Efficacy and Safety of Rezafungin Versus Caspofungin for the Treatment of Candidemia and Invasive Candidiasis in a China Cohort of a Double‐Blind, Randomised, Phase 3 Trial (ReSTORE China)
Haihui Huang, Sizhou Feng, Yunsong Yu, Yong Zhang, Yuan Yuan, Laura Cox, Yingyuan Zhang

TL;DR
A clinical trial in China found that rezafungin is as effective and safe as caspofungin for treating candidemia and invasive candidiasis.
Contribution
The study confirms rezafungin's noninferiority to caspofungin in a China-specific cohort, supporting its potential as a new treatment option.
Findings
All-cause mortality at Day 30 was 33.3% for rezafungin and 35.7% for caspofungin.
Global cure at Day 14 was 48.1% for rezafungin and 46.4% for caspofungin.
Mycological eradication rates were comparable between the two drugs.
Abstract
The global double‐blind, randomised, Phase 3 ReSTORE trial (NCT03667690) demonstrated noninferiority of rezafungin versus caspofungin for all‐cause mortality at Day 30 and global cure at Day 14 in patients with candidemia and/or invasive candidiasis. We report outcomes for patients from China (ReSTORE China), comprising participants enrolled in the original ReSTORE trial (n = 11) and from an extended, China‐only phase (n = 47) implemented to fulfill Chinese regulatory requirements. Patients with candidemia/invasive candidiasis were randomised 1:1 to intravenous rezafungin (400 mg loading, then 200 mg once weekly) or caspofungin (70 mg loading, then 50 mg once daily) for ≤ 4 weeks. Primary endpoints were all‐cause mortality at Day 30 and global cure at Day 14 in the modified intent‐to‐treat population. Between October 2018 and March 2024, 58 patients were randomised and received study…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
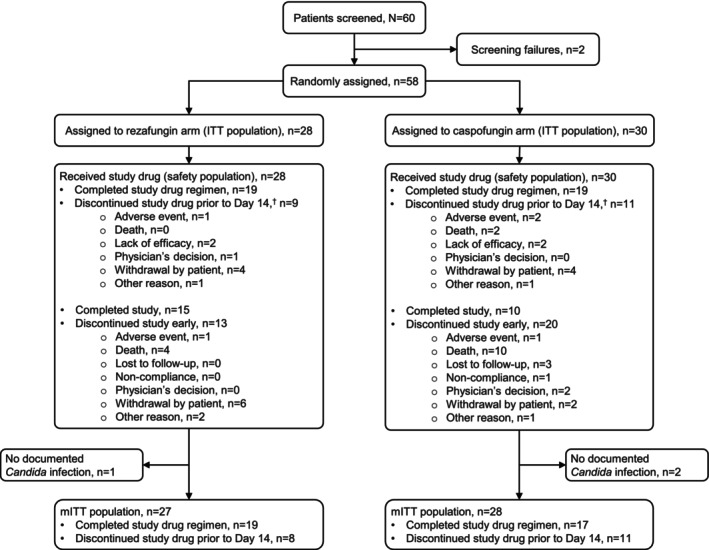 FIGURE 1
FIGURE 1| Characteristic | Treatment group | |
|---|---|---|
| Rezafungin 400/200 mg ( | Caspofungin 70/50 mg ( | |
| Age, | ||
| < 65 years | 18 (64.3) | 18 (60.0) |
| ≥ 65 years | 10 (35.7) | 12 (40.0) |
| Sex, | ||
| Male | 22 (78.6) | 16 (53.3) |
| Female | 6 (21.4) | 14 (46.7) |
| Race, | ||
| Asian | 28 (100.0) | 30 (100.0) |
| Final diagnosis, | ||
| Candidemia only | 26 (92.9) | 26 (86.7) |
| IC | 2 (7.1) | 4 (13.3) |
| Modified APACHE II score | ||
| Mean (SD) | 14.0 (6.1) | 14.4 (7.1) |
| Score ≥ 20, | 4 (14.3) | 6 (20.0) |
| Score < 20, | 23 (82.1) | 24 (80.0) |
| Mean body mass index, kg/m2 (SD) | 21.2 (3.5) | 22.2 (4.0) |
| Absolute neutrophil count, | ||
| < 500 cells/μL | 6 (21.4) | 6 (20.0) |
| ≥ 500 cells/μL | 22 (78.6) | 24 (80.0) |
| Mean estimated creatinine clearance, mL/min (SD) | 91.1 (88.1) | 75.6 (36.5) |
| Child–Pugh score, | ||
| < 7 | 0 | 0 |
| 7–9 | 1 (3.6) | 1 (3.3) |
| No history of liver disease/not calculated | 27 (96.4) | 29 (96.7) |
| Patients with ≥ 1 risk factor for | 28 (100) | 30 (100) |
| Central venous catheter | 9 (32.1) | 9 (30.0) |
| Peripherally inserted central catheter | 9 (32.1) | 11 (36.7) |
| Active malignancy | 6 (21.4) | 9 (30.0) |
| Broad‐spectrum antibiotic therapy | 22 (78.6) | 19 (63.3) |
| Diabetes mellitus | 3 (10.7) | 8 (26.7) |
| Immunosuppression | 8 (28.6) | 7 (23.3) |
