Clinical Spectrum of Xeroderma Pigmentosum: An Observational Study
Usha Sri Akkineni, Dilip Chandra Chintada, Kirankanth Vudayana, Pooja Unnikrishnan

TL;DR
This study examines the varied symptoms and cancers in xeroderma pigmentosum patients, emphasizing the need for early diagnosis and sun protection.
Contribution
The study provides a detailed observational analysis of XP's clinical spectrum, including mucocutaneous and extracutaneous malignancies.
Findings
XP patients showed 100% poikiloderma and 80% freckles, with 20% neurological involvement.
Common malignancies included squamous cell and basal cell carcinomas, along with extracutaneous cancers like sarcoma and stomach carcinoma.
Early onset under one year was observed in 70% of cases, highlighting the importance of early diagnosis and cancer screening.
Abstract
Background Xeroderma pigmentosum (XP) is an uncommon condition caused by impaired UV radiation-induced damage repair. It is brought on by deficiencies in either post-replication repair or nucleotide excision repair, which can result in neurological, ophthalmic, and cutaneous problems. With a focus on mucocutaneous symptoms, associated malignancies, and systemic involvement, this study aims to record and examine the diverse clinical presentations of XP. Methodology A total of 10 clinically diagnosed XP patients participated in this 12-month prospective observational study conducted at a tertiary care center between April 2024 and April 2025. A comprehensive history, consent, and a dermatological, ophthalmic, neurological, and systemic examination were obtained. Results Of the 10 cases, there were four (40%) female and 6 (60%) male cases. The age of onset was less than one year in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1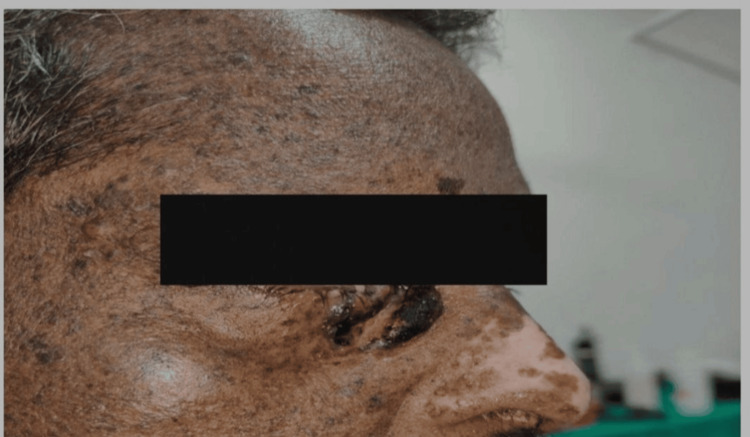 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4 Figure 5
Figure 5| Features | Clinical features | Number of cases | Percentage |
| Skin features | Poikiloderma | 10 | 100 |
| Freckles | 8 | 80 | |
| Xerosis | 8 | 80 | |
| Lentigenes | 6 | 60 | |
| Skin atrophy | 6 | 60 | |
| Seborrheic keratosis | 4 | 40 | |
| Nevi | 3 | 30 | |
| Actinic keratosis | 2 | 20 | |
| Ocular features | Photophobia | 7 | 70 |
| Conjunctival xerosis | 6 | 60 | |
| Cataract | 5 | 50 | |
| Neurological features | Speech delay, gait disturbances | 2 | 20 |
| Mucocutaneous malignancies and extracutaneous malignancies | Squamous cell carcinoma | 2 | 20 |
| Basal cell carcinoma | 3 | 30 | |
| Lip carcinoma | 1 | 10 | |
| Tongue carcinoma | 1 | 10 | |
| Buccal cavity carcinoma | 2 | 20 | |
| Eyelid carcinoma | 1 | 10 | |
| Stomach carcinoma | 1 | 10 | |
| Sarcoma | 1 | 10 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
Topicsmelanin and skin pigmentation · RNA regulation and disease · DNA Repair Mechanisms
Introduction
Xeroderma pigmentosum (XP) is a rare autosomal recessive disease with 100% penetrance, caused by mutations in any of eight genes. The products of seven of these (XP-A through G) participate in the nucleotide excision repair mechanism, which fixes UV-induced photoproducts in DNA. Replication of DNA with unrepaired damage requires the eighth gene (XPV). It affects individuals across all racial groups and continents. Both men and women are equally impacted. It is characterized by a high sensitivity to sunlight, which can lead to sunburn, changes in skin pigmentation, and a significantly higher risk of developing skin cancer [1]. Skin atrophy, seborrheic keratosis, actinic keratosis, lentiginous pigmentation, photosensitivity, and seborrheic warts are common cutaneous features of the disease.
