymphadenopathy [5,10]. Such findings contribute to raising clinical suspicion and guiding further invasive testing, although imaging alone rarely establishes a definitive diagnosis [10].
When non-invasive tests are inconclusive, laparoscopic peritoneal biopsy becomes pivotal, with diagnostic yields exceeding 90% [4,5,10]. In our case, laparoscopic evaluation revealed multiple peritoneal implants, and histopathology demonstrated caseating granulomatous inflammation, while PCR confirmed the presence of M. tuberculosis, ultimately securing a conclusive diagnosis.
Importantly, HIV infection substantially modifies the clinical course and therapeutic approach in abdominal TB. In addition to increasing susceptibility, HIV often masks classic systemic features such as fever, night sweats, and weight loss, leading to delayed recognition [11]. Furthermore, therapeutic decisions are complicated by potential drug-drug interactions between rifamycins and antiretroviral therapy [2,5]. In this patient, careful regimen selection was required, and rifabutin was chosen instead of rifampicin to minimize these interactions, consistent with current recommendations [2,5].
Once the diagnosis is established, standard anti-TB therapy remains the mainstay of management. The standard six-month regimen, comprising a two-month intensive phase with isoniazid, rifamycin, pyrazinamide, and ethambutol followed by a four-month continuation phase with isoniazid and rifamycin, achieves high treatment success rates [2,5]. In cases of HIV co-infection, early initiation of antiretroviral therapy alongside TB treatment is associated with improved survival [11]. Our patient demonstrated complete clinical recovery, with resolution of ascites, following the prompt initiation of therapy, highlighting the importance of early recognition, individualized management, and timely treatment initiation.
Conclusions
This case exemplifies the diagnostic complexity of abdominal TB, particularly in the context of HIV co-infection. While ascitic fluid ADA measurement is a valuable diagnostic adjunct, definitive diagnosis often requires peritoneal biopsy. Clinicians should maintain a high index of suspicion for abdominal TB in patients presenting with unexplained ascites and relevant risk factors. Early diagnosis and appropriate anti-TB therapy remain paramount to improving patient outcomes and preventing serious complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global Tuberculosis Report Global Tuberculosis Report World Health Organization Geneva, Switzerland World Health Organization 2024 https://www.who.int/publications/i/item/9789240101531
- 2Tuberculosis Lancet Furin J Cox H Pai M 1642165639320193090426210.1016/S 0140-6736(19)30308-3 · doi ↗ · pubmed ↗
- 3Clinical heterogeneity and treatment outcomes of extrapulmonary tuberculosis in a low-incidence setting: insights from a prospective cohort study Infection Klingmüller A Feldmann M Rohr S 180918185320254006756910.1007/s 15010-025-02500-4PMC 12460547 · doi ↗ · pubmed ↗
- 4Abdominal tuberculosis of the gastrointestinal tract: revisited World J Gastroenterol Debi U Ravisankar V Prasad KK Sinha SK Sharma AK 14831148402020142535604310.3748/wjg.v 20.i 40.14831 PMC 4209546 · doi ↗ · pubmed ↗
- 5Abdominal tuberculosis Stat Pearls [Internet] Tobin E Khatri A Treasure Island (FL)Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 556115/32310575 · pubmed ↗
- 6Gastrointestinal tuberculosis Microbiol Spectr Choi EH Coyle WJ 4201610.1128/microbiolspec.TNMI 7-0014-201628084201 · doi ↗ · pubmed ↗
- 7Epidemiology of tuberculosis and HIV coinfection among inpatients in Chengdu, China, 2018-2022 BMC Infect Dis Tang XZ Ma Y Ma Y 10432520254083043310.1186/s 12879-025-11316-4PMC 12366068 · doi ↗ · pubmed ↗
- 8Clinical and ultrasonographic features of abdominal tuberculosis in HIV positive adults in Zambia BMC Infect Dis Sinkala E Gray S Zulu I 44920091937475710.1186/1471-2334-9-44PMC 2678139 · doi ↗ · pubmed ↗