| Major surgery | 5 (17.9) | 6 (20.0) |
| Total parenteral nutrition | 5 (17.9) | 9 (30.0) |
| Transplant recipient | 3 (10.7) | 0 |
| Trauma | 3 (10.7) | 1 (3.3) |
| End‐stage renal disease/dialysis | 2 (7.1) | 1 (3.3) |
| Burns | 0 | 1 (3.3) |
| Pancreatitis | 2 (7.1) | 2 (6.7) |
| Other | 12 (42.9) | 10 (33.3) |
| In ICU at time of randomisation, | 10 (35.7) | 13 (43.3) |
| Currently mechanically ventilated, | 6 (21.4) | 11 (36.7) |
| Dialysis within the previous 3 days, | 3 (10.7) | 2 (6.7) |
| Pancreatitis within the previous 10 days, | 2 (7.1) | 2 (6.7) |
|
| Treatment group, | |
|---|---|---|
| Rezafungin 400/200 mg ( | Caspofungin 70/50 mg ( | |
|
| 9 (33.3) | 9 (32.1) |
|
| 10 (37.0) | 8 (28.6) |
|
| 3 (11.1) | 3 (10.7) |
|
| 5 (18.5) | 6 (21.4) |
|
| 0 | 1 (3.6) |
|
| 0 | 1 (3.6) |
| Endpoint | Treatment group, | Treatment difference, % (95% CI) | |
|---|---|---|---|
| Rezafungin 400/200 mg ( | Caspofungin 70/50 mg ( | ||
| All‐cause mortality at Day 30 | |||
| Died or unknown survival status | 9 (33.3) | 10 (35.7) | −2.4 (−27.0–22.6) |
| Known to have died | 5 (18.5) | 7 (25.0) | |
| Unknown survival status | 4 (14.8) | 3 (10.7) | |
| Global response at Day 14, assessed by DRC | |||
| Cure | 13 (48.1) | 13 (46.4) | 0.3 (−25.4–26.3) |
| Failure | 11 (40.7) | 12 (42.9) | |
| Indeterminate | 3 (11.1) | 3 (10.7) | |
| Endpoint | Treatment group | ||
|---|---|---|---|
| Rezafungin 400/200 mg ( | Caspofungin 70/50 mg ( | Treatment difference, % (95% CI) | |
| Day 5 endpoints | |||
| Global cure, assessed by DRC, | 9 (33.3) | 10 (35.7) | −2.4 (−27.0–22.6) |
| Mycological eradication, | 19 (70.4) | 20 (71.4) | −1.1 (−25.1–22.9) |
| Investigator assessment of clinical cure, | 6 (22.2) | 6 (21.4) | 0.8 (−21.5–23.3) |
| Radiological cure, | 0/0 | 1/1 | — |
| Day 14 endpoints | |||
| Global cure, assessed by DRC, | 13 (48.1) | 13 (46.4) | 0.3 (−25.4–26.3) |
| Mycological eradication, | 17 (63.0) | 19 (67.9) | −4.9 (−29.5–20.1) |
| Investigator assessment of clinical cure, | 12 (44.4) | 15 (53.6) | −9.1 (−34.2–17.2) |
| Radiological cure, | 0/1 | 1/2 | −50.0 (−93.1–64.2) |
| Exploratory endpoint | |||
| Patients with negative blood culture, | |||
| At 24 h | 5/24 (20.8) | 4/24 (16.7) | — |
| At 48 h | 14/22 (63.6) | 12/23 (52.2) | — |
| TEAE | Treatment group, | |
|---|---|---|
| Rezafungin 400/200 mg ( | Caspofungin 70/50 mg ( | |
| Any TEAE | 27 (96.4) | 29 (96.7) |
| Study drug‐related TEAEs | 7 (25.0) | 8 (26.7) |
| SAE | 13 (46.4) | 17 (56.7) |
| Study drug‐related SAE | 0 | 0 |
| SAE leading to death | 7 (25.0) | 11 (36.7) |
| TEAE leading to study drug discontinuation | 1 (3.6) | 2 (6.7) |
| TEAE leading to study discontinuation | 4 (14.3) | 4 (13.3) |
| TEAEs in ≥ 10% of patients in either group | ||
| Hypokalaemia | 6 (21.4) | 7 (23.3) |
| Anaemia | 5 (17.9) | 2 (6.7) |
| Diarrhoea | 4 (14.3) | 2 (6.7) |
| Hyponatraemia | 4 (14.3) | 1 (3.3) |
| Pneumonia | 4 (14.3) | 5 (16.7) |
| Abdominal pain | 3 (10.7) | 1 (3.3) |
| Septic shock | 3 (10.7) | 4 (13.3) |
| Weight decreased | 3 (10.7) | 0 |
| Hypoalbuminaemia | 2 (7.1) | 4 (13.3) |
| Platelet count decreased | 2 (7.1) | 3 (10.0) |
| Pyrexia | 2 (7.1) | 3 (10.0) |
| Respiratory failure | 2 (7.1) | 3 (10.0) |