Ocular abnormalities, resulting from UV-induced DNA modification in conjunctival, corneal, and eyelid epithelial cells, are present in approximately 40% to 80% of patients with XP. Photophobia, severe keratitis, corneal opacification, and vascularization are its defining characteristics. About 20-30% of patients experience neurological issues, which can start anywhere from the age of two to middle life. These include spasticity, sensorineural deafness, convulsions, and intellectual disability [2].
Patients with XP are 1,000 times more likely to develop skin cancers in sun-exposed areas. The most prevalent kind is basal cell carcinoma (BCC), followed by malignant melanoma and squamous cell carcinoma (SCC). The incidence of other systemic cancers, such as breast, uterine, pancreatic, gastric, and mucosal carcinomas, is 10-20 times greater in XP [3].
Although the condition is ultimately fatal, lifespan can be extended by taking simple precautions to limit sun exposure. Extensive UV radiation-induced skin and eye damage in XP patients is indicative of a lack of awareness of the disease’s deadly nature, which leads to XP neglect [4]. With a focus on mucocutaneous symptoms, other features such as malignancies and systemic features have been described in this study.
Materials and methods
Study design
A prospective, observational, pilot study was conducted over a 12-month period from April 2024 to April 2025 in the Department of Dermatology, after obtaining approval from the Institutional Ethics Committee, Great Eastern Medical School and Hospital (approval number: 09/IEC/GEMS&H/2025). The primary objective was to document and analyze the spectrum of clinical manifestations of XP, with a focus on mucocutaneous symptoms, related cancers, and systemic involvement.
Study population
The study included 10 consecutive patients with a confirmed clinical diagnosis of XP, irrespective of age and sex, who attended the dermatology outpatient clinic during the study period and were willing to provide consent. Patients with inadequate follow-up and those with photodermatoses or genodermatoses mimicking XP, where diagnosis could not be confirmed, were excluded.
Data collection
All patients underwent a detailed clinical evaluation and provided a comprehensive clinical history focusing on age of onset, gender, consanguinity, and symptom progression after providing written informed consent. Evaluation of pigmentation, freckling, skin malignancies, and atrophy was part of the dermatological examination. Relevant specialists performed neurological and ocular tests. Whenever feasible, dermoscopy and clinical imaging were employed. Laboratory investigations were performed to assess systemic involvement, and the data were compiled and tabulated.
Statistical analysis
Demographic characteristics, clinical presentations, and systemic findings were summarized descriptively. Data were analyzed using the OpenEpi software to provide a comprehensive overview of disease patterns within the study population.
Results
Of the 10 patients included in the study, six (60%) were male and four (40%) were female. Seven cases (70%) had an age of onset before one year, followed by two (20%) cases between one and two years, and one (10%) case above two years. Consanguinity in marriage was found in four (40%) cases.
Skin abnormalities included poikiloderma (Figure 1) in 10 (100%) cases, freckles in eight (80%) cases, xerosis in eight (80%) cases, lentigenes in six (60%) cases, skin atrophy in six (60%) cases, seborrheic keratosis in four (40%) cases, nevi in three (30%) cases, and actinic keratosis in two (20%) cases.
Clinical presentation of poikiloderma over the anterior trunk.