| Hypocalcaemia | 1 (3.6) | 5 (16.7) |
| Hypoproteinaemia | 1 (3.6) | 4 (13.3) |
- —Mundipharma Research Limited10.13039/100014471
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Fungal Infections and Studies · Cystic Fibrosis Research Advances
Introduction
1
It is estimated that, worldwide, there are > 1.5 million cases of candidemia and invasive candidiasis (IC) each year [1]. Most infections occur in hospitals, with an IC incidence of ~100 cases per 100,000 admissions; the highest incidence of IC is observed in intensive care units (ICUs) with 5.5–7.0 cases per 1000 admissions [2]. In China, the incidence of candidemia is reported to be 0.26–0.33 cases per 1000 admissions, and the incidence of IC to be 0.41 cases per 1000 admissions [3, 4, 5]. Furthermore, in ICUs in China, the incidence of IC is reported to be 32 cases per 1000 admissions, with a mortality rate of 37% [6].
Candida albicans is the most prevalent Candida species (spp.) globally. However, the prevalence of each Candida spp. varies geographically, and non‐ C. albicans spp. are reportedly becoming more common [7]. Three multicentre surveillance studies of IC in China described the four most prevalent Candida spp. to be C. albicans , C. parapsilosis , C. tropicalis and C. glabrata [8, 9, 10]. The introduction and transmission of C. auris across multiple provinces in China have also recently been reported [11].
Drug resistance, especially multidrug resistance, in Candida spp. is a growing problem, particularly in C. glabrata and C. auris [8, 11, 12, 13]. The increase in fluconazole resistance in C. parapsilosis also presents a global health risk [14, 15]. Echinocandins are among the preferred antifungal treatments for candidemia and IC in China and other countries [13, 16, 17]. These antifungals have not only excellent activity against most Candida spp., but also good tolerability and few drug–drug interactions [7]. However, most clinical data describing antifungal activity are obtained in Western countries and differences in the geographical prevalence of each Candida spp. (with non‐albicans Candida spp. being the predominant cause of over two‐thirds of cases of candidemia in China [10]) and their associated susceptibility to common antifungal drugs, including azoles and echinocandins, mean that data obtained in one region of the world may not always be applicable to another.
Rezafungin is a next‐generation echinocandin that has recently been approved for the treatment of adults with candidemia and/or IC in the United States, Europe, Brazil and the UAE [18, 19, 20, 21]. This novel echinocandin has distinctive pharmacokinetic characteristics that differentiate it from other echinocandins. These characteristics include a low clearance rate and an extended half‐life, which enable once‐weekly dosing. Weekly dosing results in high, front‐loaded exposures that may maximise the effect of rezafungin early in the treatment course, therefore increasing its antimicrobial effect [22, 23, 24]. In addition, rezafungin is active against various Candida spp., including strains resistant to azoles and some with isolates resistant to the other echinocandins [22, 25, 26].
The efficacy and safety of rezafungin in the treatment of candidemia and IC have been demonstrated in the Phase 2 STRIVE (NCT02734862) and Phase 3 ReSTORE (NCT03667690) trials [27, 28]. In ReSTORE, which was conducted in 15 countries, including China, rezafungin was shown to be noninferior to caspofungin for all‐cause mortality (ACM) at Day 30 and global cure at Day 14 [28]. To fulfill regulatory requirements for drug marketing authorisation in China and allow enrichment of the ReSTORE data with isolates from a region that had limited representation in the original trial, additional patients were recruited to an extended China‐only phase. Data from the ReSTORE China cohort, comprising participants from China who enrolled in the original ReSTORE trial and participants from the extended China‐only phase, are reported herein.
Patients and Methods
2
Study Design and Participants
2.1
ReSTORE was a global multicentre, double‐blind, randomised, Phase 3, noninferiority trial. Full methodological details have been reported [28]. ReSTORE China comprised participants from China who enrolled in the original ReSTORE trial (n = 11) and participants from an extended China‐only phase (n = 47).
Eligible patients were adults with systemic signs of candidemia and/or IC plus mycological evidence of infection (based on baseline blood or sterile site specimen cultures collected ≤ 96 h before randomisation) (see the Supporting Information for key eligibility criteria). Patients were randomised in a 1:1 ratio to receive either rezafungin or caspofungin. Rezafungin was administered intravenously (IV) at 400 mg on Day 1 and 200 mg on Day 8. Optional third and fourth doses of rezafungin at 200 mg were administered on Days 15 and 22, respectively, based on the investigator's judgment. Caspofungin was administered IV as a 70 mg loading dose on Day 1, followed by 50 mg/day for ≥ 3 days. After Day 3, patients meeting predefined criteria (e.g., stable clinical status, isolated Candida spp. susceptible to fluconazole, all signs and symptoms of candidemia/IC resolved, most recent blood culture negative for Candida spp., and no evidence of moderate‐to‐severe hepatic injury (see the Supporting Information) [28]) could switch to oral stepdown therapy (placebo for patients who received rezafungin, fluconazole 200–800 mg/day for patients who received caspofungin). The overall treatment duration was 14–28 days. Assessments are described in the Supporting Information.
Ethics Statement
2.2
The authors confirm that the ethical policies of the journal, as noted on the journal's author guidelines page, were adhered to and the appropriate ethical review committee approvals were received. ReSTORE was conducted in accordance with current regulations, the International Conference on Harmonisation Good Clinical Practice guidelines and the Declaration of Helsinki. The protocol was subject to approval by ethics committees or institutional review boards at participating sites. Patients provided written informed consent.
Endpoints
2.3
The primary efficacy endpoints were ACM at Day 30 and global cure at Day 14. Secondary efficacy endpoints included global cure at Day 5, and mycological eradication, clinical cure and radiological cure (for patients with IC) at Day 5 and 14. Exploratory efficacy endpoints were the proportion of patients with a negative blood culture at 24 and 48 h post first dose and time to first negative blood culture. These endpoints are defined in the Supporting Information. Additional exploratory endpoints in the China cohort were duration of hospital and intensive care unit (ICU) admissions and readmissions.
Treatment‐emergent adverse events (TEAEs) were recorded and coded using the Medical Dictionary for Regulatory Activities (MedDRA) version 23.0. Safety was also evaluated through physical examination findings, vital signs, laboratory tests and electrocardiogram results.
Statistical Analysis
2.4
From a clinical perspective (to assess efficacy and safety in patients from China who may present with distinct pathogenic strains and drug susceptibility) and independent of any statistical considerations, the regulatory authorities in China requested that a certain proportion of the overall ReSTORE study population (from the original ReSTORE trial and the extended China‐only phase) should be from China.
In the China cohort, primary and secondary efficacy endpoints were evaluated in the modified intent‐to‐treat (mITT) population using a two‐sided 95% confidence interval (CI) for the difference between the rezafungin and the caspofungin group (rezafungin – caspofungin), calculated using Miettinen and Nurminen methodology. For endpoints adjusted based on the randomisation strata, Cochran–Mantel–Haenszel weights were applied. Noninferiority was not tested as this is a subgroup of the primary study. Time to negative blood culture was analysed using Kaplan–Meier methods. Descriptive statistics were used to summarise safety endpoints in the safety population.
Study populations are defined in Supporting Information. All analyses were conducted using SAS version 9.4 or higher.