Overall, two (20%) cases out of 10 had neurological symptoms, such as delayed speech and abnormal gait. Further, seven (70%) cases had photophobia, six (60%) cases had conjunctival xerosis, and five (50%) cases had cataracts. However, among the mucocutaneous cancers, three (30%) cases had BCC (Figure 2), two (20%) cases had SCC, one (10%) case had eyelid carcinoma, one (10%) case had lip carcinoma (Figure 3), one (10%) cases had tongue carcinoma (Figure 4), and two (20%) cases had buccal cavity carcinoma (Table 1).
Clinical presentation of basal cell carcinoma near the right medial canthus.
Clinical image of carcinoma of the upper lip in a patient with xeroderma pigmentosum.
Clinical image of carcinoma of the tongue in a patient with xeroderma pigmentosum.
Among the extracutaneous cancers, one (10%) cases had sarcoma (Figure 5), and one (10%) case had stomach carcinoma.
Clinical image showing sarcoma below the posterior aspect of the neck.
Discussion
This study included 10 clinically diagnosed XP cases, reinforcing the multisystem nature of the disease and highlighting uncommon findings such as gastrointestinal and mucosal cancers in Indian patients.
Demographic profile
Overall, seven (70%) cases in our analysis had a mean age of onset during the first year of life, which is consistent with findings by DiGiovanna and Kraemer (2012) [5], who found that cumulative UV exposure tends to cause initial skin alterations by the time a child is six months to three years old. Similar to the research by Halkud et al. (2014) [6], the male-to-female ratio (1.5:1) indicated no sex preference but rather a potentially greater detection rate among male youngsters because of increased solar exposure in rural areas.
Cutaneous manifestations
Poikiloderma, freckles, and xerosis were among the most common cutaneous symptoms detected in more than eight (80%) patients, which is comparable with the findings of Cleaver et al. (2009), who found these traits in 80-90% of cases [7].
Ocular manifestations
Ocular symptoms such as conjunctival xerosis, photophobia, and cataract were observed in seven (70%) patients. These findings are consistent with those reported by Brooks et al. (2013) [8], who found ocular involvement in more than two-thirds of XP patients, demonstrating that UV damage is not limited to the skin.
Neurological manifestations
Overall, two (20%) cases had neurological symptoms, such as cognitive impairment and speech delay. This is similar to the findings of Kraemer et al. (2003) [9] and Bradford et al. (2011) [10], who observed neurological symptoms in 20-30% of the XP-A and XP-D complementation groups. However, due to limited access to genetic typing, we were unable to classify our patients based on the complementation group.
Cutaneous malignancies
A notable characteristic of our study was the occurrence of cutaneous malignancies in five (50%) patients, including BCC in three (30%) and SCC in two (20%) cases, beginning as early as the second decade. This is consistent with the study reported by Aneja et al. (2025) [11], who found that XP patients have a >10,000-fold higher risk of non-melanoma skin cancer before the age of 20 than the general population.
Mucosal and internal malignancies
A notable characteristic of this series was the documentation of non-cutaneous cancers, which included mucosal malignancies such as lip, tongue, and buccal mucosa in a few individuals. Baskurt et al. (2024) previously described mucosal tumors in pediatric XP patients [12], notwithstanding their rarity. Additionally, gastric cancer was seen in one patient, an extremely unusual indication previously reported by Li et al. (2000) and hypothesized to result from worldwide DNA repair defects affecting the gastrointestinal mucosa [13]. Our findings highlight the importance of complete systemic surveillance in XP patients beyond dermatological follow-up. Our findings are consistent with previous XP literature regarding the frequency of cutaneous malignancies. However, the occurrence of mucosal and visceral tumors in two patients, while noteworthy, should be interpreted cautiously, given the small sample size and potential reporting bias.