Results
3
Patients
3.1
Between October 12, 2018, and March 31, 2024, 60 patients with candidemia and/or IC from China were screened; 58 patients who met the eligibility criteria for the study were randomised and included in the intent‐to‐treat (ITT) population (rezafungin n = 28, caspofungin n = 30) (Figure 1). All 58 patients received ≥ 1 dose of the study treatment and were included in the safety population (rezafungin n = 28; caspofungin n = 30). Fifty‐five patients were included in the mITT population (rezafungin n = 27; caspofungin n = 28; as defined in the Supporting Information) that was used for the efficacy analyses.
Patient disposition. The disposition and flow of patients in the study are shown, including screening, randomisation, study (drug) discontinuation, study completion and analysis populations. †Patients who discontinued the study drug prior to Day 14 did not have to discontinue the study; they may have continued in the study for the safety analysis. ITT, intent‐to‐treat; mITT, modified intent‐to‐treat.
Patient baseline characteristics were similar between the two treatment groups (Table 1). The majority of patients had a modified Acute Physiology and Chronic Health Evaluation (APACHE) II score of < 20 (rezafungin 82.1% [23/28], caspofungin 80.0% [24/30]), an absolute neutrophil count (ANC) of ≥ 500 cells/μL (rezafungin 78.6% [22/28], caspofungin 80.0% [24/30]), and a final diagnosis of candidemia only (rezafungin 92.9% [26/28], caspofungin 86.7% [26/30]). In the mITT population, of patients with candidemia only, 73.1% (19/26) in the rezafungin group and 66.7% (18/27) in the caspofungin group had a catheter present at screening (Table S1).
The Candida spp. present in the blood and sterile site cultures were balanced between the two treatment groups at baseline (Table 2). C. albicans and C. tropicalis were the most common spp. present. The minimum inhibitory concentration range for rezafungin by baseline Candida spp. (analysed post hoc) is shown in Table S2.
Treatment Exposure
3.2
In the safety population, the median duration of study drug exposure in patients receiving intravenous (IV) therapy only (rezafungin or caspofungin) was 14.0 days in both the rezafungin and the caspofungin group (interquartile range [IQR] 6.0–17.5 and 7.0–15.0, respectively). During the study period, three (10.7%) patients in the rezafungin group and seven (23.3%) in the caspofungin group who met predefined criteria switched to oral stepdown therapy (placebo for patients who received rezafungin, fluconazole for patients who received caspofungin) for a median duration of 10.0 days (IQR 8.0–12.0) and 6.0 days (IQR 6.0–7.0), respectively. The median duration of IV and oral therapy combined was 14.0 days for both rezafungin (IQR 6.0–19.0) and caspofungin (IQR 7.0–21.0).
Primary Endpoints
3.3
This study had two primary endpoints: ACM at Day 30 and global cure at Day 14 in the mITT population. At Day 30, 33.3% (9/27) of patients in the rezafungin group and 35.7% (10/28) in the caspofungin group were deceased or had an unknown survival status (treatment difference for ACM at Day 30 –2.4% [95% CI −27.0–22.6]) (Table 3). Global cure at Day 14 was observed in 48.1% (13/27) of patients in the rezafungin group and 46.4% (13/28) in the caspofungin group (weighted treatment difference 0.3% [95% CI −25.4–26.3]) (Table 3).
Secondary and Exploratory Efficacy Endpoints
3.4
The secondary efficacy endpoints included global cure at Day 5 and mycological eradication at Day 5 and 14 in the mITT population. Exploratory efficacy endpoints were the proportion of patients with a negative blood culture at 24 and 48 h post first dose, and time to first negative blood culture.
Global cure at Day 5 was seen in 33.3% (9/27) of patients in the rezafungin group and 35.7% (10/28) in the caspofungin group (treatment difference −2.4% [95% CI −27.0–22.6]) (Table 4). Mycological eradication at Day 5 was seen in 70.4% (19/27) of patients in the rezafungin group and 71.4% (20/28) in the caspofungin group. At Day 14, mycological eradication was seen in 63.0% (17/27) and 67.9% (19/28) of patients in the rezafungin group and the caspofungin group, respectively (Table 4).
At 24 h, the proportion of patients with a negative blood culture was 20.8% (5/24) in the rezafungin group and 16.7% (4/24) in the caspofungin group. At 48 h, the proportions were 63.6% (14/22) and 52.2% (12/23), respectively (Table 4). The median time to first negative blood culture was 46.4 h (95% CI 32.4–90.3) in the rezafungin group and 48.9 h (95% CI 37.8–94.3) in the caspofungin group.
Exploratory Analyses of Hospital and Intensive Care Unit Admissions
3.5
In the mITT population, in patients who remained alive during hospitalisation (n = 23 in both treatment groups), the median duration of hospital stay across all admissions was 25.0 days (IQR 16.0–45.0) in the rezafungin group and 21.0 days (IQR 15.0–31.0) in the caspofungin group. The median duration of ICU admission was 10.0 days (IQR 6.0–24.0; n = 9) and 10.5 days (IQR 4.0–22.0; n = 6) in the rezafungin and the caspofungin group, respectively. Two (7.4%) patients receiving rezafungin and four (14.3%) patients receiving caspofungin were newly admitted to the ICU on or after Day 1 of the study.
None of the patients discharged from hospital before Day 30 was readmitted by Day 30. By follow‐up (Days 52–59), 4.5% (1/22) of patients discharged on or after Day 1 in the rezafungin group and 9.5% (2/21) in the caspofungin group had been readmitted. Of the patients admitted to the ICU during their initial hospitalisation and subsequently discharged from the ICU before Day 30, 10.0% (1/10) in the rezafungin group and 22.2% (2/9) in the caspofungin group were readmitted to the ICU by Day 30. By follow‐up, 9.1% (1/11) of patients in the rezafungin group and 30.0% (3/10) in the caspofungin group were readmitted to the ICU.
In a post hoc analysis, study investigators indicated that they would have considered discharging 9.1% (5/55) of patients sooner if once‐weekly IV rezafungin had been available (11.1% [3/27] of patients in the rezafungin group and 7.1% [2/28] in the caspofungin group).
Safety
3.6
In the safety population, TEAEs were experienced by 96.4% (27/28) of patients in the rezafungin group and 96.7% (29/30) in the caspofungin group (Table 5). The most common TEAE, experienced by > 20% of patients in both treatment groups, was hypokalaemia. Study drug‐related TEAEs were reported in 25.0% (7/28) and 26.7% (8/30) of patients in the rezafungin and the caspofungin group, respectively; none led to study drug discontinuation. Study drug‐related TEAEs that were reported in > 1 patient were raised alanine aminotransferase (rezafungin 7.1% [2/28], caspofungin 3.3% [1/30]), hypokalaemia (rezafungin 3.6% [1/28], caspofungin 6.7% [2/30]) and diarrhoea (rezafungin 0.0%, caspofungin 6.7% [2/30]) (Table S3). TEAEs led to study drug discontinuation in 3.6% (1/28) and 6.7% (2/30) of patients in the rezafungin and the caspofungin group, respectively. TEAEs that led to study drug discontinuation were respiratory failure (rezafungin group), Aspergillus infection (caspofungin group) and pneumonia (caspofungin group).
Serious adverse events (SAEs) were experienced by 46.4% (13/28) of patients in the rezafungin group and 56.7% (17/30) in the caspofungin group. In the rezafungin group, SAEs that were reported in > 1 patient were gastrointestinal haemorrhage (7.1% [2/28]), multiple organ dysfunction syndrome (7.1% [2/28]) and sepsis (7.1% [2/28]). In the caspofungin group, SAEs that were reported in > 1 patient were septic shock (13.3% [4/30]) and pneumonia (6.7% [2/30]). No study drug‐related SAEs were reported.
Discussion
4
Although formal inferential statistical analysis was not undertaken, data from the ReSTORE China cohort (herein referred to as the China cohort) of patients with candidemia and IC suggested that rezafungin and caspofungin have similar efficacy with respect to the primary (ACM at Day 30 and global cure at Day 14), secondary (including global cure at Day 5 and mycological eradication at Days 5 and 14) and exploratory endpoints (including time to negative blood culture, duration of hospital/ICU admissions and readmissions). Rezafungin had a comparable safety and tolerability profile to caspofungin. For both rezafungin and caspofungin, the nature, intensity and seriousness of TEAEs were consistent with those reported in the primary analysis of the ReSTORE trial and the Phase 2 STRIVE trial [27, 28], as well as their established safety profiles [18, 19, 29].