Association with sarcoma
One (10%) patient had sarcoma, a finding that has been very rarely reported in the literature. While most likely coincidental, this observation may reflect a broader embryological disruption of developmental instability in XP patients and merits further assessment. Unlike many Western studies that utilize genetic profiling, our lack of complementation group typing limits the ability to establish direct genotype-phenotype correlations. However, the phenotypic diversity observed between patients reflects a varied genetic background, which may have been influenced by consanguinity, as seen in four (40%) cases. This is consistent with the research of Ijaz et al. (2019), who described a frequent trait in various Indian and Middle Eastern cohorts [14].
Management
Strict and consistent sun avoidance and protection and early detection and treatment of premalignant and malignant skin lesions are the mainstays of management [15]. Surgical removal of cancerous lesions and the use of antioxidants are considered to be effective against this disease [16]. Counselling on photoprotection, genetic counseling, and psychosocial support were given to all patients. Sun avoidance, UV-blocking clothing, and sunscreens were included in the management along with regular dermatological, ophthalmological, and neurological checkups.
Limitations
The lack of molecular or genetic subtyping, which would improve comprehension of phenotype-genotype connections, and the small sample size are the limitations of this study. Although malignancies were documented clinically, none of the cases had complete histologic confirmation. Standardized outcome measures and long-term follow-up were not feasible, which may limit the generalizability of the findings. Despite these constraints, the study provides valuable insight into the clinical variability and disease burden of XP in an underreported population.
Conclusions
This study highlights the clinical spectrum of XP in an underreported population and suggests possible variation in malignancy patterns. For early detection and management of XP in India, our findings underscore the need for national guidelines, increased awareness, and vigilant clinical monitoring. Early genetic counseling can help families understand recurrence risk and enable informed reproductive choices, especially in populations with higher rates of consanguinity. Establishing multicenter registries and enabling wider access to genetic testing in the future can help improve outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Xeroderma pigmentosum Orphanet J Rare Dis Lehmann AR Mc Gibbon D Stefanini M 70620112204460710.1186/1750-1172-6-70PMC 3221642 · doi ↗ · pubmed ↗
- 2Xeroderma pigmentosum: man deprived of his right to light Scientific World Journal Mareddy S Reddy J Babu S Balan P 534752201320132445943510.1155/2013/534752 PMC 3891433 · doi ↗ · pubmed ↗
- 3Xeroderma pigmentosum and the role of UV-induced DNA damage in skin cancer Mol Med Today van Steeg H Kraemer KH 8694519991020095010.1016/s 1357-4310(98)01394-x · doi ↗ · pubmed ↗
- 4Cutaneous malignancies in xeroderma pigmentosum: earlier management improves survival Indian J Otolaryngol Head Neck Surg Naik SM Shenoy AM Nanjundappa A Halkud R Chavan P Sidappa K Gupta S 1621676520132442755810.1007/s 12070-012-0614-6PMC 3649029 · doi ↗ · pubmed ↗
- 5Shining a light on xeroderma pigmentosum J Invest Dermatol Di Giovanna JJ Kraemer KH 78579613220122221773610.1038/jid.2011.426PMC 3279615 · doi ↗ · pubmed ↗
- 6Xeroderma pigmentosum: clinicopathological review of the multiple oculocutaneous malignancies and complications Indian J Surg Oncol Halkud R Shenoy AM Naik SM Chavan P Sidappa KT Biswas S 120124520142511446410.1007/s 13193-014-0307-6PMC 4116547 · doi ↗ · pubmed ↗
- 7Disorders of nucleotide excision repair: the genetic and molecular basis of heterogeneity Nat Rev Genet Cleaver JE Lam ET Revet I 7567681020091980947010.1038/nrg 2663 · doi ↗ · pubmed ↗
- 8Ocular manifestations of xeroderma pigmentosum: long-term follow-up highlights the role of DNA repair in protection from sun damage Ophthalmology Brooks BP Thompson AH Bishop RJ 1324133612020132360180610.1016/j.ophtha.2012.12.044PMC 3702678 · doi ↗ · pubmed ↗