In the China cohort, both ACM at Day 30 and global cure at Day 14 were comparable between the treatment groups; this is in accordance with the findings of the primary ReSTORE analysis (herein referred to as the primary analysis), in which rezafungin was shown to be noninferior to caspofungin for these primary endpoints [28]. For ACM at Day 30, the treatment difference (rezafungin − caspofungin) was 2.4% (95% CI −9.7–14.4) in the primary analysis [28] and −2.4% (95% CI −27.0–22.6) in the China cohort. For global cure at Day 14, the weighted treatment difference was −1.1% (95% CI −14.9–12.7) in the primary analysis and 0.3% (95% CI −25.4–26.3) in the China cohort.
Despite the similarity between the two treatment groups in the primary endpoints, higher overall Day 30 ACM rates and lower Day 14 global cure rates were observed in the China cohort than in the primary analysis [28]. We believe that several factors may have contributed to this finding. A higher proportion of patients in the China cohort (14.8% and 10.7% of patients in the rezafungin and caspofungin groups, respectively) than in the primary analysis (3.2% of patients in each group) had unknown survival status at Day 30. Given that patients with unknown survival status were considered deceased for the purposes of calculating ACM, the higher incidence in the China cohort is likely to have inflated the mortality rate; this is probably compounded by the smaller sample size. The higher Day 30 ACM rates and lower Day 14 global cure rates in the China cohort may also be related to the observed ANC levels and APACHE II scores, with both being indicators of more severe disease. A higher proportion of patients in the China cohort than in the primary analysis had ANC levels of < 500 cells/μL (respective proportions were 21.4% vs. 9.0% for rezafungin and 20.0% vs. 6.1% for caspofungin) and a higher mean modified APACHE II score (respective mean scores were 14.0 vs. 12.5 for rezafungin and 14.4 vs. 13.1 for caspofungin) [28]. In addition, the data may have been affected by the different Candida spp. present in the two study populations (and consequently different echinocandin susceptibility profiles), which could reflect geographical variations in prevalence [7, 8, 9, 11].
Results from the primary analysis suggested that there were potential early treatment benefits for rezafungin versus caspofungin. This was indicated by a shorter median time to first negative blood culture (23.9 h vs. 27.0 h, respectively), higher proportion of patients with negative blood culture at 24 h (53.7% vs. 46.2%, respectively) and 48 h (74.2% vs. 64.1%, respectively), and higher rate of mycological eradication at Day 5 (treatment difference 7.1% [95% CI −6.6–20.6]) in the rezafungin group than the caspofungin group [28]. The median time to first negative blood culture was numerically longer in the China cohort (rezafungin 46.4 h, caspofungin 48.9 h) than in the primary analysis, with a less pronounced difference between the two treatment groups. There was also little difference between the treatment groups in the rate of mycological eradication at Day 5 (−1.1% [95% CI −25.1–22.9]) in the China cohort; however, rates in both groups were similar to those in the primary analysis. Possible explanations for the differences between the China cohort and the primary analysis could include the smaller sample size in the China cohort (making it more difficult to accurately detect differences), differences in baseline characteristics (e.g., ethnicity, infection type, ANC levels, Candida risk factors and catheter placement/removal), and the distribution of Candida spp. between the two populations.
A population pharmacokinetic model has been reported for rezafungin, which was developed using data from healthy participants, hepatically impaired patients and patients with candidemia and/or IC [30]. Covariate analysis did not identify any patient factors that were associated with clinically meaningful changes in rezafungin pharmacokinetics, indicating that a common dose regimen is adequate for all adult patients. An update to the population pharmacokinetic model to include pharmacokinetic data from patients in the ReSTORE China extension study enabled assessment of rezafungin exposure in patients from China and comparison with the non‐China cohort [31]. The analysis showed no clinically meaningful differences in rezafungin exposure parameters between patients from China and patients from elsewhere, supporting a lack of requirement for dose adjustments in patients from China [31].
Given the geographical variation in the prevalence and patterns of Candida spp. and antifungal resistance [7], extension cohorts, such as this one, are important because they provide region‐specific data that can be used to tailor treatment strategies to the local clinical landscape, in this case, in China. Although the small sample in the China cohort prohibited formal statistical analysis, the efficacy and safety findings were consistent with those for the main primary analysis, providing confidence in the findings. No separate hypothesis was formulated for the extension cohort, which was conducted specifically to meet regulatory requirements for evaluating efficacy and safety in a sample of patients from China. In the future, real‐world post‐marketing studies will further evaluate the effectiveness and safety of rezafungin in patients from China, while antimicrobial susceptibility testing results of isolates will be monitored to enrich the dataset and capture regional variations in pathogen distribution and antifungal resistance. In addition to the small sample size, limitations reported for the original ReSTORE trial apply here also, such as the exclusion of children and patients with specific forms of IC [28].
In this ReSTORE China cohort, rezafungin demonstrated comparable efficacy and safety to caspofungin in patients with candidemia or IC. These findings support the primary analysis of the Phase 3 ReSTORE trial and suggest that rezafungin could provide a new treatment option for candidemia and/or IC in China.
Author Contributions
Haihui Huang: data curation, investigation, project administration, resources, supervision, validation, writing – review and editing. Sizhou Feng: data curation, investigation, project administration, resources, writing – review and editing. Yunsong Yu: data curation, investigation, project administration, resources, writing – review and editing. Yong Zhang: data curation, investigation, project administration, resources, writing – review and editing. Yuan Yuan: data curation, investigation, project administration, resources, writing – review and editing. Laura Cox: data curation, investigation, project administration, resources, writing – review and editing. Yingyuan Zhang: conceptualisation, data curation, investigation, methodology, project administration, resources, supervision, validation, writing – review and editing.
Conflicts of Interest
Yingyuan Zhang, Haihui Huang, Sizhou Feng, Yunsong Yu, Yong Zhang and Yuan Yuan report no conflicts of interest. Laura Cox is an employee of Mundipharma Research Ltd.
Supporting information
Data S1: myc70122‐sup‐0001‐DataS1.pdf.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1D. W. Denning , “Global Incidence and Mortality of Severe Fungal Disease,” Lancet Infectious Diseases 24 (2024): e 428–e 438, 10.1016/s 1473-3099(23)00692-8.38224705 · doi ↗ · pubmed ↗
- 2C. Lass‐Flörl , S. S. Kanj , N. P. Govender , G. R. Thompson , L. Ostrosky‐Zeichner , and M. A. Govrins , “Invasive Candidiasis,” Nature Reviews Disease Primers 10 (2024): 20, 10.1038/s 41572-024-00503-3.38514673 · doi ↗ · pubmed ↗
- 3Z. Zeng , Y. Ding , G. Tian , et al., “A Seven‐Year Surveillance Study of the Epidemiology, Antifungal Susceptibility, Risk Factors and Mortality of Candidaemia Among Paediatric and Adult Inpatients in a Tertiary Teaching Hospital in China,” Antimicrobial Resistance and Infection Control 9 (2020): 133, 10.1186/s 13756-020-00798-3.32799915 PMC 7429891 · doi ↗ · pubmed ↗
- 4L. Chen , Z. Xie , and J. Jian , “Epidemiology and Risk Factors of Candidemia a 8‐Year Retrospective Study From a Teaching Hospital in China,” Infection and Drug Resistance 17 (2024): 3415–3423, 10.2147/idr.S 471171.39131515 PMC 11317046 · doi ↗ · pubmed ↗
- 5Z. R. Zeng , G. Tian , Y. H. Ding , K. Yang , J. B. Liu , and J. Deng , “Surveillance Study of the Prevalence, Species Distribution, Antifungal Susceptibility, Risk Factors and Mortality of Invasive Candidiasis in a Tertiary Teaching Hospital in Southwest China,” BMC Infectious Diseases 19 (2019): 939, 10.1186/s 12879-019-4588-9.31699043 PMC 6836498 · doi ↗ · pubmed ↗
- 6F. Guo , Y. Yang , Y. Kang , et al., “Invasive Candidiasis in Intensive Care Units in China: A Multicentre Prospective Observational Study,” Journal of Antimicrobial Chemotherapy 68 (2013): 1660–1668, 10.1093/jac/dkt 083.23543609 · doi ↗ · pubmed ↗
- 7P. G. Pappas , M. S. Lionakis , M. C. Arendrup , L. Ostrosky‐Zeichner , and B. J. Kullberg , “Invasive Candidiasis,” Nature Reviews Disease Primers 4 (2018): 18026, 10.1038/nrdp.2018.26.29749387 · doi ↗ · pubmed ↗
- 8M. Xiao , Z. Y. Sun , M. Kang , et al., “Five‐Year National Surveillance of Invasive Candidiasis: Species Distribution and Azole Susceptibility From the China Hospital Invasive Fungal Surveillance Net (CHIF‐NET) Study,” Journal of Clinical Microbiology 56 (2018): e 00577−18, 10.1128/jcm.00577-18.29743305 PMC 6018329 · doi ↗ · pubmed ↗